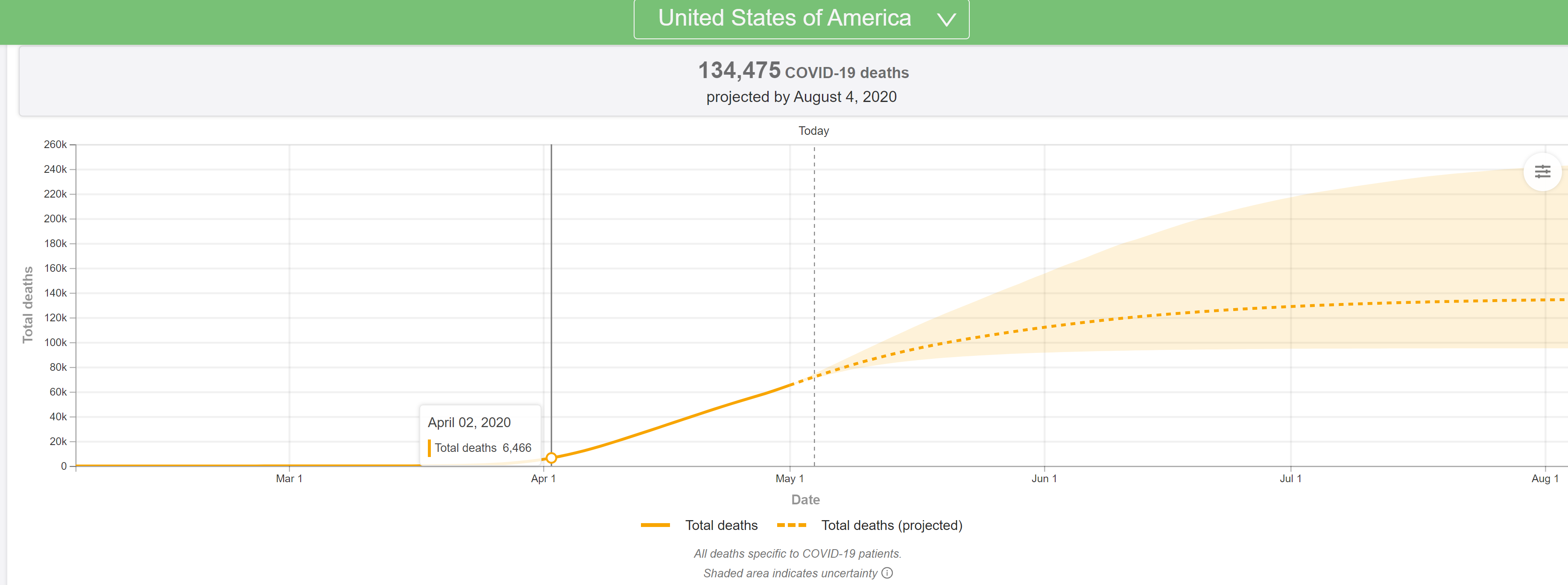
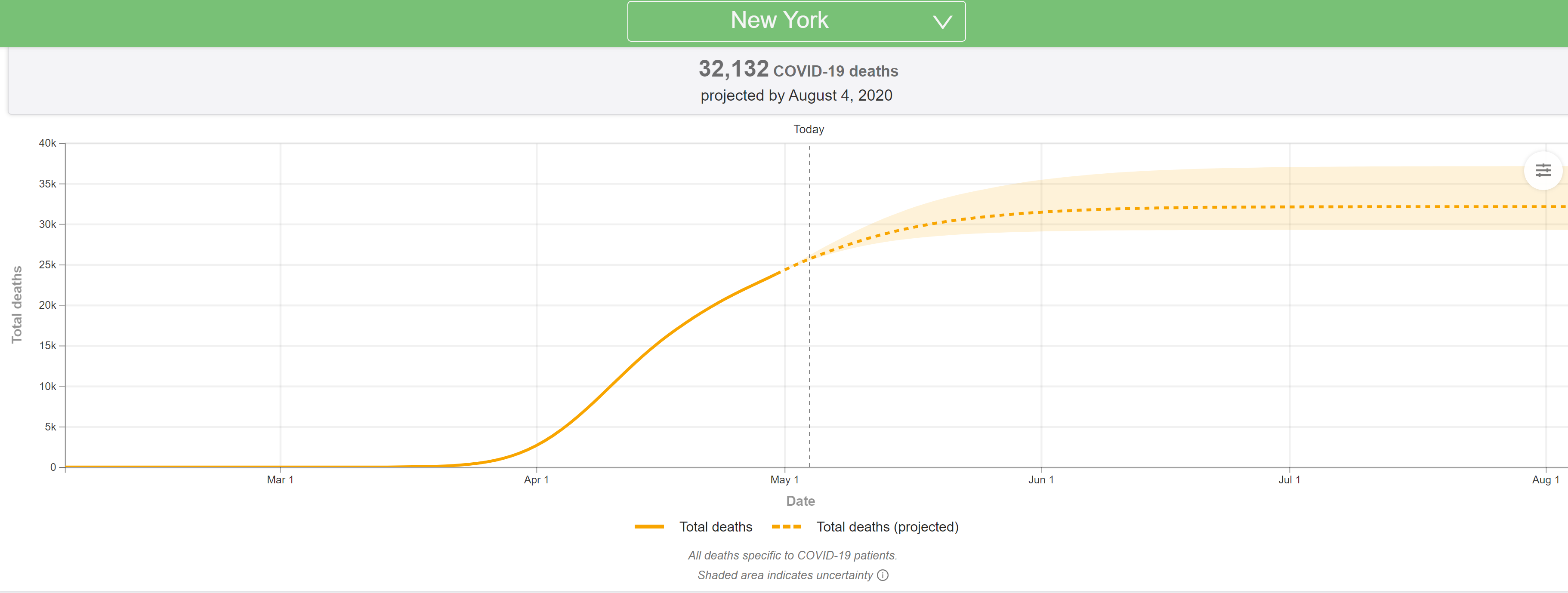
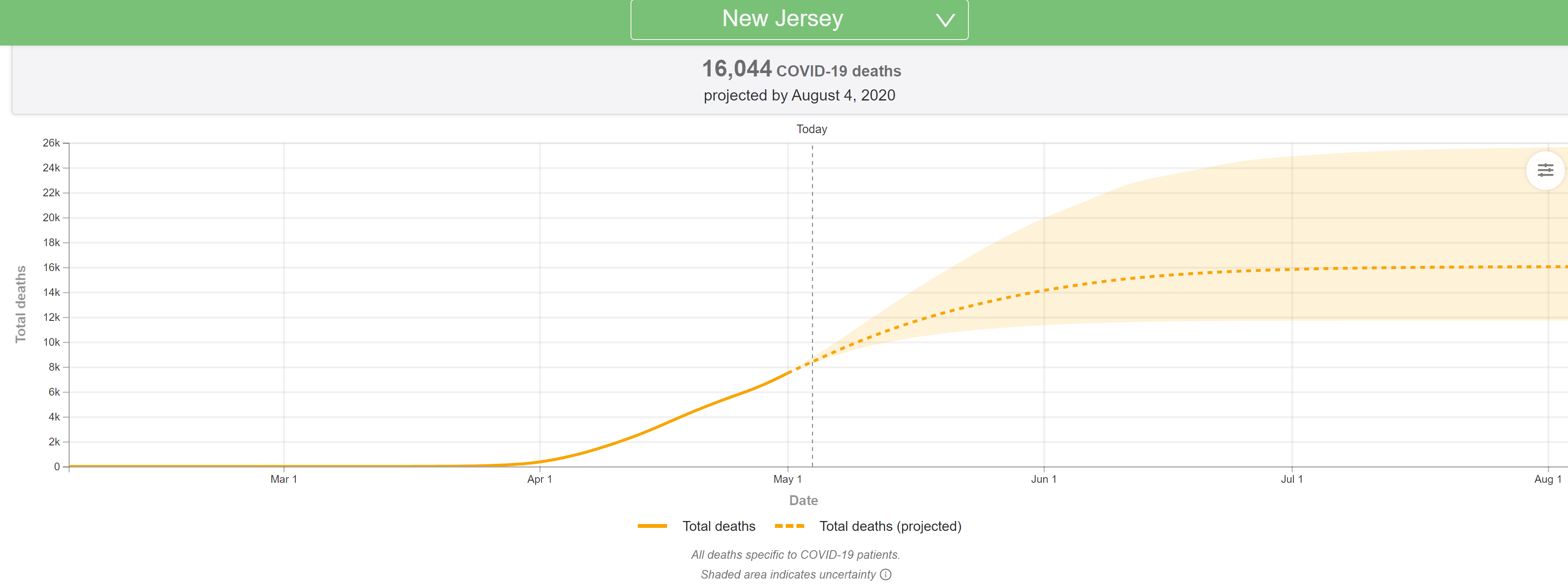
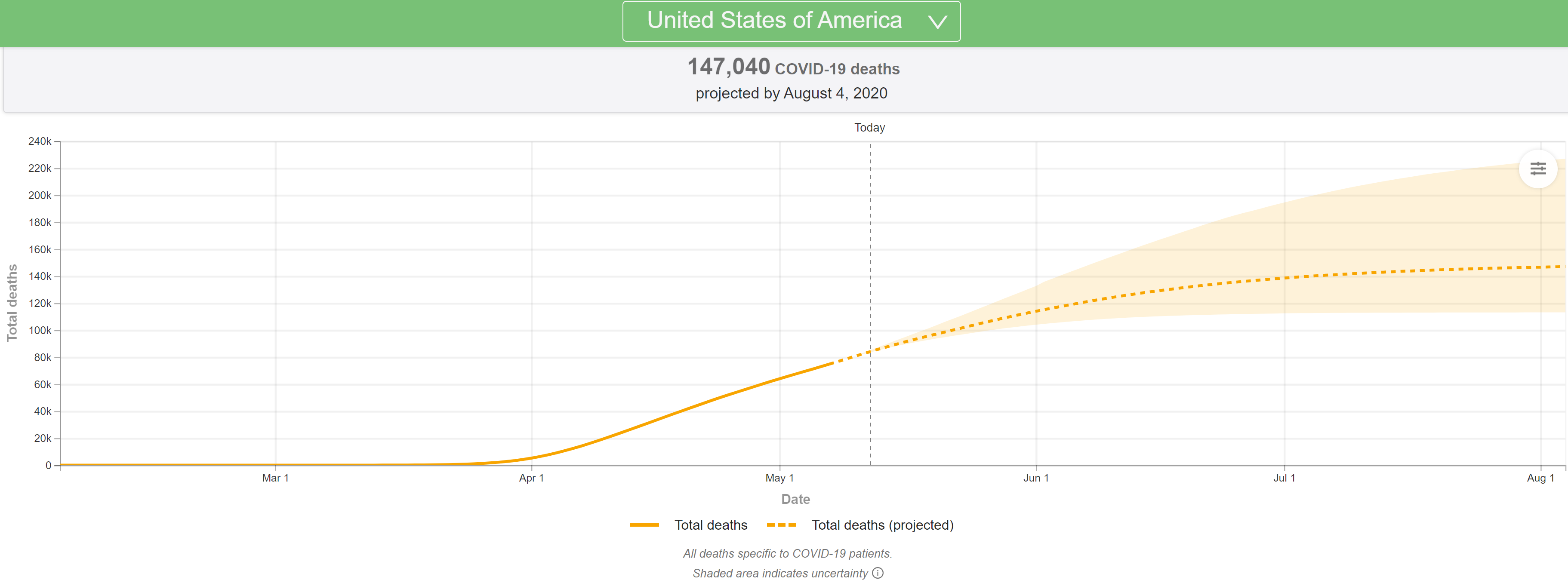
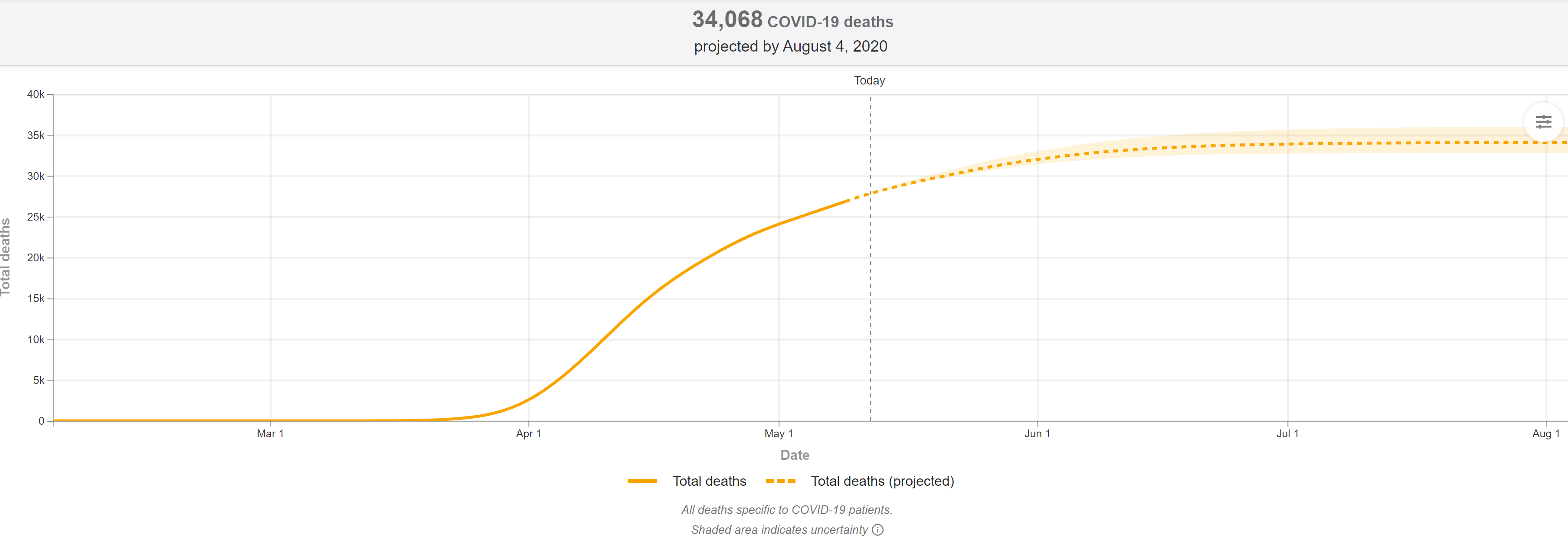
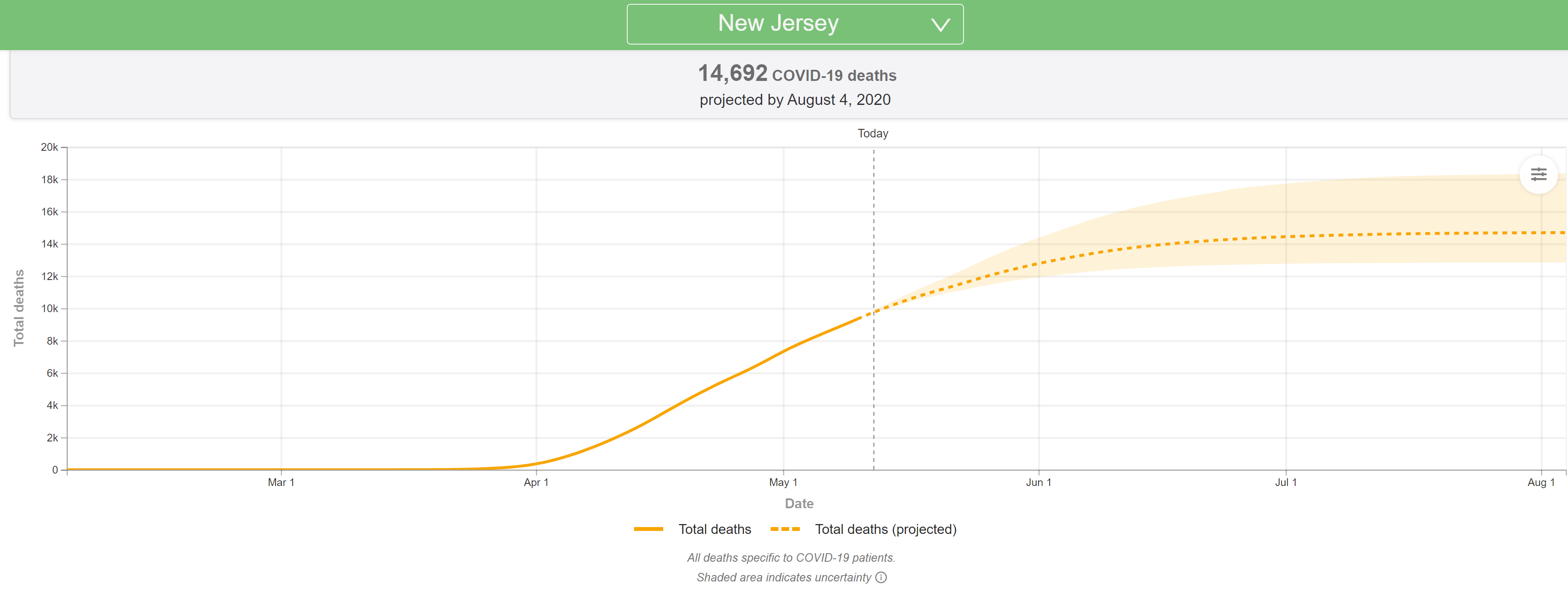
The latest (5/4) projections are out from the U of Washington/IHME and they're very bad, with the US deaths predicted to jump from the 72K in the 4/27 model to 134K through the end of July in the 5/4 model run. NY deaths are modeled to increase from 24K in the 4/27 model to 32K in the 5/4 model (more distancing modeled, hence the smaller increase vs. the US) and NJ deaths are modeled to increase from 7,2K in the 4/27 mode to 16K in the 5/4 model (not clear why NJ wasn't treated like NY).
