
He's been angry for much longer than that. He's the biggest snowflake of them all. Just overly ridiculous outrage at everything. He's not really credible to anyone but the hard-core trumpers. He's been around for years and hasn't sponsored a single piece of legislation that has actually passed.[/. Well , if your talking hardcore party allegiances, then you understand what party Fauci is aligned with . It is why he avoids a particular topic or plays the , “ I don’t know understand what you mean question.” I do give Tony credit for his honesty when asked those 3 questions about shutting down travel and if he was part of the decisions and that doing so saved lives. Pretty forthright in his statements.
Colleges
- American Athletic
- Atlantic Coast
- Big 12
- Big East
- Big Ten
- Colonial
- Conference USA
- Independents (FBS)
- Junior College
- Mountain West
- Northeast
- Pac-12
- Patriot League
- Pioneer League
- Southeastern
- Sun Belt
- Army
- Charlotte
- East Carolina
- Florida Atlantic
- Memphis
- Navy
- North Texas
- Rice
- South Florida
- Temple
- Tulane
- Tulsa
- UAB
- UTSA
- Boston College
- California
- Clemson
- Duke
- Florida State
- Georgia Tech
- Louisville
- Miami (FL)
- North Carolina
- North Carolina State
- Pittsburgh
- Southern Methodist
- Stanford
- Syracuse
- Virginia
- Virginia Tech
- Wake Forest
- Arizona
- Arizona State
- Baylor
- Brigham Young
- Cincinnati
- Colorado
- Houston
- Iowa State
- Kansas
- Kansas State
- Oklahoma State
- TCU
- Texas Tech
- UCF
- Utah
- West Virginia
- Illinois
- Indiana
- Iowa
- Maryland
- Michigan
- Michigan State
- Minnesota
- Nebraska
- Northwestern
- Ohio State
- Oregon
- Penn State
- Purdue
- Rutgers
- UCLA
- USC
- Washington
- Wisconsin
High Schools
- Illinois HS Sports
- Indiana HS Sports
- Iowa HS Sports
- Kansas HS Sports
- Michigan HS Sports
- Minnesota HS Sports
- Missouri HS Sports
- Nebraska HS Sports
- Oklahoma HS Sports
- Texas HS Hoops
- Texas HS Sports
- Wisconsin HS Sports
- Cincinnati HS Sports
- Delaware
- Maryland HS Sports
- New Jersey HS Hoops
- New Jersey HS Sports
- NYC HS Hoops
- Ohio HS Sports
- Pennsylvania HS Sports
- Virginia HS Sports
- West Virginia HS Sports
ADVERTISEMENT
COVID-19 Pandemic: Transmissions, Deaths, Treatments, Vaccines, Interventions and More...
- Thread starter Richie O
- Start date
- Status
- Not open for further replies.
Thought this was a good article on Antibodies and how decreasing levels doesn’t equal decreasing immunity.
https://www.nytimes.com/2020/07/31/...s-immunity.html#click=https://t.co/s243mF4NqU
https://www.nytimes.com/2020/07/31/...s-immunity.html#click=https://t.co/s243mF4NqU

Huge outbreak in late June at a Georgia camp for kids aged 6-19 with 260 of 597 attendees testing positive (of 344 tested) for COVID within 4 days of opening the camp, which was then closed. Masks were not required for the kids and there were many high risk activities for transmission (singing, cheering, and simply being in close quarters for extended periods without masks).
https://www.cdc.gov/mmwr/volumes/69/wr/mm6931e1.htm
These findings demonstrate that SARS-CoV-2 spread efficiently in a youth-centric overnight setting, resulting in high attack rates among persons in all age groups, despite efforts by camp officials to implement most recommended strategies to prevent transmission. Asymptomatic infection was common and potentially contributed to undetected transmission, as has been previously reported (1–4). This investigation adds to the body of evidence demonstrating that children of all ages are susceptible to SARS-CoV-2 infection (1–3) and, contrary to early reports (5,6), might play an important role in transmission (7,8). The multiple measures adopted by the camp were not sufficient to prevent an outbreak in the context of substantial community transmission. Relatively large cohorts sleeping in the same cabin and engaging in regular singing and cheering likely contributed to transmission (9). Use of cloth masks, which has been shown to reduce the risk for infection (10), was not universal. An ongoing investigation will further characterize specific exposures associated with infection, illness course, and any secondary transmission to household members. Physical distancing and consistent and correct use of cloth masks should be emphasized as important strategies for mitigating transmission in congregate settings.
https://www.cdc.gov/mmwr/volumes/69/wr/mm6931e1.htm
These findings demonstrate that SARS-CoV-2 spread efficiently in a youth-centric overnight setting, resulting in high attack rates among persons in all age groups, despite efforts by camp officials to implement most recommended strategies to prevent transmission. Asymptomatic infection was common and potentially contributed to undetected transmission, as has been previously reported (1–4). This investigation adds to the body of evidence demonstrating that children of all ages are susceptible to SARS-CoV-2 infection (1–3) and, contrary to early reports (5,6), might play an important role in transmission (7,8). The multiple measures adopted by the camp were not sufficient to prevent an outbreak in the context of substantial community transmission. Relatively large cohorts sleeping in the same cabin and engaging in regular singing and cheering likely contributed to transmission (9). Use of cloth masks, which has been shown to reduce the risk for infection (10), was not universal. An ongoing investigation will further characterize specific exposures associated with infection, illness course, and any secondary transmission to household members. Physical distancing and consistent and correct use of cloth masks should be emphasized as important strategies for mitigating transmission in congregate settings.
