
Colleges
- AAC
- ACC
- Big 12
- Big East
- Big Ten
- Pac-12
- SEC
- Atlantic 10
- Conference USA
- Independents
- Junior College
- Mountain West
- Sun Belt
- MAC
- More
- Navy
- UAB
- Tulsa
- UTSA
- Charlotte
- Florida Atlantic
- Temple
- Rice
- East Carolina
- USF
- SMU
- North Texas
- Tulane
- Memphis
- Miami
- Louisville
- Virginia
- Syracuse
- Wake Forest
- Duke
- Boston College
- Virginia Tech
- Georgia Tech
- Pittsburgh
- North Carolina
- North Carolina State
- Clemson
- Florida State
- Cincinnati
- BYU
- Houston
- Iowa State
- Kansas State
- Kansas
- Texas
- Oklahoma State
- TCU
- Texas Tech
- Baylor
- Oklahoma
- UCF
- West Virginia
- Wisconsin
- Penn State
- Ohio State
- Purdue
- Minnesota
- Iowa
- Nebraska
- Illinois
- Indiana
- Rutgers
- Michigan State
- Maryland
- Michigan
- Northwestern
- Arizona State
- Oregon State
- UCLA
- Colorado
- Stanford
- Oregon
- Arizona
- California
- Washington
- USC
- Utah
- Washington State
- Texas A&M
- Auburn
- Mississippi State
- Kentucky
- South Carolina
- Arkansas
- Florida
- Missouri
- Ole Miss
- Alabama
- LSU
- Georgia
- Vanderbilt
- Tennessee
- Louisiana Tech
- New Mexico State
- Middle Tennessee
- Western Kentucky
- UTEP
- Florida International University
High School
- West
- Midwest
- Northeast
- Southeast
- Other
- Alaska
- Arizona
- California
- Colorado
- Nevada
- New Mexico
- Northern California
- Oregon
- Southern California Preps
- Washington
- Edgy Tim
- Indiana
- Kansas
- Nebraska
- Iowa
- Michigan
- Minnesota
- Missouri
- Oklahoma Varsity
- Texas Basketball
- Texas
- Wisconsin
- Delaware
- Maryland
- New Jersey Basketball
- New Jersey
- New York City Basketball
- Ohio
- Pennsylvania
- Greater Cincinnati
- Virginia
- West Virginia Preps
ADVERTISEMENT
Install the app
How to install the app on iOS
Follow along with the video below to see how to install our site as a web app on your home screen.
Note: This feature may not be available in some browsers.
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
COVID-19 Pandemic: Transmissions, Deaths, Treatments, Vaccines, Interventions and More...
- Thread starter Richie O
- Start date
- Status
- Not open for further replies.
Just stop. There are plenty of article and studies that say masks help. Nobody says they are perfect. Bottom line is the measures we have taken in NJ have greatly reduced transmission. That is a fact. Cannot be argued. Again I have never really understood what you are arguing for. If it is literally gyms then maybe I get that. If it is to go back to normal then no way. Indoors should only be open with masks only. Restaurants not open indoors. Not yet. Have to wait another 4-6 months. I would say that if by the new year no vaccine or cure looms close then we might have to reconsider things.
did you bother to read the study...this is why i say virus going to virus
did you bother to read the study...this is why i say virus going to virus
No, you say that because you're a dope who falls for easy-to-remember slogans.

https://www.nj.com/union/2020/08/ma...ted-for-coronavirus-violation-police-say.html
Ugh. Who wants outdoor dining at a strip club?
Ugh. Who wants outdoor dining at a strip club?
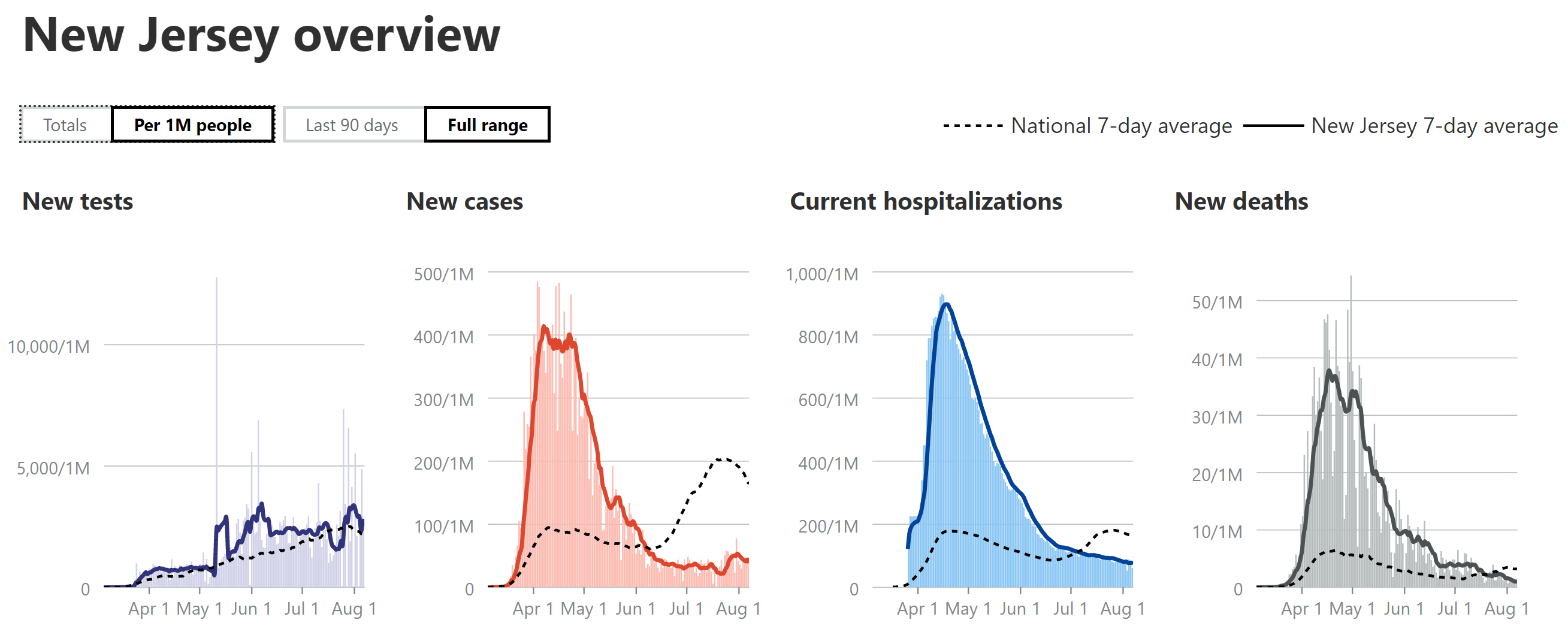
Am a day late, due to our power outage and don't have time for the full analysis of past weeks either, so just going with a summary...
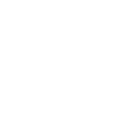
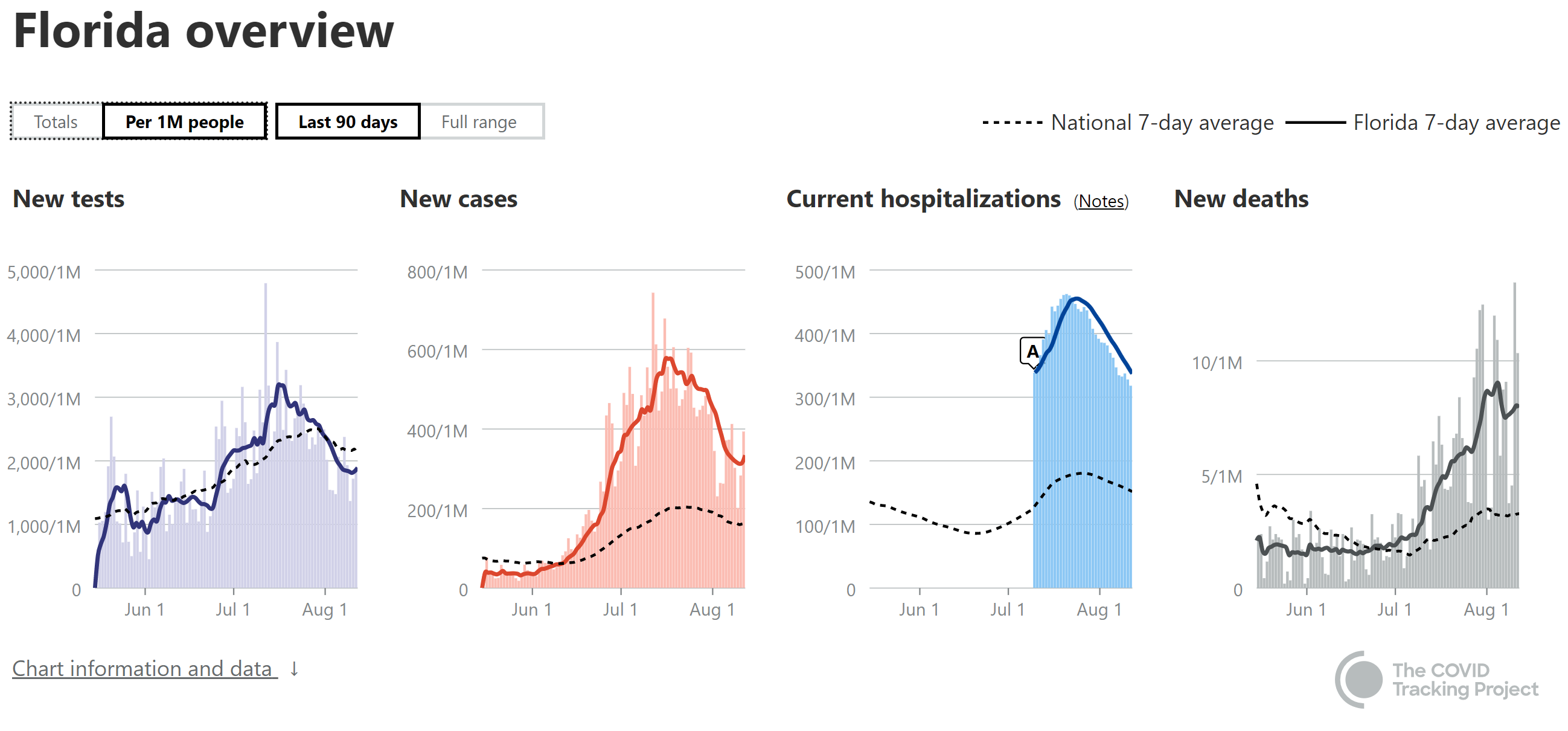
- Note: I'm using 7-day moving averages on a per capita (per 1MM) basis for these discussions of cases, hospitalizations and deaths, from the Covidtracking site.
