[
Editorial
October 12, 2020
Excess Deaths and the Great Pandemic of 2020
Howard Bauchner, MD1;
Phil B. Fontanarosa, MD, MBA1
Author Affiliations
Article Information
JAMA. 2020;324(15):1504-1505. doi:10.1001/jama.2020.20016
COVID-19 Resource Center
editorial comment icon
Editorial
Comment
related articles icon
Related
Articles
multimedia icon
Multimedia
Video (2:24)
Excess Deaths During the Coronavirus Pandemic
Two new reports in
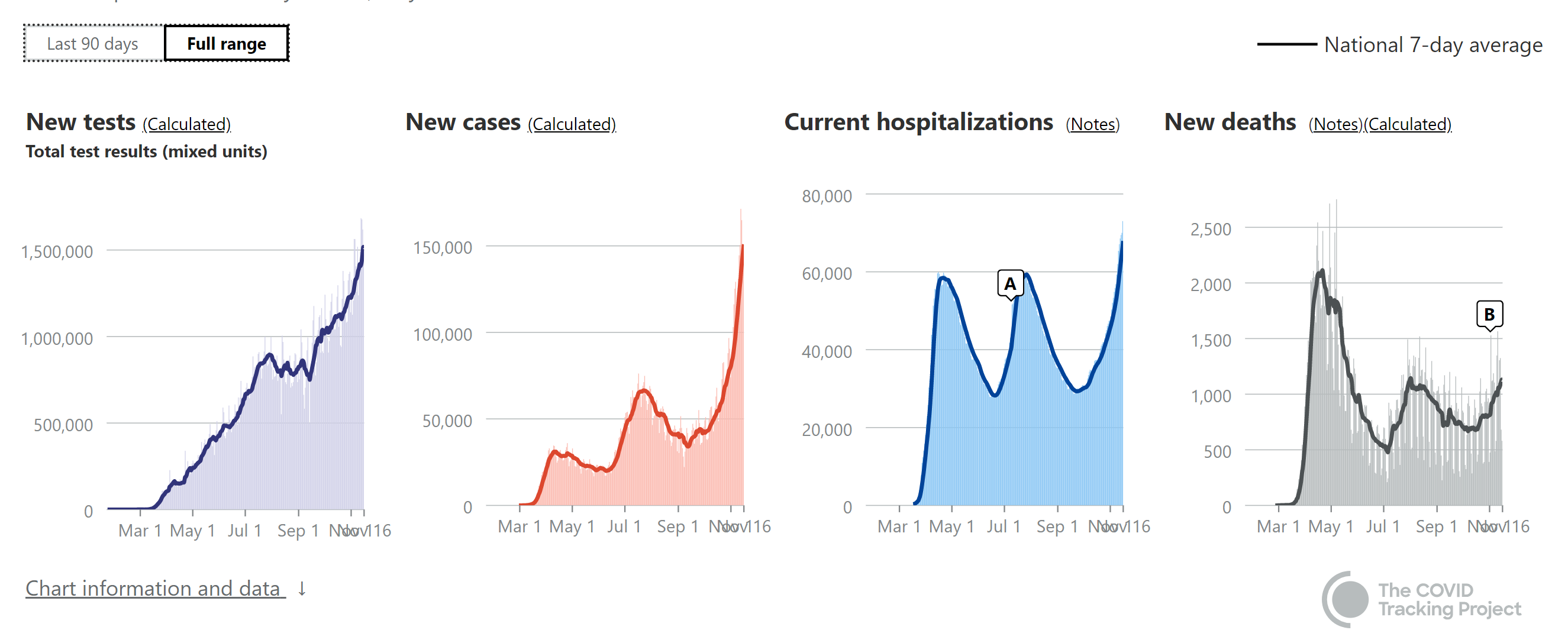
JAMA provide updated estimates regarding the mortality associated with the coronavirus disease 2019 (COVID-19) pandemic in the US. In a research letter by Woolf and colleagues, the authors update their analysis of the number of “excess” deaths in the US related to COVID-19 and other causes from March 1 through August 1, 2020.