Thought this was a good article on Antibodies and how decreasing levels doesn’t equal decreasing immunity.
https://www.nytimes.com/2020/07/31/...s-immunity.html#click=https://t.co/s243mF4NqU
It's an excellent article, except somehow they missed including any discussion of the recent work at Mt. Sinai, under Dr. Krammer, and out of Wuhan by some Chinese scientists, showing robust antibody responses lasting 3 months, so far in the US study and 6 months so far in the Chinese study, both of which were far larger than the earlier studies questioning antibody response duration (links below). This is why I'm becoming even more optimistic for plasma (with some great data out yesterday, showing 57% mortality reduction), engineered antibodies at the end of the summer (a cure?), and vaccines by the end of the year.
While the above post was mostly on T-cells, there was a nugget in there about how some recent small scale studies have shown patient antibody levels decreasing over time significantly, including one in China with 37 recovered patients who had mild or asymptomatic infections. Well, today Dr. Krammer's group from Mt. Sinai, published a preprint of a paper where they've analyzed antibodies in nearly 20,000 mildly to moderately ill COVID patients (lots of infections in NYC!) and had this wonderfully pithy one sentence summary of the work, which is great news, particularly the part about antibody responses being stable for at least 3 months (the full abstract is below that). While this doesn't "guarantee" 3-month+ immunity in recovered patients or in vaccinated patients who achieve similar antibody levels, it's the way to bet.
One Sentence Summary: Antibody responses induced by natural mild-to-moderate SARS27 CoV-2 infection are robust, neutralizing and are stable for at least 3 months.
Abstract: SARS-CoV-2 has caused a global pandemic with millions infected and numerous fatalities. Questions regarding the robustness, functionality and longevity of the antibody response to the virus remain unanswered. Here we report that the vast majority of infected individuals with mild to-moderate COVID-19 experience robust IgG antibody responses against the viral spike protein, based on a dataset of 19,860 individuals screened at Mount Sinai Health System in New York City. We also show that titers are stable for at least a period approximating three months, and that anti-spike binding titers significantly correlate with neutralization of authentic SARS-CoV-2. Our data suggests that more than 90% of seroconverters make detectible neutralizing antibody responses and that these titers are stable for at least the near-term future.
Conclusion: Our data reveal that individuals who have recovered from mild COVID-19 experience robust antibody responses. Antibody binding titers to the spike protein correlate significantly with neutralization with authentic SARS-CoV-2 virus, and the vast majority of individuals with antibody titers of 1:320 or higher show neutralizing activity in their serum. Consistent with data for human coronaviruses, SARS-CoV-1 and Middle Eastern respiratory syndrome-CoV (23), we also find stable antibody titers over a period of at least 3 months, and we plan to follow this cohort over longer intervals of time. While this cannot provide conclusive evidence that these antibody responses protect from re-infection, we believe it is very likely that they will decrease the odds ratio of getting re-infected, and may attenuate disease in the case of breakthrough infection.
https://www.medrxiv.org/content/10.1101/2020.07.14.20151126v1.full.pdf
Looks like some additional big, positive antibody news in a paper that came out yesterday (preprint, so not peer-reviewed yet, but looks solid) confirming and extending Dr. Krammer's work at Mt. Sinai, posted above. A Chinese study on 349 of the earliest patients from Wuhan shows ~6 months of generally durable antibody response in the "vast majority" of convalescent patients (who recovered from COVID infections). This is very good news for recovered patients retaining immunity for 6 months or more and for any vaccines able to raise neutralizing antibody responses (which we have seen).
https://www.medrxiv.org/content/10.1101/2020.07.21.20159178v1.full.pdf
Abstract: Long-term antibody responses and neutralizing activities following SARS-CoV-2 infections have not yet been elucidated. We quantified immunoglobulin M (IgM) and G (IgG) antibodies recognizing the SARS-CoV-2 receptor-binding domain (RBD) of the spike (S) or the nucleocapsid (N) protein, and neutralizing antibodies during a period of six months following COVID-19 disease onset in 349 symptomatic COVID-19 patients, which were among the first world-wide being infected. The positivity rate and magnitude of IgM-S and IgG-N responses increased rapidly. High levels of IgMS/N and IgG-S/N at 2-3 weeks after disease onset were associated with virus control and IgG-S titers correlated closely with the capacity to neutralize SARS-CoV-2. While specific IgM-S/N became undetectable 12 weeks after disease onset in most patients, IgG-S/N titers showed an intermediate contraction phase, but stabilized at relatively high levels over the six months observation period. At late time points the positivity rates for binding and neutralizing SARS-CoV-2-specific antibodies was still over 70%. Taken together, our data indicate sustained humoral immunity in recovered patients who suffer from symptomatic COVID-19, suggesting prolonged immunity.
Conclusion: In conclusion, antibodies appear to have antiviral effects in the early stages of SARS-CoV-2 infection; and the most symptomatic patients with COVID-19 remain positive for IgG-S and exhibit sufficient neutralizing activity at six months after the onset of illness. These results support the notion that naturally infected patients have the ability to combat re-infection and vaccines may be able to produce sufficient protection. Please note, that analyses which terminated their observation earlier than ours and extrapolates the long-term trend based on this contraction phase without considering or determining the consolidation phase, bear the inherent risk to come to wrong over-pessimistic conclusions concerning the durability of humoral immune responses.
Hindsight being 20/20 what would you have done?Nobody has disputed where the outbreak started. Most of the rest of your post is pure conjecture unsupported by anything resembling substantiated facts.
To claim there was nothing we could have done to limit the spread of the infection, or to learn about how to treat it, or get a head-start on vaccines... that's so obviously false that there's nothing polite that can be said about it.
But for sure, such fact-less conjecture helps deflect from the tremendously poor national response to the virus. Pure misinformation that leaves no room for self-reflection and self-improvement.