- National Stats: cases peaked and plateaued for about 3 weeks at roughly ~2X the first wave, but are clearly now on the decline, while hospitalizations have also started to decline, after peaking at slightly more than the peak in the first wave, but this turns out to be only a little more than half of what they were in the first wave (relative to cases, which were 2X, as much per capita). Deaths are up over 2X from their early July low and look like they might be starting to peak at about half of the April peak (1100-1150/day now vs. 2250/day in April). So, relatively speaking, a bit of better news, although our current peak death rates are still worse than all but a handful of countries with over 50MM in population (Brazil, Mexico, Colombia and South Africa), per capita.
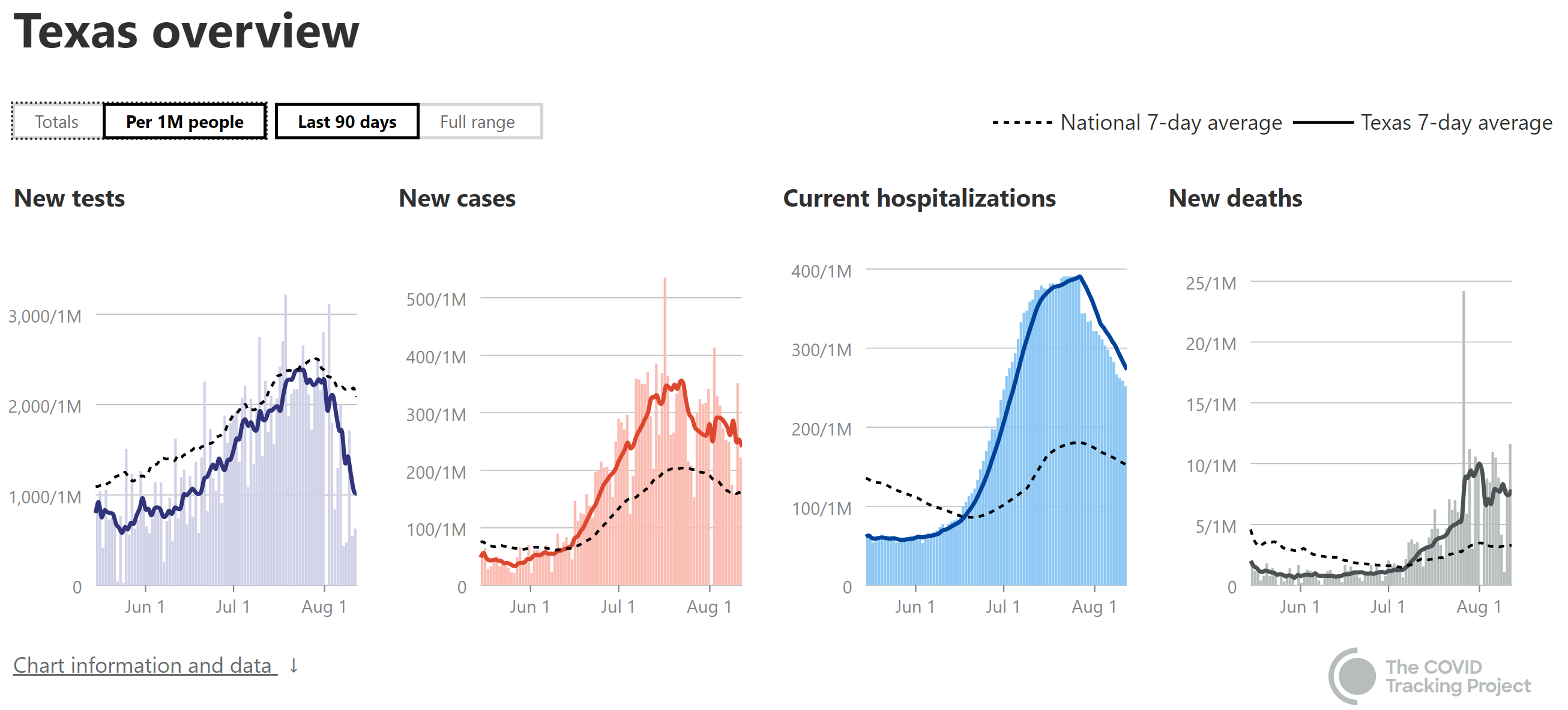
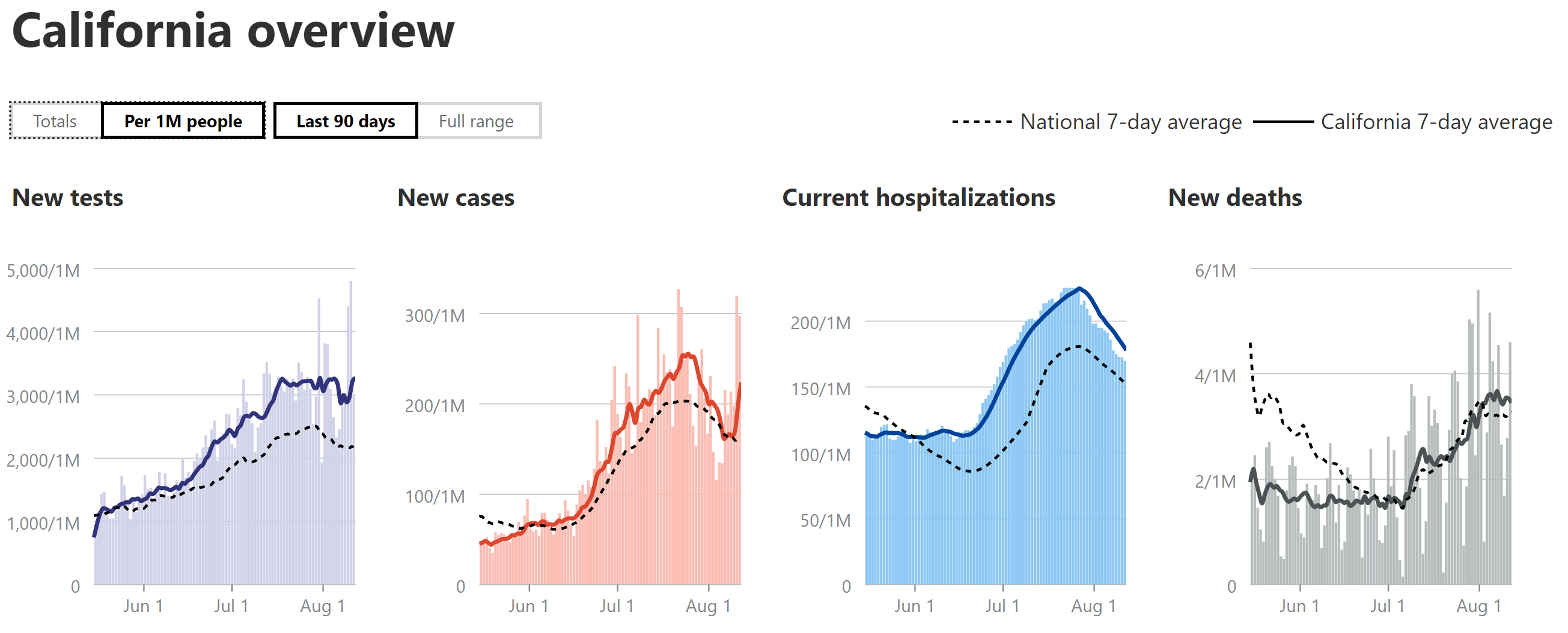
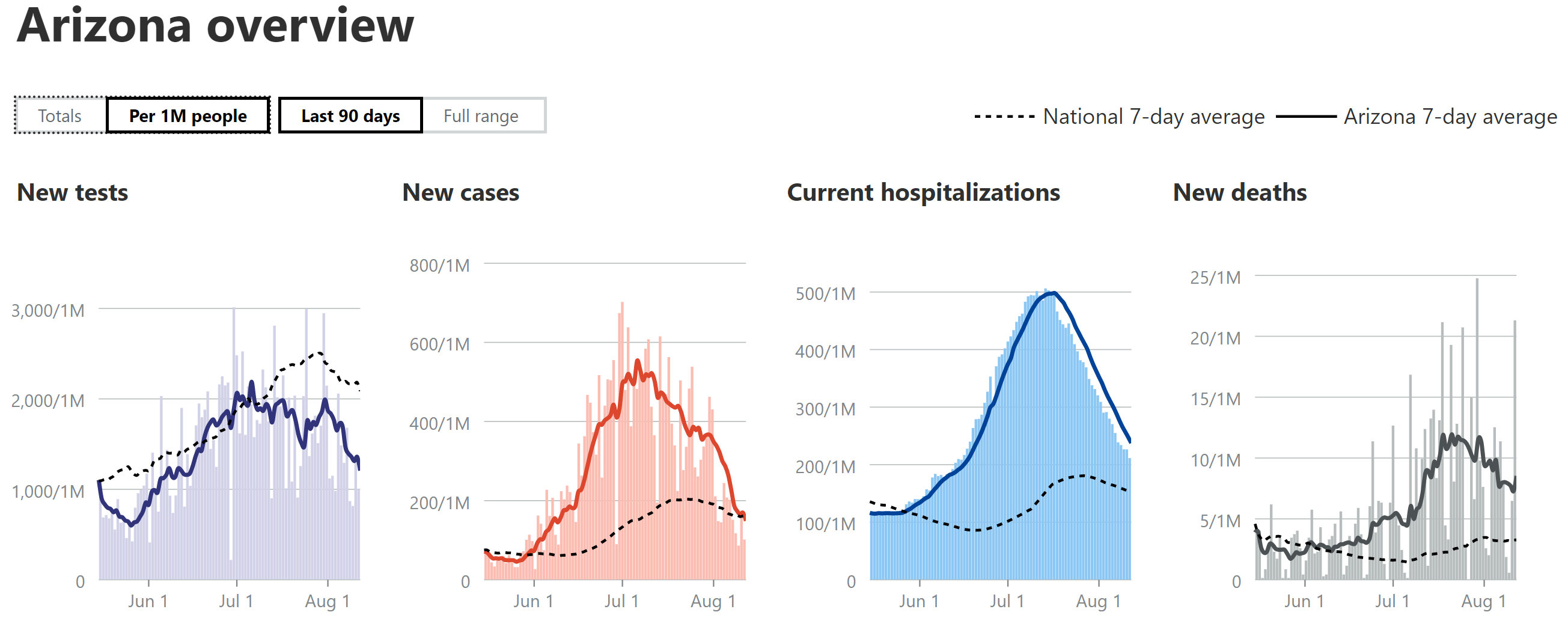
- Cases in AZ/FL/TX/CA: For the 4 states I've been looking at, closely (Florida, Texas, California, as all three spiked and are the 3 largest states, plus Arizona, as it peaked earlier and has a similar population as NJ, the comparator) cases are continuing to decline in AZ and in FL/TX/CA, cases appeared to be just starting to decline last week, but are definitely declining now. The AZ peak was about 30% more, per capita (per 1MM people) than the NJ peak (about 3500/day or 400/1MM), while the FL peak was ~50% more, the TX peak was ~10% less and the CA peak was ~40% less.