1,
2 The authors report that during this 5-month period, a total of 1 336 561 deaths occurred in the US, an estimated 20% increase compared with the number of expected deaths, and representing 225 530 excess deaths.
2 Approximately 67% of these excess deaths were attributable directly to COVID-19, whereas excess deaths attributed to other causes also could have been related to the pandemic in general.
A second research letter, by Bilinski and Emanuel,
3 compared the US to Organisation for Economic Co-operation and Development countries with populations exceeding 5 million. The authors found that since the beginning of the pandemic, among the countries with moderate mortality (n = 8; COVID-19 deaths, 5-25/100 000) or high mortality (n = 7; COVID-19 deaths, >25/100 00), the US ranked third, with 71.6 deaths/100 000.
The importance of the estimate by Woolf et al—which suggests that for the entirety of 2020, more than 400 000 excess deaths will occur—cannot be overstated, because it accounts for what could be declines in some causes of death, like motor vehicle crashes, but increases in others, like myocardial infarction. These deaths reflect a true measure of the human cost of the Great Pandemic of 2020. As depicted in the illustration, these deaths far exceed the number of US deaths from some armed conflicts, such as the Korean War and the Vietnam War, and deaths from the 2009 H1N1 (Swine flu) pandemic, and approach the number of deaths from World War II.
In the report by Bilinski and Emanuel,
3 the authors note that the US experienced high COVID-19–associated mortality and excess all-cause mortality into September 2020. After the initial peak in early spring, US death rates from COVID-19 and from all causes remained higher than rates in countries with high COVID-19 mortality.
In addition, 3 Viewpoints and an Editorial in
JAMA reflect on the mental health, financial, and disparities issues related to the pandemic.
Simon and colleagues
4 suggest that it is critical to consider that for every death, an estimated 9 family members are affected, such as with prolonged grief or symptoms of posttraumatic stress disorder. In other words, approximately 3.5 million people could develop major mental health needs. This does not account for the thousands of health care workers in hospitals and nursing homes who have been witness to the unimaginable morbidity and mortality associated with COVID-19.
Cooper and Williams
5 comment on the unrelenting and seemingly intractable and embedded disparities that exist in the US and within the US health care system. They call for restorative justice. This issue is not new, but rather the COVID-19 pandemic has once again highlighted and further compounded the health, social, and economic disparities inherent in communities of color.
5,
6
Cutler and Summers
7 suggest that the COVID-19 pandemic represents the greatest threat to prosperity and well-being that the US has encountered since the Great Depression that began in 1929. The authors estimated the total financial cost of the pandemic—related to lost economic output and losses related to health—at $16 trillion, or approximately 90% of the annual US gross domestic product (GDP). The estimated economic loss from COVID-19 is a staggering number, but was largely preventable, and will reverberate through society for years to come.
In an accompanying Editorial, Fineberg underscores the key ideas of the Viewpoints by Simon et al, Cooper and Williams, and Cutler and Summers, and summarizes the findings of the report by Woolf et al highlighting that the data on excess deaths related to COVID-19 are “sufficiently mortifying and motivating.”
8 He also emphasizes that “an intense, persistent, multipronged, and coherent response must be the order of the day and an urgent priority for the nation.”
8
Few people will forget the Great Pandemic of 2020, where and how they lived, how it substantially changed their lives, and for many, the profound human toll it has taken.
Back to top
Article Information
Corresponding Author: Howard Bauchner, MD,
JAMA (
Howard.Bauchner@jamanetwork.org).
Published Online: October 12, 2020. doi:
10.1001/jama.2020.20016
Conflict of Interest Disclosures: None reported.
References
1.
Woolf SH, Chapman DA, Sabo RT, Weinberger DM, Hill L. Excess deaths from COVID-19 and other causes, March-April 2020.