Anyone with a shred of intellectual honesty should watch this video and learn why some notable scientists have strong doubts about a natural origin. For those who have none, carry on as you were.
Good that you edited your post. I watched and they're simply saying the same things that Chris Martenson said in his video which you posted awhile back trying to "prove" the same thing. As I said back then, it'll never be possible to "prove" the virus couldn't have come from a lab (nearly impossible to prove a "negative"), but the papers/arguments I've read have convinced me (and more importantly, the vast majority of virology/evolutionary biology experts) that it's extraordinarily unlikely. We've already seen how wrong Martenson was on HCQ and he and these guys are just as wrong on the origin of the novel coronavirus.
I also think it's really dumb to have cut off collaboration with Chinese scientists. Even if one is suspicious of them, I'd rather keep working with them on the probability that they're being honest and I'd also want to keep working with them if I didn't trust them (keep your friends close and your enemies closer). I think the kind of global scientific cooperation we're seeing for the most part now is fantastic and will help get us out of this mess soon and will be needed to try to do a lot more surveillance of future pandemic threats, especially from China.
Below are a couple of posts on this from back then, which go into great detail on several of the elements Martenson and now these guys highlight. The one thing I'll give these guys credit for is not overdoing it, like Martenson did, as they both were careful to not say they "know" SARS-CoV-2 was either lab generated or brought to the lab from the wild and accidentally released.
One other thing: these "Dark Intellectual Web" guys love getting people riled up with nutty conspiracy theories, but none of them ever publishes anything. The reason they don't is they know they'd be torn to shreds by the real experts, so they prefer to sit back and post their theories and influence the intellectually susceptible, who will never question them.
With regard to new information, see the link below, with a long article/interview about/with Shi Zhengli, the Chinese researcher known as the "batwoman" who many have pointed to as a possible culprit for any lab shenanigans. She said the following:
- They first received actual SARS-CoV-2 samples in late December from patients
- They've never worked with any viruses that are that close genetically to CV2 - even the RaTG13 bat coronavirus (the closest) only shares 96.2% of its genetic material witih CV2, which is actually pretty far off from a match (humans and chimps share 98%) - she and others have said that their differences suggest these two viruses diverged evolutionarily 20-70 years ago. They spent much of their time investigating variants of SARS, since that was what they were most worried about.
- She also explained the naming issue with RaTG13 and its original name, 4991 - they're identical with the former being a better identifier of sample collection time and location.
- She also doubts the Wuhan wet market is the origin of CV2, thinking that's just where many of the cases started, but that it likely started somewhere else and was brought to Wuhan.
- Her answers to Science were reviewed by Chinese authorities (as they likely would be in any other country's govt. lab), but the experts Science spoke with feel the answers were logical and helpful. Doesn't mean everyone will believe her though.
https://rutgers.forums.rivals.com/t...entions-and-more.191275/page-112#post-4558420
https://rutgers.forums.rivals.com/t...entions-and-more.191275/page-110#post-4556128
because we are going to find out masks dont stop the spread.....hence why everyone is suggest eye goggles this week after 3 months of not addressing it.
More failure, randomness, or hypocrisy from Fauci and Birx. I think all these so called experts have no idea what is going on and how its spread right now, its spreading regardless
These people dont know their asses from their elbows.
Fauci answering questions any typical 3rd grader could do is a genius in his own medium.
Let me get this straight...Covid supposedly originated in Wuhan where there is a highly, secretive lab which not only specializes in bat coronavirus, but is funded by the US? Reports say deadly bat virus has a 50 year evolution to jump from animal to human and was not sold in the Wuhan markets? And yet not many people think this escaped from a lab in Wuhan either intentionally or unintentionally?
I don't know what the point would be. If CCP released the virus on purpose I could see using "an accident" as a cover-up, but as things are, it just seems like China authorities knew they had an accident and A) concealed it and B) made sure the virus spread so they they wouldn't be only one hammered but i.
It could just be China being selfish and sly. They are not above any tactic..
Its like a neighbor who really wants a fence.. but waits for his side and back neighbors to put theirs up.
China could very well be the victim of virus after virus.. because of wet markets or poor security in research facilities.. and now the seeds and dirt being delivered along with random products ordered from China on ebay or other online sources? Maybe the dragonfish thing is another example of the same thing..
That is.. China has a problem.. doesn't have the skill or desire to use resources to solve the problem.. so they spread the pain to the west and the west solves the problem for them.
Even if this is their "innocent" goal.. this is the same thing as their hacking.. it is a shadow war.. a cold war. It is asymmetric warfare because they don't expect us to respond in kind.. they have deniability.. or paid enough people in power to buy lack of accountability.
Last edited:
Should the "not" be a "now?"Let me get this straight...Covid supposedly originated in Wuhan where there is a highly, secretive lab which not only specializes in bat coronavirus, but is funded by the US? Reports say deadly bat virus has a 50 year evolution to jump from animal to human and was not sold in the Wuhan markets? And yet not many people think this escaped from a lab in Wuhan either intentionally or unintentionally?
If I may answer for my friend, @mildone, I think he would've stocked up on COVID-free hookers and blow and had a much better time of it...Hindsight being 20/20 what would you have done?