- Hospitalizations in AZ/FL/TX/CA: AZ's hospitalizations peaked (and are declining) at ~55% of NJ's (which were 8000 total or 900 per 1MM), while FL peaked at about 50% of NJ's per capita rate (and is declining) and TX peaked at ~45% of NJ's rate and is now declining. CA peaked last week at 25% of NJ's peak and have started to decline. As per previous reports, these reductions vs. NJ are likely due to the much younger age of those infected in this wave, combined with far more aggressive testing than during our peak (we had positivity rates of 40-50% due to lack of tests), which is discovering more mild/asymptomatic cases.
- Deaths in AZ/FL/TX/CA: My guesstimate has been that deaths in AZ/FL/TX would likely be about 1/3-2/3 of the peaks of NJ (about 270-300/day or ~31/1MM), partly due to the younger age and milder cases of those infected (as above) and partly due to improved treatments and procedures. AZ peaked at ~40% of NJ's peak and despite having major fluctuations, they're death rates finally appear to have levelled off and may be starting to decline. FL is now at about 30% of NJ's peak and it's possible they're approaching their peak, while TX looks like it may have peaked at 30% of NJ's peak, but their death data have been all over the map, so let's wait another week before declaring they've peaked. CA's case/hospitalization rates have been well below the other 3 states and is why CA is only at 12% of NJ's peak and will likely max out at <15% of NJ's peak, as I've been predicting based on lower case rates per capita vs. the other 3 states. It's quite possible that deaths have been on the low side of my guesstimates given the recent data showing convalescent plasma likely has over a 50% mortality reduction and it's being used heavily in seriously ill patients.
Time for the weekly update in bulleted format. Getting more involved in some work these days, which is why my posting is down. Some will rejoice, others maybe not, lol.
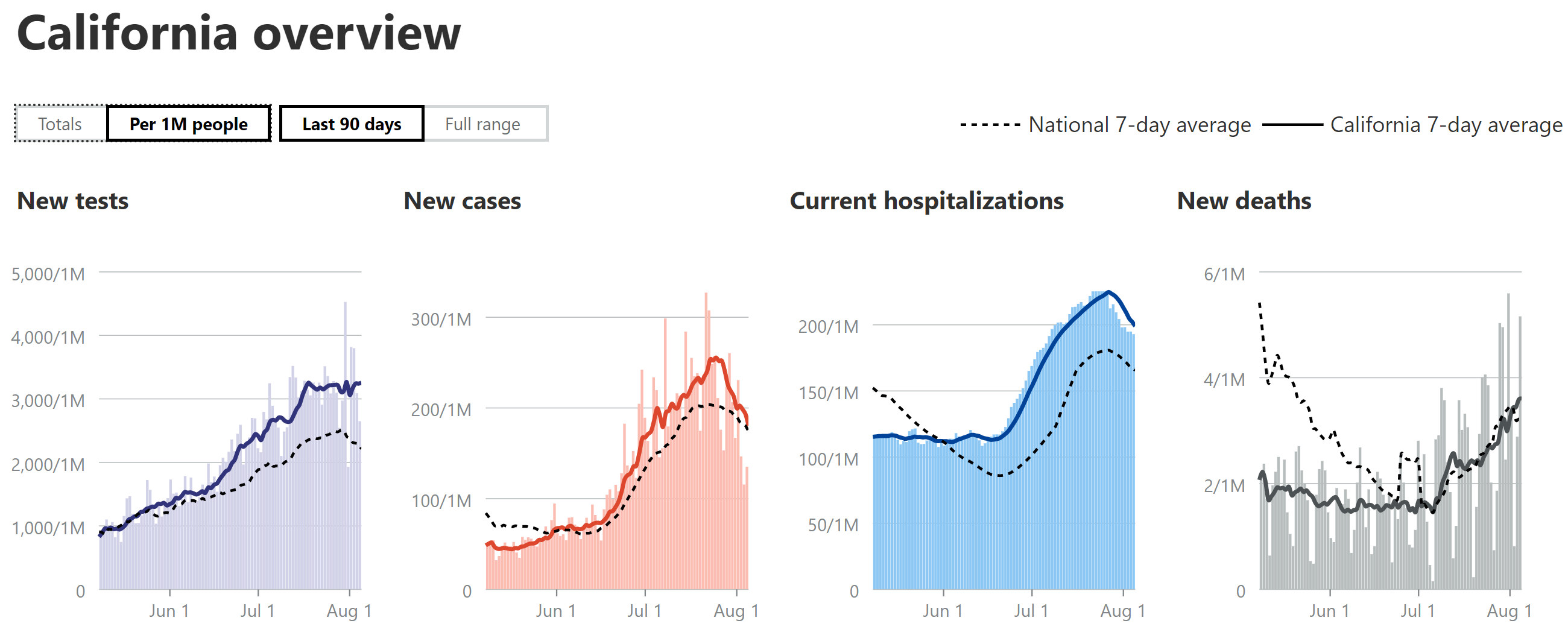
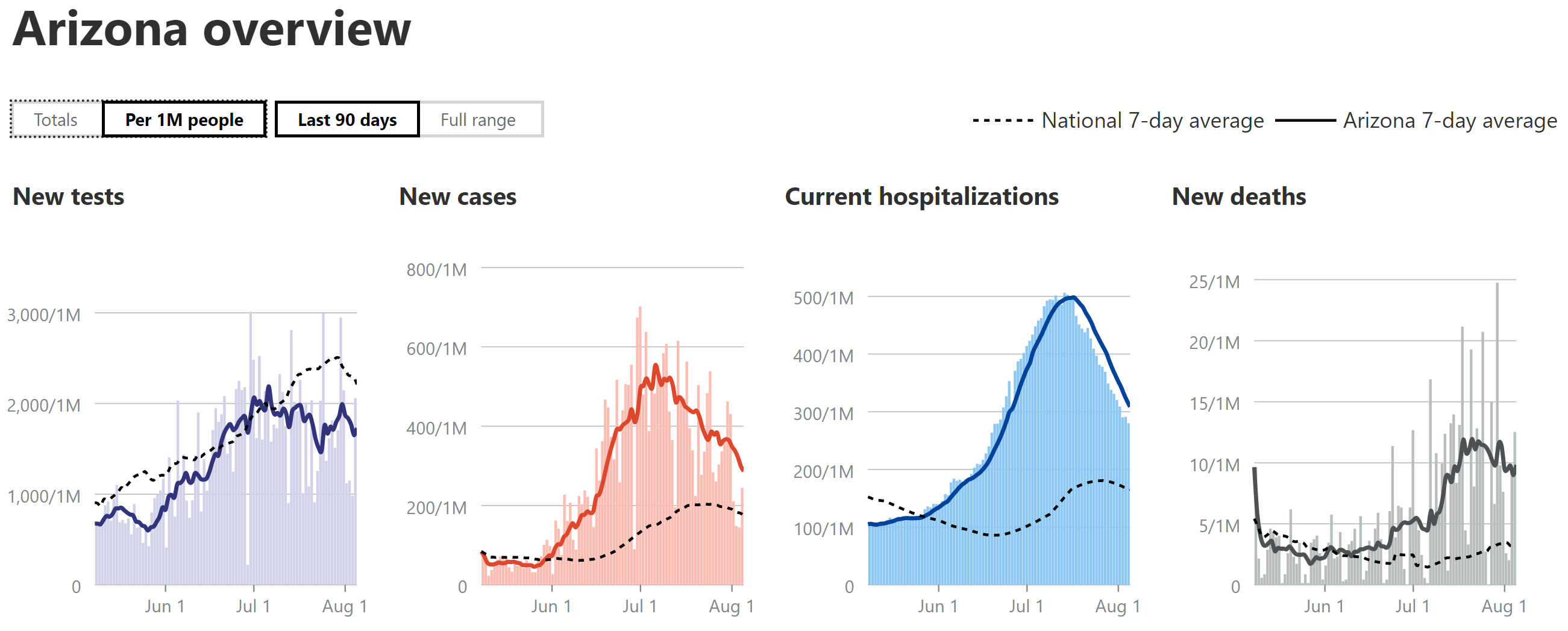
- Still using 7-day moving averages on a per capita (per 1MM) basis for most of the discussions of cases, hospitalizations and deaths (especially for comparing states), from the Covidtracking site.