They've completely overhauled the model and are now factoring in an increase in deaths due to expected significant increases in transmissions related to significant relaxation of stay at home policies and social distancing efforts, as well as slower than expected declines in deaths everywhere, once peaks are reached and passed. Haven't had time to go through it all, as there's a ton of new info, but did include the updated US/NY/NJ graphics. Will update this post with more later...
In addition, the Times obtained an internal CDC report from internal modeling, which is also predicting roughly a doubling of deaths from the current 68K (that would be 136K) by mid-summer, but the Administration is pushing back on that saying the report hasn't been fully vetted yet. However, President Trump on Sunday said deaths could reach 100K, so it certainly seems like forecasts are getting worse, even if not final yet. In that CDC report, it shows deaths per day increasing from the current ~2000/day to over 3000 per day by June.
https://covid19.healthdata.org/united-states-of-america
https://www.nytimes.com/2020/05/04/us/coronavirus-live-updates.html#link-32993cff
https://int.nyt.com/data/documenthe...f7319f4a55fd0ce5dc9/optimized/full.pdf#page=1
As I have been saying for the past week or so and which the Wharton model clearly confirmed on Friday, if restrictive policies are relaxed and social distancing lessened significantly, as looks to be happening, without an infrastructure to test massively and rapidly to detect outbreaks and to trace contacts and isolate positives and contacts, like South Korea and Taiwan have done (which we don't appear to be ready/willing to implement), deaths will get far worse than most have been projecting (including me). If one assumes a 60% infection endpoint (near herd immunity) and a very conservative 0.2% infection fatality rate (NY is at 0.7% now), then about ~400K US deaths would occur in the next 6-12 months if we open it all back up, but if we use an IFR of 0.5% (plausible), the estimate would be 1000K US deaths, which is pretty damn close to Wharton's 950K estimate in their model with limited controls/distancing.
https://rutgers.forums.rivals.com/t...social-distancing.191275/page-94#post-4539724
The only other hope we have to not hit the modeled numbers of deaths in the next 2 months is if we have a bona fide cure (or close to it) in place in the next month or so. We all better hope convalescent plasma is as good as the anecdotal reports are indicating, since that can help now, whereas even the engineered antibodies, which could be available by late summer, will be too late to prevent many of these deaths, and a vaccine is at least several more months beyond late summer.