Last edited:
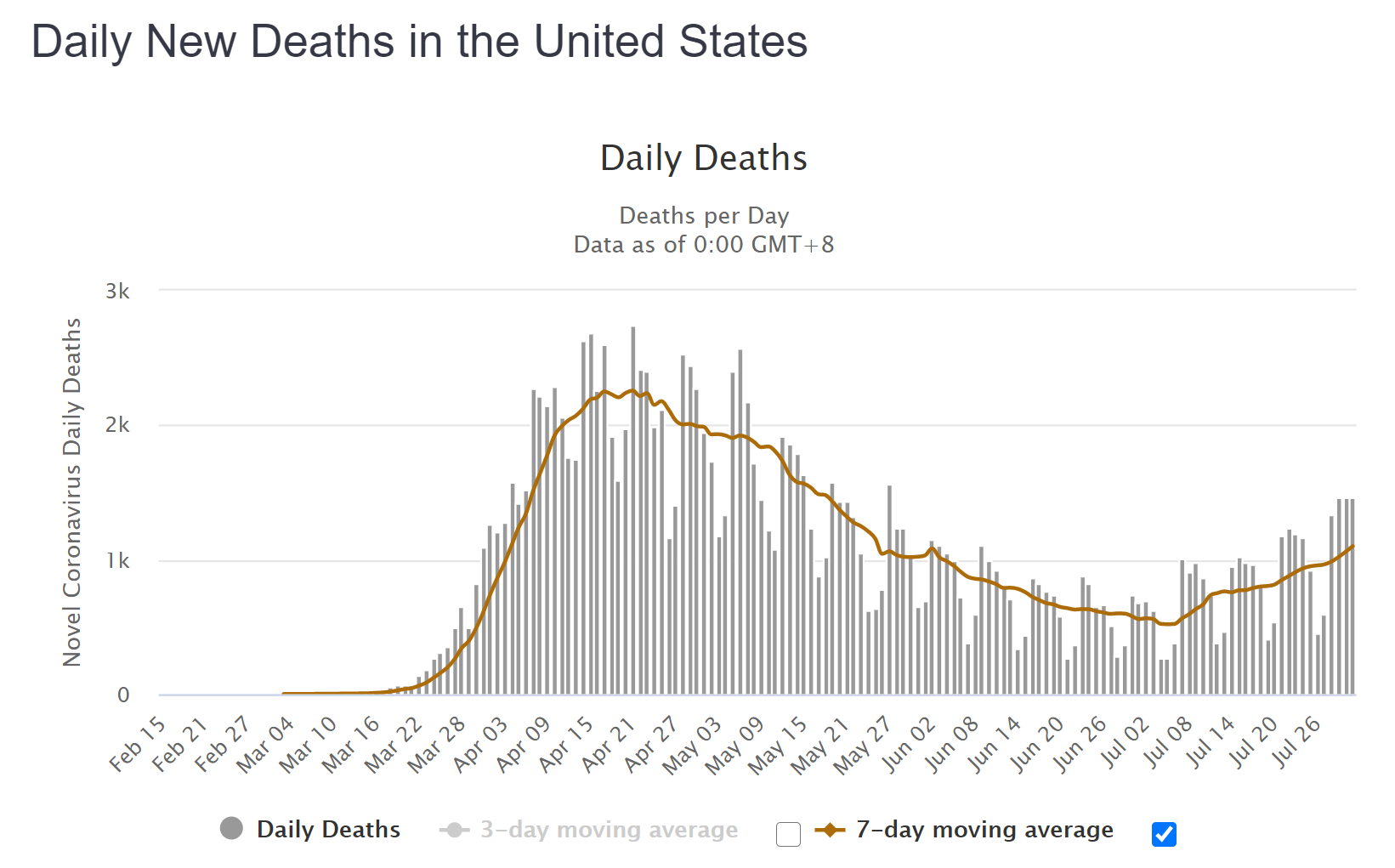
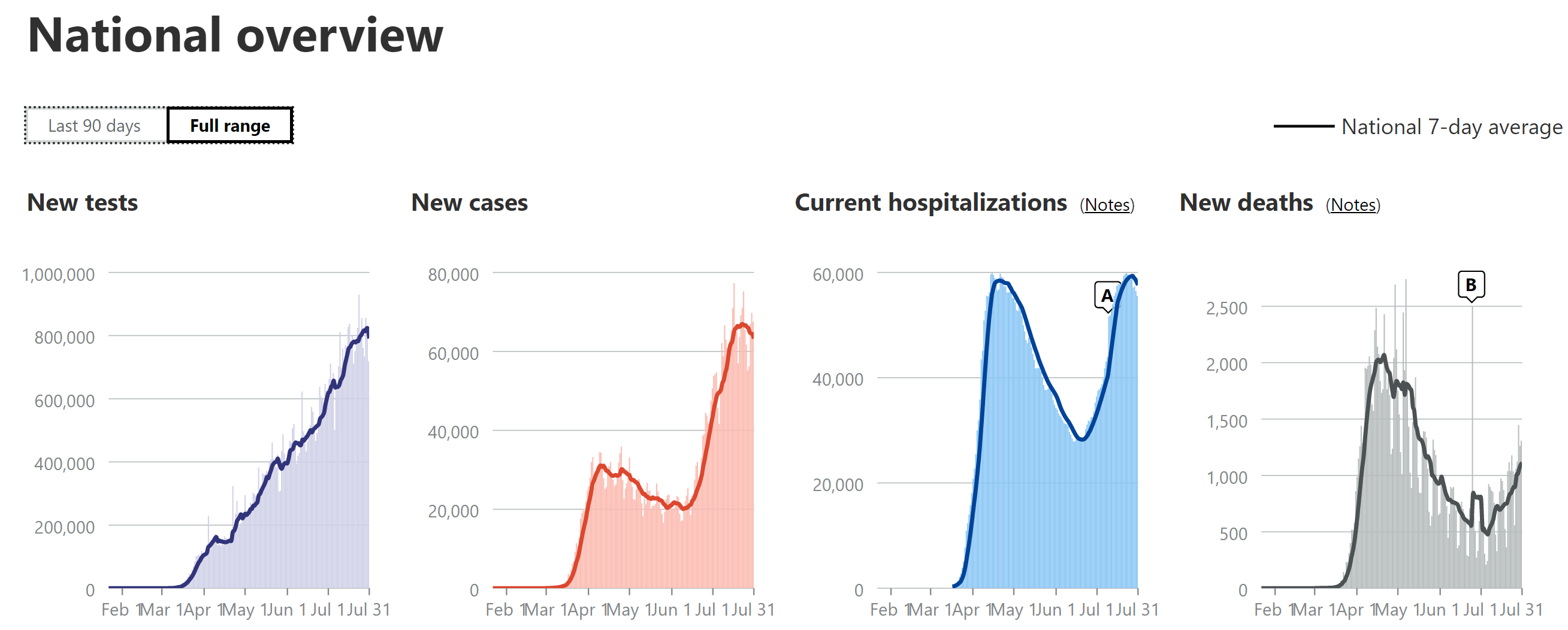
Below is the Worldometers detailed graphic of US deaths and the COVID Tracking charts of US tests, cases, hospitalizations, and deaths, all on 7-day moving averages. Not a great day, as Worldometers reported that we tied yesterday's record high in deaths for wave 2, with 1465, although COVID Tracking had a drop from 1447 yesterday to 1262 today. Regardless, the 7-day moving average continues its steady climb and is now around 1060 per day in both sources. Cases were up again today to over 68K, so the 7-day MA is still in a peak plateau and hospitalizations appear to be at their peak.