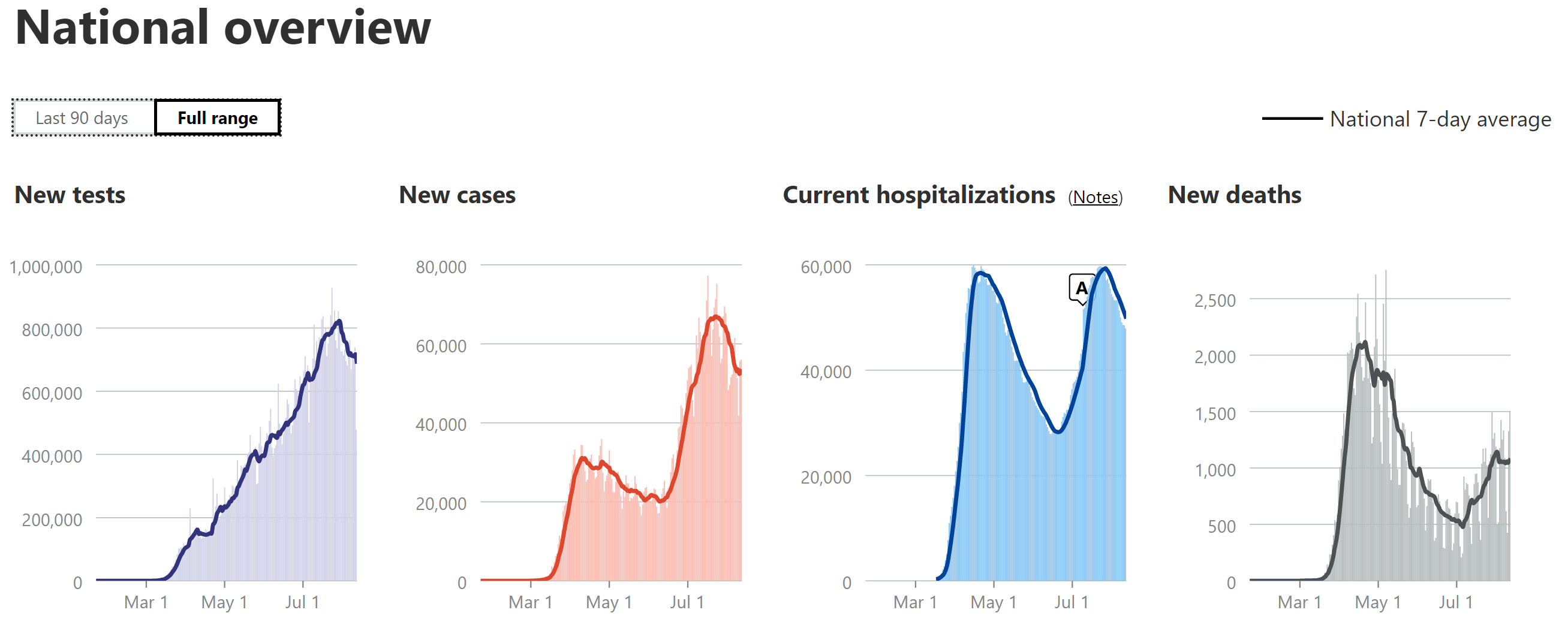
- National Stats: cases peaked around 65-68K/day for awhile (~2X the peak from wave 1), but declined the past week or two and have now plateaued again in the range of ~55K cases/day for about the past week. Hospitalizations peaked at about ~60K, which is very close to the peak in the first wave, but if the dynamics were the same as the first wave, this 2nd peak would have also been ~2X what they were in the first wave, not roughly the same, meaning the hospitalization rate is roughly half the rate it was for the first wave (relative to cases). Deaths are up over 2X from their early July low and they've now clearly peaked at a rate of about 1000-1150 per day (7-day MA) over the past 2 weeks, which is about half of the April peak (2100-2250/day in April). So, relatively speaking, a bit of better news, although our current peak death rates are still worse than all but a handful of countries with over 50MM in population (Brazil, Mexico, Colombia and South Africa), per capita. As I've been saying for weeks now, hospitalizations and deaths are likely half of what they were in wave 1 due to the combination of younger patient profile, more testing (per capita vs. NJ) leading to more mild cases, and improved medical procedures/pharmaceutical treatments.
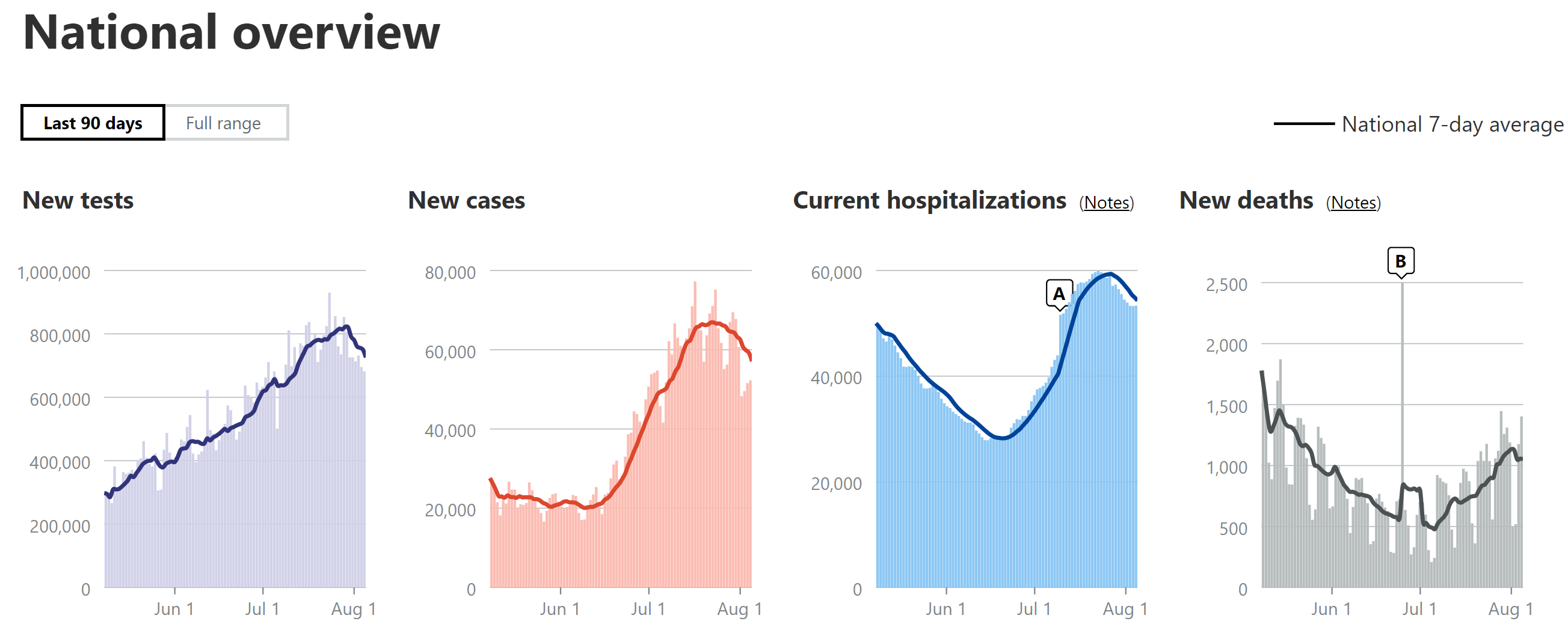
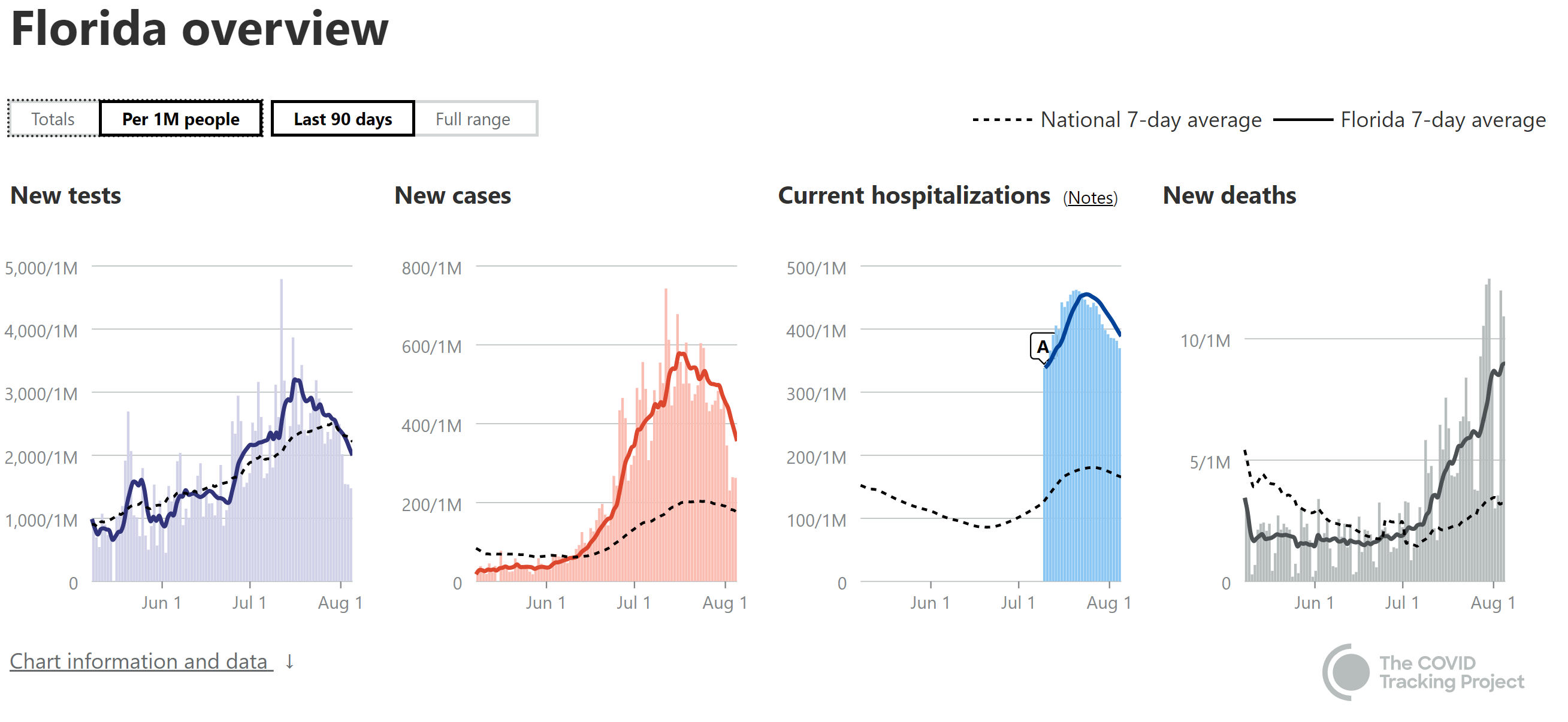
- Cases in AZ/FL/TX/CA: For the 4 states I've been looking at, closely (Florida, Texas, California, as all three spiked and are the 3 largest states, plus Arizona, as it peaked earlier and has a similar population as NJ, the comparator) cases are continuing to decline in AZ and it's now clear that cases are declining in FL/TX and they were in CA, but CA spiked back up to its old peak level the past few days. Another interesting observation is that FL/TX/AZ have all seen major drops (30-60% down from their recent peaks) in reported tests, which is a little disconcerting, as part of the case decrease is very likely due to the major drop in testing, especially given the rises in positive tests seen in all three states. No idea why they'd be reducing testing. As per last week's post, the AZ case peak was about 30% more, per capita (per 1MM people) than the NJ peak (about 3500/day or 400/1MM), while the FL peak was ~50% more, the TX peak was ~10% less and the CA peak was ~40% less.