JAMA. 2020;324(5):510-513. doi:
10.1001/jama.2020.11787
ArticlePubMedGoogle ScholarCrossref
2.
Woolf SH, Chapman DA, Sabo RT, et al. Excess deaths from COVID-19 and other causes, March-July 2020.
JAMA. Published online October 12, 2020. doi:
10.1001/jama.2020.19545
ArticleGoogle Scholar
3.
Bilinski A, Emanuel EJ. COVID-19 and excess all-cause mortality in the US and 18 comparison countries.
JAMA. Published online October 12, 2020. doi:
10.1001/jama.2020.20717
ArticleGoogle Scholar
4.
Simon NM, Saxe GN, Marmar CR. Mental health disorders related to COVID-19–related deaths.
JAMA. Published online October 12, 2020. doi:
10.1001/jama.2020.19632
ArticleGoogle Scholar
5.
Cooper LA, Williams DR. Excess deaths from COVID-19, community bereavement, and restorative justice for communities of color.
JAMA. Published online October 12, 2020. doi:
10.1001/jama.2020.19567
ArticleGoogle Scholar
6.
Wadhera RK, Wadhera P, Gaba P, et al. Variation in COVID-19 hospitalizations and deaths across New York City boroughs.
JAMA. 2020;323(21):2192-2195. doi:
10.1001/jama.2020.7197
ArticlePubMedGoogle ScholarCrossref
7.
Cutler DM, Summers LH. The COVID-19 pandemic and the $16 trillion virus.
JAMA. Published online October 12, 2020. doi:
10.1001/jama.2020.19759
ArticleGoogle Scholar
8.
Fineberg HV. The toll of COVID-19.
JAMA. Published online October 12, 2020. doi:
10.1001/jama.2020.20019
ArticleGoogle Scholar
Comment
1 Comment for this article
October 13, 2020
Death analysis during Covid-19 pandemic
Khichar Shubhakaran, MD(Med), D.M.(Neurology) | Senior Professor and Head of Department of Neurology, MDM Hospital, Dr.S. N. Medical College, Jodhpur(Rajasthan), India-342003
This is probably the right step to analyse the ,mortality during Covid-19 pandemic which will enable us in identify the direct and indirect deaths due to Covid-19 pandemic. The analysis of such data from different ares across the globe and their correlation with available healthcare resources will facilitate the way we tackle the situation and its further consequences so as to plan future strategies.
CONFLICT OF INTEREST: None Reported
See More About
Population Health Public Health Coronavirus (COVID19)
Coronavirus Resource Center
Trending
Select Your Interests
JOB LISTINGS ON JAMA CAREER CENTER®
CLINICAL FACULTY: BARIATRIC MEDICINEPhoenix, Arizona
ICU TRAINED PHYSICIANS and HOSPITALISTS: Urgent Help Needed in ICU's with Banner Health in AZ and CO(Phoenix – Tucson – Northern Colorado Front Range)
Nocturnist - Critical Care Intensivist OpportunityLynchburg, VA
Executive Medical Director Primary CareLynchburg, VA
MEDICAL DIRECTOR: CARE MANAGEMENT - Banner Health - Phoenix, ArizonaPhoenix, Arizona
See more at JAMA Career Center
Others Also Liked
- Deaths spike 20% in U.S. during 4-month period
Healio
- Excess mortality from COVID-19 in NYC comparable to peak of 1918 flu pandemic
Healio
- Prevalence of diabetes, hypertension among COVID-19 patients likely lower than reported
By Michael Monostra, Healio, 2020
Powered by
Trending
JAMA
JAMA Network
Help
Get the latest from JAMA
Sign Up
Privacy Policy |
Terms of Use
© 2020 American Medical Association. All Rights Reserved.
Terms of Use|
Privacy Policy|
Accessibility Statement
Our website uses cookies to enhance your experience. By continuing to use our site, or clicking "Continue," you are agreeing to our
Cookie Policy |
Continue