With regard to highlights from states, Arizona reported record high of 158 new deaths and Florida set another record today (3 days in a row), hitting 253 deaths; California dropped from their record of 192 on Wednesday to 114 deaths today. Texas continues with funky data reporting a record 322 on WM, but only 84 on CT - this is all in relation to how they're incorporating that 600 death increase, 225 of which were in error, supposedly (bottom line is deaths are increasing still).
https://www.worldometers.info/coronavirus/country/us
https://covidtracking.com/data#chart-annotations


Below is the Worldometers detailed graphic of US deaths and the COVID Tracking charts of US tests, cases, hospitalizations, and deaths, all on 7-day moving averages. Another bad day, as Worldometers reported that we almost tied yesterday's record high in deaths for wave 2 (1465), with 1462 deaths, although COVID Tracking only reported 1308 today. Regardless, the 7-day moving average continues its steady climb and is now around 1100 per day in both sources.
Cases were up again today to over 71K, despite drops in FL/TX/CA, which had been driving the increases, meaning other states are starting to accelerate more. The 7-day MA is still in a peak plateau and hospitalizations appear to be at their peak, also.
With regard to highlights from states, California set another new high 191 deaths, today, as did Florida, with 256 deaths, while Texas was just below their WM high. In addition, Mississippi, Nevada, Idaho, and Montana all set new records for deaths.
https://www.worldometers.info/coronavirus/country/us
https://covidtracking.com/data#chart-annotations
I'll stick with the Rutgers guy:Good that you edited your post. I watched and they're simply saying the same things that Chris Martenson said in his video which you posted awhile back trying to "prove" the same thing. As I said back then, it'll never be possible to "prove" the virus couldn't have come from a lab (nearly impossible to prove a "negative"), but the papers/arguments I've read have convinced me (and more importantly, the vast majority of virology/evolutionary biology experts) that it's extraordinarily unlikely. We've already seen how wrong Martenson was on HCQ and he and these guys are just as wrong on the origin of the novel coronavirus.
I also think it's really dumb to have cut off collaboration with Chinese scientists. Even if one is suspicious of them, I'd rather keep working with them on the probability that they're being honest and I'd also want to keep working with them if I didn't trust them (keep your friends close and your enemies closer). I think the kind of global scientific cooperation we're seeing for the most part now is fantastic and will help get us out of this mess soon and will be needed to try to do a lot more surveillance of future pandemic threats, especially from China.
Below are a couple of posts on this from back then, which go into great detail on several of the elements Martenson and now these guys highlight. The one thing I'll give these guys credit for is not overdoing it, like Martenson did, as they both were careful to not say they "know" SARS-CoV-2 was either lab generated or brought to the lab from the wild and accidentally released.
One other thing: these "Dark Intellectual Web" guys love getting people riled up with nutty conspiracy theories, but none of them ever publishes anything. The reason they don't is they know they'd be torn to shreds by the real experts, so they prefer to sit back and post their theories and influence the intellectually susceptible, who will never question them.
With regard to new information, see the link below, with a long article/interview about/with Shi Zhengli, the Chinese researcher known as the "batwoman" who many have pointed to as a possible culprit for any lab shenanigans. She said the following:
https://www.sciencemag.org/news/202...st-center-covid-19-origin-theories-speaks-out
- They first received actual SARS-CoV-2 samples in late December from patients
- They've never worked with any viruses that are that close genetically to CV2 - even the RaTG13 bat coronavirus (the closest) only shares 96.2% of its genetic material witih CV2, which is actually pretty far off from a match (humans and chimps share 98%) - she and others have said that their differences suggest these two viruses diverged evolutionarily 20-70 years ago. They spent much of their time investigating variants of SARS, since that was what they were most worried about.
- She also explained the naming issue with RaTG13 and its original name, 4991 - they're identical with the former being a better identifier of sample collection time and location.
- She also doubts the Wuhan wet market is the origin of CV2, thinking that's just where many of the cases started, but that it likely started somewhere else and was brought to Wuhan.