- Hospitalizations in AZ/FL/TX/CA: AZ's hospitalizations peaked (and are declining) at ~55% of NJ's (which were 8000 total or 900 per 1MM), while FL peaked at about 50% of NJ's per capita rate (and is declining) and TX peaked at ~45% of NJ's rate and is now declining. CA peaked last week at 25% of NJ's peak and have started to decline. As per previous reports, these reductions vs. NJ are likely due to the much younger age of those infected in this wave, combined with far more aggressive testing than during our peak (we had positivity rates of 40-50% due to lack of tests), which is discovering more mild/asymptomatic cases.
- Deaths in AZ/FL/TX/CA: My guesstimate has been that deaths in AZ/FL/TX would likely be about 1/3-2/3 of the peaks of NJ (about 270-300/day or ~31/1MM), partly due to the younger age and milder cases of those infected (as above) and partly due to improved treatments and procedures. AZ peaked at ~40% of NJ's peak and despite having major fluctuations, they're death rates have been declining for about the past week or so, although they spiked up to their 2nd highest daily total today. FL was at about 30% of NJ's peak llast week and seemed like they were starting to decline, but they had their all-time highest death peak yesterday, so it's premature to day they're declining yet. TX looks like they may have peaked at about 1/3 of NJ's peak and might be starting to decline, but again, their fluctuations have been large, so calling it a decline yet is tough. CA's case/hospitalization rates have been well below the other 3 states and their death rate appears to be leveling off at about 12% of NJ's peak, as I've been predicting based on lower case rates per capita vs. the other 3 states. It's quite possible that deaths have been on the low side of my guesstimates given the recent data showing convalescent plasma likely has over a 50% mortality reduction and it's being used heavily in these states. Also, keep an eye on Georgia, whose deaths have been rising quickly; they're already at about 20-25% of NJ's peak.
- Getting back to the big picture, it's good to see that most states are now seeing flat or declining levels of cases, with only a few increasing (most were increasing several weeks ago); however, due to the 2-4 week lag from cases to deaths, deaths are still increasing or flat in many states.
https://www.worldometers.info/coronavirus/country/us
https://www.nytimes.com/interactive...rus®ion=TOP_BANNER&context=storylines_menu
My neighbors who think the entire covid thing is a hoax and who is a gym rat just outfitted his basement and my buddy who is a contractor and had 3 gym memberships said he will never go back to a gym,
Cool stories ancidotalTom
49 states! What is wrong with King Murphy!!! Flatten the curve Murph??
Give us 15 days!
It definitely slowed it and prevented it from overwhelming the healthcare system. And if you put yourself in complete lockdown and/or wore an N.99 mask, you'd keep the virus from infecting you.
Nothing like a hurricane. Horrific analogy.
Based on your frightened postings, You prob go to sleep and shower with a N95
everyone be sure to wear your masks at home during your zoom meetings!
https://www.foxnews.com/health/face-masks-coronavirus-zoom-calls
https://www.foxnews.com/health/face-masks-coronavirus-zoom-calls
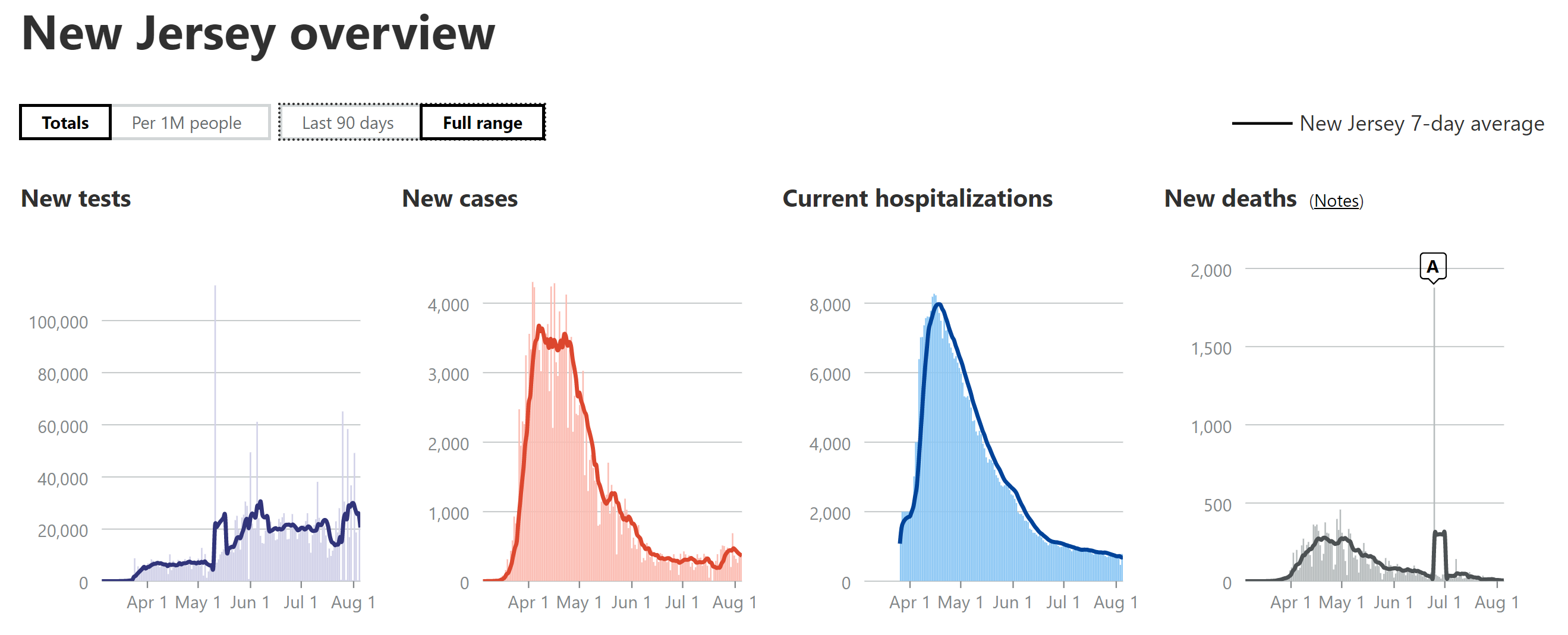
Based ok the NJ graphs we isn’t NJ in stage 3? Every data at low points.Time for the weekly update in bulleted format. Getting more involved in some work these days, which is why my posting is down. Some will rejoice, others maybe not, lol.
https://covidtracking.com/data#chart-annotations
- Still using 7-day moving averages on a per capita (per 1MM) basis for most of the discussions of cases, hospitalizations and deaths (especially for comparing states), from the Covidtracking site.
- National Stats: cases peaked around 65-68K/day for awhile (~2X the peak from wave 1), but declined the past week or two and have now plateaued again in the range of ~55K cases/day for about the past week. Hospitalizations peaked at about ~60K, which is very close to the peak in the first wave, but if the dynamics were the same as the first wave, this 2nd peak would have also been ~2X what they were in the first wave, not roughly the same, meaning the hospitalization rate is roughly half the rate it was for the first wave (relative to cases). Deaths are up over 2X from their early July low and they've now clearly peaked at a rate of about 1000-1150 per day (7-day MA) over the past 2 weeks, which is about half of the April peak (2100-2250/day in April). So, relatively speaking, a bit of better news, although our current peak death rates are still worse than all but a handful of countries with over 50MM in population (Brazil, Mexico, Colombia and South Africa), per capita. As I've been saying for weeks now, hospitalizations and deaths are likely half of what they were in wave 1 due to the combination of younger patient profile, more testing (per capita vs. NJ) leading to more mild cases, and improved medical procedures/pharmaceutical treatments.
- Cases in AZ/FL/TX/CA: For the 4 states I've been looking at, closely (Florida, Texas, California, as all three spiked and are the 3 largest states, plus Arizona, as it peaked earlier and has a similar population as NJ, the comparator) cases are continuing to decline in AZ and it's now clear that cases are declining in FL/TX and they were in CA, but CA spiked back up to its old peak level the past few days. Another interesting observation is that FL/TX/AZ have all seen major drops (30-60% down from their recent peaks) in reported tests, which is a little disconcerting, as part of the case decrease is very likely due to the major drop in testing, especially given the rises in positive tests seen in all three states. No idea why they'd be reducing testing. As per last week's post, the AZ case peak was about 30% more, per capita (per 1MM people) than the NJ peak (about 3500/day or 400/1MM), while the FL peak was ~50% more, the TX peak was ~10% less and the CA peak was ~40% less.
- Hospitalizations in AZ/FL/TX/CA: AZ's hospitalizations peaked (and are declining) at ~55% of NJ's (which were 8000 total or 900 per 1MM), while FL peaked at about 50% of NJ's per capita rate (and is declining) and TX peaked at ~45% of NJ's rate and is now declining. CA peaked last week at 25% of NJ's peak and have started to decline. As per previous reports, these reductions vs. NJ are likely due to the much younger age of those infected in this wave, combined with far more aggressive testing than during our peak (we had positivity rates of 40-50% due to lack of tests), which is discovering more mild/asymptomatic cases.
- Deaths in AZ/FL/TX/CA: My guesstimate has been that deaths in AZ/FL/TX would likely be about 1/3-2/3 of the peaks of NJ (about 270-300/day or ~31/1MM), partly due to the younger age and milder cases of those infected (as above) and partly due to improved treatments and procedures. AZ peaked at ~40% of NJ's peak and despite having major fluctuations, they're death rates have been declining for about the past week or so, although they spiked up to their 2nd highest daily total today. FL was at about 30% of NJ's peak llast week and seemed like they were starting to decline, but they had their all-time highest death peak yesterday, so it's premature to day they're declining yet. TX looks like they may have peaked at about 1/3 of NJ's peak and might be starting to decline, but again, their fluctuations have been large, so calling it a decline yet is tough. CA's case/hospitalization rates have been well below the other 3 states and their death rate appears to be leveling off at about 12% of NJ's peak, as I've been predicting based on lower case rates per capita vs. the other 3 states. It's quite possible that deaths have been on the low side of my guesstimates given the recent data showing convalescent plasma likely has over a 50% mortality reduction and it's being used heavily in these states. Also, keep an eye on Georgia, whose deaths have been rising quickly; they're already at about 20-25% of NJ's peak.
- Getting back to the big picture, it's good to see that most states are now seeing flat or declining levels of cases, with only a few increasing (most were increasing several weeks ago); however, due to the 2-4 week lag from cases to deaths, deaths are still increasing or flat in many states.
https://www.worldometers.info/coronavirus/country/us
https://www.nytimes.com/interactive...rus®ion=TOP_BANNER&context=storylines_menu
everyone be sure to wear your masks at home during your zoom meetings!
https://www.foxnews.com/health/face-masks-coronavirus-zoom-calls
Just one example of the mass hysteria
No, you say that because you're a dope who falls for easy-to-remember slogans.
He fits the profile of his leader. “We love the uneducated”
New Jersey Health Commissioner on Fox5 local news (probably the best interview I've seen in this whole pandemic as it pertains to NJ). The anchors asked the commissioner directly about restaurants ( indoor dining) and gyms, she said they won't be opened until we learn more about how the virus is transmitted indoors via ventilation and air conditioning and currently, from a health commission perspective there is to much risk.
Start a little before the 4 min mark, watch till the end.
https://www.fox5ny.com/video/840068
Start a little before the 4 min mark, watch till the end.
https://www.fox5ny.com/video/840068
That is what concerns me about opening schools. It seems contradictory.
, she said they won't be opened until we learn more about how the virus is transmitted indoors via ventilation and air conditioning and currently,
, she said they won't be opened until we learn more about how the virus is transmitted indoors via ventilation and air conditioning and currently,
New Jersey Health Commissioner on Fox5 local news (probably the best interview I've seen in this whole pandemic as it pertains to NJ). The anchors asked the commissioner directly about restaurants ( indoor dining) and gyms, she said they won't be opened until we learn more about how the virus is transmitted indoors via ventilation and air conditioning and currently, from a health commission perspective there is to much risk.
Start a little before the 4 min mark, watch till the end.
https://www.fox5ny.com/video/840068
I guess Pennslyvania has access to data that the Governor and his minion do not want to see
they did a great job trying to pinpoint her down on the interview...and she scrambled especially about gyms and dining
yet casinos are open
Last edited:
How did the other 49 states reach their conclusion to open in- door dining? This is becoming a joke.I guess Pennslyvania has access to data that the Governor and his minion do not want to see
Because it’s BS.That is what concerns me about opening schools. It seems contradictory.
, she said they won't be opened until we learn more about how the virus is transmitted indoors via ventilation and air conditioning and currently,
RU - shouldn’t NJ be in Stage 3 based on your graphs? Data determines dates.Time for the weekly update in bulleted format. Getting more involved in some work these days, which is why my posting is down. Some will rejoice, others maybe not, lol.
https://covidtracking.com/data#chart-annotations
- Still using 7-day moving averages on a per capita (per 1MM) basis for most of the discussions of cases, hospitalizations and deaths (especially for comparing states), from the Covidtracking site.
- National Stats: cases peaked around 65-68K/day for awhile (~2X the peak from wave 1), but declined the past week or two and have now plateaued again in the range of ~55K cases/day for about the past week. Hospitalizations peaked at about ~60K, which is very close to the peak in the first wave, but if the dynamics were the same as the first wave, this 2nd peak would have also been ~2X what they were in the first wave, not roughly the same, meaning the hospitalization rate is roughly half the rate it was for the first wave (relative to cases). Deaths are up over 2X from their early July low and they've now clearly peaked at a rate of about 1000-1150 per day (7-day MA) over the past 2 weeks, which is about half of the April peak (2100-2250/day in April). So, relatively speaking, a bit of better news, although our current peak death rates are still worse than all but a handful of countries with over 50MM in population (Brazil, Mexico, Colombia and South Africa), per capita. As I've been saying for weeks now, hospitalizations and deaths are likely half of what they were in wave 1 due to the combination of younger patient profile, more testing (per capita vs. NJ) leading to more mild cases, and improved medical procedures/pharmaceutical treatments.
- Cases in AZ/FL/TX/CA: For the 4 states I've been looking at, closely (Florida, Texas, California, as all three spiked and are the 3 largest states, plus Arizona, as it peaked earlier and has a similar population as NJ, the comparator) cases are continuing to decline in AZ and it's now clear that cases are declining in FL/TX and they were in CA, but CA spiked back up to its old peak level the past few days. Another interesting observation is that FL/TX/AZ have all seen major drops (30-60% down from their recent peaks) in reported tests, which is a little disconcerting, as part of the case decrease is very likely due to the major drop in testing, especially given the rises in positive tests seen in all three states. No idea why they'd be reducing testing. As per last week's post, the AZ case peak was about 30% more, per capita (per 1MM people) than the NJ peak (about 3500/day or 400/1MM), while the FL peak was ~50% more, the TX peak was ~10% less and the CA peak was ~40% less.
- Hospitalizations in AZ/FL/TX/CA: AZ's hospitalizations peaked (and are declining) at ~55% of NJ's (which were 8000 total or 900 per 1MM), while FL peaked at about 50% of NJ's per capita rate (and is declining) and TX peaked at ~45% of NJ's rate and is now declining. CA peaked last week at 25% of NJ's peak and have started to decline. As per previous reports, these reductions vs. NJ are likely due to the much younger age of those infected in this wave, combined with far more aggressive testing than during our peak (we had positivity rates of 40-50% due to lack of tests), which is discovering more mild/asymptomatic cases.
- Deaths in AZ/FL/TX/CA: My guesstimate has been that deaths in AZ/FL/TX would likely be about 1/3-2/3 of the peaks of NJ (about 270-300/day or ~31/1MM), partly due to the younger age and milder cases of those infected (as above) and partly due to improved treatments and procedures. AZ peaked at ~40% of NJ's peak and despite having major fluctuations, they're death rates have been declining for about the past week or so, although they spiked up to their 2nd highest daily total today. FL was at about 30% of NJ's peak llast week and seemed like they were starting to decline, but they had their all-time highest death peak yesterday, so it's premature to day they're declining yet. TX looks like they may have peaked at about 1/3 of NJ's peak and might be starting to decline, but again, their fluctuations have been large, so calling it a decline yet is tough. CA's case/hospitalization rates have been well below the other 3 states and their death rate appears to be leveling off at about 12% of NJ's peak, as I've been predicting based on lower case rates per capita vs. the other 3 states. It's quite possible that deaths have been on the low side of my guesstimates given the recent data showing convalescent plasma likely has over a 50% mortality reduction and it's being used heavily in these states. Also, keep an eye on Georgia, whose deaths have been rising quickly; they're already at about 20-25% of NJ's peak.
- Getting back to the big picture, it's good to see that most states are now seeing flat or declining levels of cases, with only a few increasing (most were increasing several weeks ago); however, due to the 2-4 week lag from cases to deaths, deaths are still increasing or flat in many states.
https://www.worldometers.info/coronavirus/country/us
https://www.nytimes.com/interactive...rus®ion=TOP_BANNER&context=storylines_menu
This is where I agree with bac and King of S. If you can open schools I dont see how you cant open these other places.
I realize that schools may be more essential but they carry a much greater risk of spread also
I realize that schools may be more essential but they carry a much greater risk of spread also
everyone be sure to wear your masks at home during your zoom meetings!
https://www.foxnews.com/health/face-masks-coronavirus-zoom-calls
If you have Norton Anti Virus on your computer aren't you protected enough that you don't have to wear a mask during zoom meeting?
This is where I agree with bac and King of S. If you can open schools I dont see how you cant open these other places.
I realize that schools may be more essential but they carry a much greater risk of spread also
NY Times story on the opening of gyms in NJ but this quote is telling from the Gov.