- Her answers to Science were reviewed by Chinese authorities (as they likely would be in any other country's govt. lab), but the experts Science spoke with feel the answers were logical and helpful. Doesn't mean everyone will believe her though.
https://rutgers.forums.rivals.com/t...entions-and-more.191275/page-112#post-4558420
https://rutgers.forums.rivals.com/t...entions-and-more.191275/page-110#post-4556128
However, Richard Ebright, a molecular biologist at Rutgers University, New Brunswick, who from the early days of the pandemic has urged that an investigation look into the possibility that SARS-CoV-2 entered humans through a laboratory accident, was decidedly unimpressed. “Most of these answers are formulaic, almost robotic, reiterations of statements previously made by Chinese authorities and state media,” Ebright says.
What is interesting to me is the relationship between new cases and hospitalizations over the April-July time span. To have a 30K/60K new case/hospitilazation ratio then morph into 65K/60K ratio must have more explanations than rising cases in younger people for whom hospitalizations are less frequent. There are several plausible reasons, already mentioned here as to why the death rate has declined (better treatments, protection of the elderly, younger infected persons etc) but to have a such a percentage dip of people being hospitalized suggests much. Have I missed any scientific studies depicting greater communicability and decreased lethality?Below is the Worldometers detailed graphic of US deaths and the COVID Tracking charts of US tests, cases, hospitalizations, and deaths, all on 7-day moving averages. Another bad day, as Worldometers reported that we almost tied yesterday's record high in deaths for wave 2 (1465), with 1462 deaths, although COVID Tracking only reported 1308 today. Regardless, the 7-day moving average continues its steady climb and is now around 1100 per day in both sources.
Cases were up again today to over 71K, despite drops in FL/TX/CA, which had been driving the increases, meaning other states are starting to accelerate more. The 7-day MA is still in a peak plateau and hospitalizations appear to be at their peak, also.
With regard to highlights from states, California set another new high 191 deaths, today, as did Florida, with 256 deaths, while Texas was just below their WM high. In addition, Mississippi, Nevada, Idaho, and Montana all set new records for deaths.
https://www.worldometers.info/coronavirus/country/us
https://covidtracking.com/data#chart-annotations
because we are going to find out masks dont stop the spread.....hence why everyone is suggest eye goggles this week after 3 months of not addressing it.
More failure, randomness, or hypocrisy from Fauci and Birx. I think all these so called experts have no idea what is going on and how its spread right now, its spreading regardless
Japan’s surge in cases shouldn’t be viewed as proof that masks are ineffective. Keep in mind three things: Japan has fully opened bars and restaurants dating back to May — you don’t eat or drink with a mask on. Tokyo gets very hot and humid in the summer — surge has coincided with when these places would be closed up and using AC too — no mask and recirculated air. Even outside of that environment masks are effective at reducing spread and transferred dose. Not perfect.
Obviously goggles and a mask is better than just a mask. A hazmat suit would be better than goggles and a mask. The idea with the mask is that it is effective low hanging fruit. My guess is we are not going to be mandated to wear goggles; maybe more people will adopt by choice.
What is interesting to me is the relationship between new cases and hospitalizations over the April-July time span. To have a 30K/60K new case/hospitilazation ratio then morph into 65K/60K ratio must have more explanations than rising cases in younger people for whom hospitalizations are less frequent. There are several plausible reasons, already mentioned here as to why the death rate has declined (better treatments, protection of the elderly, younger infected persons etc) but to have a such a percentage dip of people being hospitalized suggests much. Have I missed any scientific studies depicting greater communicability and decreased lethality?
I think the most likely driver (with other minor contributing factors) is that overtime we’ve built more testing capacity so the case count is inclusive of more mild cases. Our spring case totals are likely understated by a material amount
People still protecting The Almighty Mask just because the took a stance on it.Japan’s surge in cases shouldn’t be viewed as proof that masks are ineffective. Keep in mind three things: Japan has fully opened bars and restaurants dating back to May — you don’t eat or drink with a mask on. Tokyo gets very hot and humid in the summer — surge has coincided with when these places would be closed up and using AC too — no mask and recirculated air. Even outside of that environment masks are effective at reducing spread and transferred dose. Not perfect.
Obviously goggles and a mask is better than just a mask. A hazmat suit would be better than goggles and a mask. The idea with the mask is that it is effective low hanging fruit. My guess is we are not going to be mandated to wear goggles; maybe more people will adopt by choice.
https://www.reuters.com/article/us-health-coronavirus-russia-vaccine-idUSKBN24X3KO
Russian vaccine completed “safety” trials and mass vaccination slated to begin in October. What I find interesting is that previously Russia stated they wouod vaccinate the military first. Now they are saying doctors and teachers.
Russian vaccine completed “safety” trials and mass vaccination slated to begin in October. What I find interesting is that previously Russia stated they wouod vaccinate the military first. Now they are saying doctors and teachers.
https://www.reuters.com/article/us-health-coronavirus-russia-vaccine-idUSKBN24X3KO
Russian vaccine completed “safety” trials and mass vaccination slated to begin in October. What I find interesting is that previously Russia stated they wouod vaccinate the military first. Now they are saying doctors and teachers.
I wonder when their clinical trials started and with how many people. I bet they did human challenges as well. Depending on this, what they are doing might not be too crazy.
What is interesting to me is the relationship between new cases and hospitalizations over the April-July time span. To have a 30K/60K new case/hospitilazation ratio then morph into 65K/60K ratio must have more explanations than rising cases in younger people for whom hospitalizations are less frequent. There are several plausible reasons, already mentioned here as to why the death rate has declined (better treatments, protection of the elderly, younger infected persons etc) but to have a such a percentage dip of people being hospitalized suggests much. Have I missed any scientific studies depicting greater communicability and decreased lethality?