Mr. Murphy, who backtracked on his plan to permit indoor dining as cases began to surge in other states that reopened early, has said it is simply too soon to open gyms in a state where 15,878 deaths have been linked to the virus.
“It’s something we want to get to,” Mr. Murphy said on Monday. “We also want to get to it and not kill anybody.”
From this quote we have gone from flattening the curve to "not kill anybody". We can debate the morality of it. But the goal posts have definitely changed.
Also from the article 43 states have opened Gyms in some form. The article listed on two cases (in New Mexico) of Gyms causing spread.
https://www.nytimes.com/2020/08/13/...tion=click&module=Top Stories&pgtype=Homepage
I like to constantly challenge my own opinions and conventional wisdom. This is an interesting video that gives a sane presentation that challenges existing theories. I would love to get folks take on this.
NY Times story on the opening of gyms in NJ but this quote is telling from the Gov.
Mr. Murphy, who backtracked on his plan to permit indoor dining as cases began to surge in other states that reopened early, has said it is simply too soon to open gyms in a state where 15,878 deaths have been linked to the virus.
“It’s something we want to get to,” Mr. Murphy said on Monday. “We also want to get to it and not kill anybody.”
From this quote we have gone from flattening the curve to "not kill anybody". We can debate the morality of it. But the goal posts have definitely changed.
Also from the article 43 states have opened Gyms in some form. The article listed on two cases (in New Mexico) of Gyms causing spread.
https://www.nytimes.com/2020/08/13/nyregion/nj-gyms-reopening.html?action=click&module=Top Stories&pgtype=Homepage
remember he said weeks not months back in June..he is a liar...all he is doing is pushing everything further back all the while everything improves. he will wait until after election day to even think about opening gyms.
the changing goalposts are why I urge Americans to ask questions and voice opinions. Who made politicians God. The public had and has had zero imput on decision making the past 5 months
how many people die of regular flu that have spread flus in gyms over the years, how many 70 year olds are working out a gyms where they will die. We have about 13K deaths in the country for people under the age of 55...and how many of those in the last month...really makes you think doesnt it.
how can casinos be allowed to be opened....$$$$$$$$$$
The governor should be placing all his importance on nursing homes...thats where he killed people, not by letting people go to gyms
if it saves only one life..lmfao
Last edited:
NY Times story on the opening of gyms in NJ but this quote is telling from the Gov.
Mr. Murphy, who backtracked on his plan to permit indoor dining as cases began to surge in other states that reopened early, has said it is simply too soon to open gyms in a state where 15,878 deaths have been linked to the virus.
“It’s something we want to get to,” Mr. Murphy said on Monday. “We also want to get to it and not kill anybody.”
From this quote we have gone from flattening the curve to "not kill anybody". We can debate the morality of it. But the goal posts have definitely changed.
Also from the article 43 states have opened Gyms in some form. The article listed on two cases (in New Mexico) of Gyms causing spread.
https://www.nytimes.com/2020/08/13/nyregion/nj-gyms-reopening.html?action=click&module=Top Stories&pgtype=Homepage
What's crazy is not just the shift from curve flattening to where we are now, but that the governor thinks saving people from death by gym visit is his responsibility.
I like to constantly challenge my own opinions and conventional wisdom. This is an interesting video that gives a sane presentation that challenges existing theories. I would love to get folks take on this.
Without watching, Tom Woods is an ace.
I like to constantly challenge my own opinions and conventional wisdom. This is an interesting video that gives a sane presentation that challenges existing theories. I would love to get folks take on this.
thank you for posting this...very very good listen and raises alot of points and questions...also calls out some of the same stuff we see in this thread when you challenge the preferred narrative. And as a Trump supporter, he has been pretty bad on messaging and I dont look for him for truth but i also dont look to cnn and ny times either. They all are corrupt. Seek out your own truth by trying to find different sources and decide for yourself. Ask questions.
Good Morning: Just to be factual here , in the beginning the state of Hawaii was a proponent of , wear a mask, wash hands and socially distance. Over the weeks that followed people started to go back to what Hawaiians do normally... Party on weekends , bar hop and in general do exactly what many other states did... also keep in mind the number of visitors , though low in number, returned from mainland visits and also the return of military personnel ... People blame this on opening too soon .....people did not adhere to guidelines when on beaches, bars and in larger groups... The governor of Hawaii, Ige and Josh Green his 2nd in command ( also medical lead) plus mayor Caldwell have not done a bad job ... people even in a very liberal state like Hawaii want their freedoms of choice... tough not to see ...The culture of Hawaii rests with Ohana and their love of doing things as a family... much of the current spread is within family groupings...no different than here on the mainland... The one thing that remains true is the military in and out has not been a big impact... Now for today be safe.it means the virus is going to spread despite people trying to go through all the precautions....Hawaii has been one of the strictest mask states around. But oh wait we keep hearing its red states causing us not to play football
its means that the mask thing cannot be used as explanations everytime there is a spread, ask questions, coronavirus does what it wants and we are still playing catchup and trying to figure it out
Good Morning: Just to be factual here , in the beginning the state of Hawaii was a proponent of , wear a mask, wash hands and socially distance. Over the weeks that followed people started to go back to what Hawaiians do normally... Party on weekends , bar hop and in general do exactly what many other states did... also keep in mind the number of visitors , though low in number, returned from mainland visits and also the return of military personnel ... People blame this on opening too soon .....people did not adhere to guidelines when on beaches, bars and in larger groups... The governor of Hawaii, Ige and Josh Green his 2nd in command ( also medical lead) plus mayor Caldwell have not done a bad job ... people even in a very liberal state like Hawaii want their freedoms of choice... tough not to see ...The culture of Hawaii rests with Ohana and their love of doing things as a family... much of the current spread is within family groupings...no different than here on the mainland... The one thing that remains true is the military in and out has not been a big impact... Now for today be safe.
dont they have one of the most liberal senators out there..yet I was told repeatedly here what type of people were spreading....oh nevermind
Another good widespread antibody testing study done, this time out of England. Pretty much in line with the other studies, but the thing the jumps out is a third of the people are asymptomatic. We need to understand why.
https://www.bloomberg.com/news/arti...udy-finds-3-4-million-in-england-had-covid-19
https://www.bloomberg.com/news/arti...udy-finds-3-4-million-in-england-had-covid-19
I agree with asking questions of both sides.thank you for posting this...very very good listen and raises alot of points and questions...also calls out some of the same stuff we see in this thread when you challenge the preferred narrative. And as a Trump supporter, he has been pretty bad on messaging and I dont look for him for truth but i also dont look to cnn and ny times either. They all are corrupt. Seek out your own truth by trying to find different sources and decide for yourself. Ask questions.
I also think most of the points Woods made have been raised in this thread and debated thoroughly, and I vehemently disagree with him for the most part. I also felt some of his points that haven’t been discussed were severely exaggerated bordering on downright lies (regarding Japan and the Olympics).
Albany, what were the specific points he raised that you hadn’t considered? Just curious, because otherwise I’m not sure how to go about starting this discussion (i.e. I don’t know where to begin with my disagreements).
Looks like the order of magnitude estimate still appears roughly accurate (10x as many actual cases as confirmed cases)Another good widespread antibody testing study done, this time out of England. Pretty much in line with the other studies, but the thing the jumps out is a third of the people are asymptomatic. We need to understand why.
https://www.bloomberg.com/news/arti...udy-finds-3-4-million-in-england-had-covid-19
I agree with asking questions of both sides.
I also think most of the points Woods made have been raised in this thread and debated thoroughly, and I vehemently disagree with him for the most part. I also felt some of his points that haven’t been discussed were severely exaggerated bordering on downright lies (regarding Japan and the Olympics).
Albany, what were the specific points he raised that you hadn’t considered? Just curious, because otherwise I’m not sure how to go about starting this discussion (i.e. I don’t know where to begin with my disagreements).
one thing that doesnt get addressed is ADMITTING THAT WE DO NOT KNOW....instead we get narratives about the certainty that masks are stopping the outbreak in Connecticut but somehow in California its different...do you not question that>
Do you question why in April the msm was writing how South Dakota was going to have an incredible spike and they didnt...do you question why in July the msm wrote how South Dakota was going to have an incredible spike and they didnt....do you question why in August the msm is going nuts over a motorcycle rally in Sturges. How dare the Governor of South Dakota not require masks and shutdown her state in March like everyone else.....seems like she did pretty good didnt she.
How about Japan, the OP and msm were extremely concerned that their way of doing things would lead to disaster and that was WITH MASKS..what happened?
Is it true Sweden has just 70 deaths under the age of 50...if this is actually true this is very telling.
the average age of Covid death is 81 and the average life expectancy number is 78
The endless everyday death totals as if we track other death totals or even flu death totals is bizarre. The arbitrary use of science in this thread as a way of explaining things away and then in other cases not using science but saying well people are not dying now because......
end games...no one ever wants to talk about end games here and you dont hear the msm asking those questions..you just see moving of the goalposts..look no further than Murphy
Everytime that Woods points have been brought up in this thread its been met with incredible pushback of how dare you say this
one thing that doesnt get addressed is ADMITTING THAT WE DO NOT KNOW....instead we get narratives about the certainty that masks are stopping the outbreak in Connecticut but somehow in California its different...do you not question that>
California and Connecticut have roughly the same case numbers per capita. And I thought Newsom opened up CA too quickly
Mazie Hirono (senator) ...the people of Hawaii, though very liberal , also flaunted the wearing of masks and social distancing after governor began to open things up. Some blamed him others blamed the younger 21-40 age group. If you saw the beaches , bars , restaurants and parks the people were on a slippery slope . Now we see the uptick in covid occurring exponentially.The culture of Hawaii is all about tourism and getting visitors into the economy. It was a double edged sword for them. These swings are not due to the crepitus crew...it is caused by the kids and grandkids .We have spent many weeks on all the islands ...2020 will not be another.dont they have one of the most liberal senators out there..yet I was told repeatedly here what type of people were spreading....oh nevermind
Does this sound like it has merit?