I don't think it's due to lethality being different, as I've discussed before. The lower hospitalization rate (about half of what was seen in the first wave) seems very likely due to the combination of younger infected population (much younger) and the higher percentage of mild/asymptomatic cases being found, due to more tests per case - the positivity rate in NY/NJ was in the 35-50% range for about a month during the worst part of the outbreak, as we only had enough tests for significantly symptomatic folks for quite awhile (have said this in previous posts, but not last night). This wave hasn't seen more than 20% positivity anywhere, consistently (see the graphs of all the states I've been doing on Tuesday nights). Haven't shared the NY graphic below in awhile, but it's pretty clear (theirs is a better graphic than NJ's, but they're similar).
Having roughly half the hospitalizations vs. cases in this wave vs. wave 1 would lead to maybe 1/2 the death rate, per capita, without any other changes from wave 1, but then improved procedures/treatments would lower that further. It's why I've been saying the peak death rates in places like AZ/FL/TX would be 1/3-2/3 of NJ's, per capita, for example (since before it was clear the hosp rate would be 1/2 - thought it might be 2/3) - looks like these will be more like 1/3-1/2 of NJ's. And CA's will likely be even lower (15% of NJ's, per capita), since they have a much lower case per capita rate than the other three, probably due to a more controlled reopening and better masking.
https://covid19tracker.health.ny.go...r-DailyTracker?:embed=yes&:toolbar=no&:tabs=n

Japan’s surge in cases shouldn’t be viewed as proof that masks are ineffective. Keep in mind three things: Japan has fully opened bars and restaurants dating back to May — you don’t eat or drink with a mask on. Tokyo gets very hot and humid in the summer — surge has coincided with when these places would be closed up and using AC too — no mask and recirculated air. Even outside of that environment masks are effective at reducing spread and transferred dose. Not perfect.
Obviously goggles and a mask is better than just a mask. A hazmat suit would be better than goggles and a mask. The idea with the mask is that it is effective low hanging fruit. My guess is we are not going to be mandated to wear goggles; maybe more people will adopt by choice.
Great post. If the eye route was more than minor and the aerosol transmission were as bad as some have said (I don't believe either is major), every front line worker wearing a mask, but not goggles, would be infected, as would all those subway riders in Seoul and Tokyo, who all wear masks, but not goggles. Goggles seem important where exposures are very high, like in ERs/COVID wards, which is why those folks usually wear goggles or facemasks.
Someday I'm going to build and patent my COVID "helmet" which seals at the neck and has a battery powered, HEPA filtered air supply (which will also keep it from fogging), and a headset with external speakers and receivers so people can talk to each other (at least if not in a crowd). This would allow all public events to resume. Only half kidding.
You'd be inconsistent if you didn't. He is a significant outlier, though.I'll stick with the Rutgers guy:
However, Richard Ebright, a molecular biologist at Rutgers University, New Brunswick, who from the early days of the pandemic has urged that an investigation look into the possibility that SARS-CoV-2 entered humans through a laboratory accident, was decidedly unimpressed. “Most of these answers are formulaic, almost robotic, reiterations of statements previously made by Chinese authorities and state media,” Ebright says.
https://www.reuters.com/article/us-health-coronavirus-russia-vaccine-idUSKBN24X3KO
Russian vaccine completed “safety” trials and mass vaccination slated to begin in October. What I find interesting is that previously Russia stated they wouod vaccinate the military first. Now they are saying doctors and teachers.
This article provides a little more info. They plan on releasing details of the initial trial soon. Honestly doesn’t sound too far fetched.
https://www.businessinsider.com/cnn-russia-races-to-approve-vaccine-within-next-two-weeks-2020-7
Many suggesting Covid 19 has become less severe. We’ll know in a few weeks.What is interesting to me is the relationship between new cases and hospitalizations over the April-July time span. To have a 30K/60K new case/hospitilazation ratio then morph into 65K/60K ratio must have more explanations than rising cases in younger people for whom hospitalizations are less frequent. There are several plausible reasons, already mentioned here as to why the death rate has declined (better treatments, protection of the elderly, younger infected persons etc) but to have a such a percentage dip of people being hospitalized suggests much. Have I missed any scientific studies depicting greater communicability and decreased lethality?
Sweden sure got it right. Shut downs and masks were idiotic.
Dear lord make it stop :flush:
RU 848789- if a treatment/cure is available late summer as we all hope, does that mean fans can attend football games? If a cure is discovered we should be good to go with caution of course.It's an excellent article, except somehow they missed including any discussion of the recent work at Mt. Sinai, under Dr. Krammer, and out of Wuhan by some Chinese scientists, showing robust antibody responses lasting 3 months, so far in the US study and 6 months so far in the Chinese study, both of which were far larger than the earlier studies questioning antibody response duration (links below). This is why I'm becoming even more optimistic for plasma (with some great data out yesterday, showing 57% mortality reduction), engineered antibodies at the end of the summer (a cure?), and vaccines by the end of the year.
RU 848789- if a treatment/cure is available late summer as we all hope, does that mean fans can attend football games? If a cure is discovered we should be good to go with caution of course.
Tough call. A treatment doesn't prevent infections, so my guess is it would depend on the degree of success of the treatment. If there were a treatment which meant infections never progressed to serious illness, then yeah, sure, it's back to normal life for most, I would think. However, if there were still some deaths and serious illnesses (very few "cures" are 100% effective), I'm not so sure - and we certainly would be reluctant to back off interventions before seeing if the "cure" was as effective in the general population as it was in a phase III clinical trial. But in the latter case I would certainly think having a near cure and wearing masks should allow for fans to attend football games, but that's just my opinion. Some may want to wait for a vaccine.
We need a treatment that can be given by doctors to keep people out of the hospital (e.g. pill or nasal spray). I don’t think anything will be ready for football season though. Antibody treatments will be ready in Oct/Nov (assuming they work in trials), and even then, there won’t be enough to go around for the general population. Remdesivir might be available as an inhaler this fall, but I don’t think that works well enough. There are a bunch other antivirals and treatments currently in trial, really need one of them to come back with impressive results. Gonna be a busy next couple of months with all the trial results coming back.
Exactly.
Also, the quote from Fauci doesn't say what the person on twitter who posted it is trying to make it out to have said.

The person on twitter would be Rep. Scalise, who was actually questioning the Fauc at the hearing. So what does the quote say if it's not what it actually says?
Last edited:
deaths are the highest they have been in over 2 months. It's not less severeMany suggesting Covid 19 has become less severe. We’ll know in a few weeks.
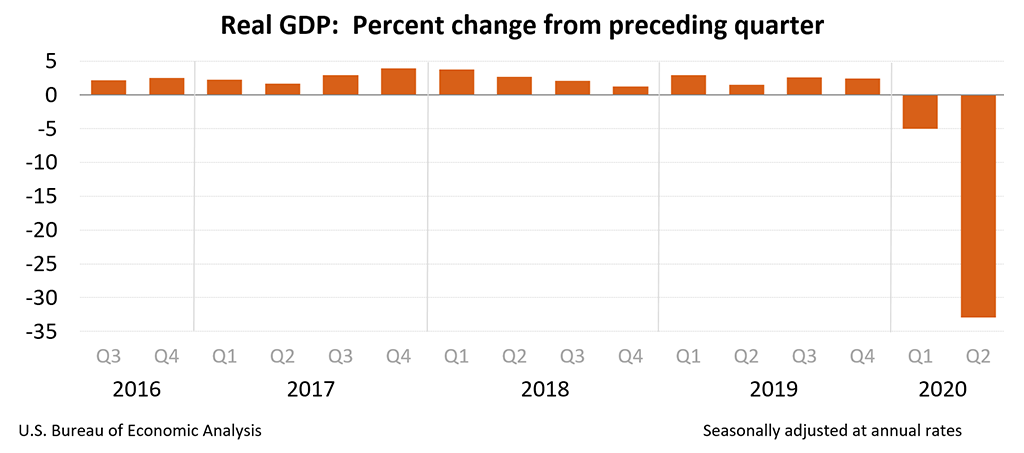
Eurozone economy shrinks by over 12% in Q2, again US quarterly fall was about 9.4%. Spain was really crushed down over 18%, France declined almost 14% and Italy dropped by 12%.When the US govt stops/slows pumping trillions in to the economy it is going to be worse than folks comprehend.
"Wages and salaries fell sharply in April, but that was more than offset by the $1,200 relief payments that the government sent to most adults and by supplemental unemployment benefits of $600 per week.
Those government payments helped prevent an even steeper drop in consumer spending — the lifeblood of the U.S. economy — and allowed struggling families to buy groceries and pay rent."
https://www.npr.org/sections/corona...witter.com&utm_campaign=npr&utm_medium=social
https://apnews.com/5ee44af8197a724cfb1ad16787275fbe
Came back from a drive down 206 in Hillsborough. Stopped at the light and looked to the car next to me and there was a man driving with gloves, a mask and a face shield closed at bottom and open at top. I did not see any hazardous material label on his car so I laughed and said WTF?
Good that you edited your post. I watched and they're simply saying the same things that Chris Martenson said in his video which you posted awhile back trying to "prove" the same thing. As I said back then, it'll never be possible to "prove" the virus couldn't have come from a lab (nearly impossible to prove a "negative"), but the papers/arguments I've read have convinced me (and more importantly, the vast majority of virology/evolutionary biology experts) that it's extraordinarily unlikely. We've already seen how wrong Martenson was on HCQ and he and these guys are just as wrong on the origin of the novel coronavirus.
He just won't let it go regarding HCQ. That said, I don't know if any of the studies that have been done included the magic bullet (zinc) that he is always talking about, so until there is such a study he'll probably keep harping on it. He also likes to tout ivermectin but I haven't seen any real good evidence that works either.
The lab thing...I think there's about a 30-40% chance it is a lab release. Working virologists are quick to dismiss that possibility but they have a vested interest in it not being a lab release. Even if this one is completely natural, eventually there's probably going to be something that gets out and wreaks similar havoc so after the pandemic is over it will be worth looking at this issue in detail.
This may have discussed been talk about on this third before but I'm not checking it everyday. There seems to be a big drop in heart attacks and strokes during the pandemic. Is this an indication that that classifications of both were inaccurate before or are deaths of these two causes being lumped in Covid #s
Came back from a drive down 206 in Hillsborough. Stopped at the light and looked to the car next to me and there was a man driving with gloves, a mask and a face shield closed at bottom and open at top. I did not see any hazardous material label on his car so I laughed and said WTF?
I just assume these people are ubers
I just assume these people are ubers
Out of town plates. Going into Shop Rite parking area.
https://news.yahoo.com/more-schools-stay-online-one-140501853.html
School opened in Indiana and the first coronavirus case on the first day
School opened in Indiana and the first coronavirus case on the first day
- Status
- Not open for further replies.
Similar threads
- Replies
- 47
- Views
- 3K
- Replies
- 472
- Views
- 20K
- Replies
- 136
- Views
- 5K
- Replies
- 90
- Views
- 3K
- Replies
- 25
- Views
- 2K
ADVERTISEMENT
Latest posts
-
-
-
 BB Recruiting 2025 Rutgers Basketball Transfer Portal Tracker
BB Recruiting 2025 Rutgers Basketball Transfer Portal Tracker- Latest: RU-Choppin-Ohio
-
ADVERTISEMENT