Scientists develop nasal spray to fight coronavirus
Researchers at the University of California, San Francisco, say they have created a nasal spray that can help ward off the coronavirus – not as a cure or vaccine, but as an antiviral.
“Far more effective than wearable forms of personal protective equipment, we think of AeroNabs as a molecular form of PPE that could serve as an important stopgap until vaccines provide a more permanent solution to COVID-19,” said AeroNabs co-inventor Peter Walter, professor of biochemistry and biophysics at UCSF, in a news release.
Nanobodies in the spray are smaller than human antibodies, making them easier to manipulate in a laboratory setting, said co-inventor Aashish Manglik, MD, PhD, an assistant professor of pharmaceutical chemistry. Nanobodies, for this reason, are therefore less expensive and easier to mass produce. The researchers are currently working to get the spray manufactured and clinically tested.
Yes, these nanobodies are the most potent COVID antivirals seen to date, so there's clearly potential there, although we're still months away from putting them into humans. The news release is excellent, but as often happens, Derek Lowe has done a very nice blog entry on nanobodies today, where he provides a fair amount more background on what these are and how they work. Fascinating stuff and the part I excerpted below is how their nanobody technology relates to SARS-CoV-2. Certainly one of the more promising treatment/prevention options we've seen and a great example of how research in one area can be taken and applied to a totally new and different problem, like COVID.
https://blogs.sciencemag.org/pipeli...obodies-against-the-coronavirus-something-new
These various forms were taken into a pseudovirus cell infection assay (that’s where you rig up a harmless virus to use the coronavirus’ infection machinery, Spike and all). Plain Nb6 had an IC50 of 2 micromolar, and another Class I nanobody (Nb11) was almost the same. The best Class II nanobody (Nb3) was 3.9 micromolar. But that trimeric form of Nb6 (Nb6-tri) was 1.2 nanomolar in the assay, a two-thousand-fold-improvement. Trimer forms of Nb11 and Nb3 also improved, but not as much. In a test of Vero cell infection with real SARS-Cov-2 coronavirus (done at the Pasteur Institute in France), Nb6-tri prevented viral attack with an IC50 of 160 picomolar, which is truly impressive.
They didn’t stop there, though. A “saturation mutagenesis” experiment around the sequence of Nb6 was then tried, with new rounds of assays, and this yielded a mutant nanobody that was still more potent. You might wonder about trying to make things even better when you started out with billions of nanobody candidates in the first round, but a quick look at the math shows that a couple of billion nanobodies are just a speck compared to the total number of possibilities (around 110 amino acids, 20 variations per!) This one was trimerized as before, and the new mNb6-tri, when put into the SPR assay, showed no off-rate at all during the limits of the experiment, putting its binding constant somewhere in the femtomolar range at worst. It comes in with IC50s of 120 picomolar in the pseudovirus assay and about 50 picomolar in the wild-type infection assay, but those are probably at the limit of detection for both. Basically, we don’t actually know how potent this nanobody construct is, because we don’t have assays good enough to read out a number (!)
Potential Therapeutic?
OK, now things get interesting. The authors tested the stability of mNb6-tri, and found that it can be heated, lyophilized (freeze-dried, basically), and nebulized into an aerosol with no loss of potency. It’s a very stable species that can put up with all sorts of handling and processing. You could certainly inject this material, just as you’d administer monocolonal antibodies. But there are more possibilities. How about formulating it as a nasal spray? Or in a nebulizer, to be breathed into the lungs, or even sprayed out into the room air? How about impregnating filter material with this protein so it pulls coronavirus particles out of the air as they pass through it? The extreme stability of nanobody proteins gives all of these a real shot, and they’re under serious consideration for development. The team says that they’re in discussion with several commercial partners to take this technology into human trials (and presumably medical-device trials, for the filtration idea), and I think that’s an excellent idea. This has real public-health potential, from the looks of it, and could be just the backup that we may need for the existing vaccine programs if they come in less effective than we’d like (or are rolled out more slowly than we’d like!) I hope that the money and resources are rounded up quickly.
I like to constantly challenge my own opinions and conventional wisdom. This is an interesting video that gives a sane presentation that challenges existing theories. I would love to get folks take on this.
THIS GUY GETS IT!!!!!
Based on your frightened postings, You prob go to sleep and shower with a N95
You said that yesterday. Guess you blacked out and forgot.
Yes, these nanobodies are the most potent COVID antivirals seen to date, so there's clearly potential there, although we're still months away from putting them into humans. The news release is excellent, but as often happens, Derek Lowe has done a very nice blog entry on nanobodies today, where he provides a fair amount more background on what these are and how they work. Fascinating stuff and the part I excerpted below is how their nanobody technology relates to SARS-CoV-2. Certainly one of the more promising treatment/prevention options we've seen and a great example of how research in one area can be taken and applied to a totally new and different problem, like COVID.
https://blogs.sciencemag.org/pipeli...obodies-against-the-coronavirus-something-new
These various forms were taken into a pseudovirus cell infection assay (that’s where you rig up a harmless virus to use the coronavirus’ infection machinery, Spike and all). Plain Nb6 had an IC50 of 2 micromolar, and another Class I nanobody (Nb11) was almost the same. The best Class II nanobody (Nb3) was 3.9 micromolar. But that trimeric form of Nb6 (Nb6-tri) was 1.2 nanomolar in the assay, a two-thousand-fold-improvement. Trimer forms of Nb11 and Nb3 also improved, but not as much. In a test of Vero cell infection with real SARS-Cov-2 coronavirus (done at the Pasteur Institute in France), Nb6-tri prevented viral attack with an IC50 of 160 picomolar, which is truly impressive.
They didn’t stop there, though. A “saturation mutagenesis” experiment around the sequence of Nb6 was then tried, with new rounds of assays, and this yielded a mutant nanobody that was still more potent. You might wonder about trying to make things even better when you started out with billions of nanobody candidates in the first round, but a quick look at the math shows that a couple of billion nanobodies are just a speck compared to the total number of possibilities (around 110 amino acids, 20 variations per!) This one was trimerized as before, and the new mNb6-tri, when put into the SPR assay, showed no off-rate at all during the limits of the experiment, putting its binding constant somewhere in the femtomolar range at worst. It comes in with IC50s of 120 picomolar in the pseudovirus assay and about 50 picomolar in the wild-type infection assay, but those are probably at the limit of detection for both. Basically, we don’t actually know how potent this nanobody construct is, because we don’t have assays good enough to read out a number (!)
Potential Therapeutic?
OK, now things get interesting. The authors tested the stability of mNb6-tri, and found that it can be heated, lyophilized (freeze-dried, basically), and nebulized into an aerosol with no loss of potency. It’s a very stable species that can put up with all sorts of handling and processing. You could certainly inject this material, just as you’d administer monocolonal antibodies. But there are more possibilities. How about formulating it as a nasal spray? Or in a nebulizer, to be breathed into the lungs, or even sprayed out into the room air? How about impregnating filter material with this protein so it pulls coronavirus particles out of the air as they pass through it? The extreme stability of nanobody proteins gives all of these a real shot, and they’re under serious consideration for development. The team says that they’re in discussion with several commercial partners to take this technology into human trials (and presumably medical-device trials, for the filtration idea), and I think that’s an excellent idea. This has real public-health potential, from the looks of it, and could be just the backup that we may need for the existing vaccine programs if they come in less effective than we’d like (or are rolled out more slowly than we’d like!) I hope that the money and resources are rounded up quickly.
I have a feeling that a side benefit of all the research into fighting this corona virus could result in a cure for the common cold.
Turns out that researchers at Mt. Sinai Hospital are in trials with a formula that they think can reduce covid-19 symptoms to that of a common cold. So if their trials are successful, and we find a cure for the common cold, we'll be in great shape!I have a feeling that a side benefit of all the research into fighting this corona virus could result in a cure for the common cold.
https://www.pharmaceutical-technology.com/news/study-fenofibrate-covid-19/
The Good (But Not Great) News About T-Cells and Herd Immunity
https://nymag.com/intelligencer/202...19-optimism-on-t-cells-and-herd-immunity.html
That's a great article. Balanced and insightful. Explores many of the concepts we've been talking about, since I first posted about T-cell cross-reactivity in early May and as per your previous posts highlighting the work on heterogeneity/modeling indicating "herd immunity" could be reached at much lower total infection levels in the population. As per the 2nd post in this thread, figuring all of this out is still maybe the most important scientific question that needs answering with regard to how many people will truly become infected and when is "herd immunity" reached.
I wish we could do viral "challenges" of people who have various levels of such T-cells which show activity against COVID, despite these people never having been exposed to SARS-CoV-2, so we could answer the question of how much immunity they have, but that won't happen ethically. Maybe we could "mine" the data from pre-COVID blood donor levels of such T-cells and find out what % of these people actually became infected vs. the general population.
The excerpt below also highlights the issues I've had with the heterogeneity work, as real world results appear to contradict infection "caps" on populations, although maybe the T-cell response observations mean we need a different "definition" of herd immunity, where perhaps we need to think about there being some cap of X% of a population that can become seriously ill, even if far more can become infected. Who knows - this stuff is driving me a little batty, lol.
But for those hoping that 25 percent represents a true ceiling for pandemic spread in a given community, well, it almost certainly does not, considering that recent serological surveys have shown that perhaps 93 percent of the population of Iquitos, Peru, has contracted the disease; as have more than half of those living in Indian slums; and as many as 68 percent in particular neighborhoods of New York City. And though there is some risk of herd-immunity “overshoot,” as Carl Bergstrom and Natalie Dean warned back in early May while contemplating the Swedish no-lockdown strategy and the risks of rushing to herd immunity, overshoot of that scale would seem unlikely if the “true” threshold were as low as 20 or 25 percent.
- Status
- Not open for further replies.
Similar threads
- Replies
- 592
- Views
- 15K
- Replies
- 80
- Views
- 2K
- Replies
- 608
- Views
- 17K
- Replies
- 280
- Views
- 6K
- Replies
- 139
- Views
- 3K
ADVERTISEMENT
ADVERTISEMENT