
So you believe NJ numbers but no others. Gotcha. Still believe Trump won? Just trying to figure how crazy you really are.YEAAAAAAAAAA . You believe the numbers and what public servants say ? And how many have died because of murphy ? It is his state and HIS plans in long tear care facilities . How about HIS plan in vet homes ? Have a swell night .
Colleges
- American Athletic
- Atlantic Coast
- Big 12
- Big East
- Big Ten
- Colonial
- Conference USA
- Independents (FBS)
- Junior College
- Mountain West
- Northeast
- Pac-12
- Patriot League
- Pioneer League
- Southeastern
- Sun Belt
- Army
- Charlotte
- East Carolina
- Florida Atlantic
- Memphis
- Navy
- North Texas
- Rice
- South Florida
- Temple
- Tulane
- Tulsa
- UAB
- UTSA
- Boston College
- California
- Clemson
- Duke
- Florida State
- Georgia Tech
- Louisville
- Miami (FL)
- North Carolina
- North Carolina State
- Pittsburgh
- Southern Methodist
- Stanford
- Syracuse
- Virginia
- Virginia Tech
- Wake Forest
- Arizona
- Arizona State
- Baylor
- Brigham Young
- Cincinnati
- Colorado
- Houston
- Iowa State
- Kansas
- Kansas State
- Oklahoma State
- TCU
- Texas Tech
- UCF
- Utah
- West Virginia
- Illinois
- Indiana
- Iowa
- Maryland
- Michigan
- Michigan State
- Minnesota
- Nebraska
- Northwestern
- Ohio State
- Oregon
- Penn State
- Purdue
- Rutgers
- UCLA
- USC
- Washington
- Wisconsin
High Schools
- Illinois HS Sports
- Indiana HS Sports
- Iowa HS Sports
- Kansas HS Sports
- Michigan HS Sports
- Minnesota HS Sports
- Missouri HS Sports
- Nebraska HS Sports
- Oklahoma HS Sports
- Texas HS Hoops
- Texas HS Sports
- Wisconsin HS Sports
- Cincinnati HS Sports
- Delaware
- Maryland HS Sports
- New Jersey HS Hoops
- New Jersey HS Sports
- NYC HS Hoops
- Ohio HS Sports
- Pennsylvania HS Sports
- Virginia HS Sports
- West Virginia HS Sports
ADVERTISEMENT
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
OT: COVID Science - Pfizer/Moderna vaccines >90% effective; Regeneron antibody cocktail looks very promising in phase II/III trial and more
- Thread starter RU848789
- Start date
- Status
- Not open for further replies.

An Emergency Use Authorization was granted for the Regeneron antibody cocktail by the FDA yesterday, as expected (and slightly surprised it was granted later than Lilly's EUA for their antibody treatment which does not look as effective). Both the Lilly and Regeneron monoclonal antibody treatments are for mild/moderately ill COVID patients prior to hospitalization, where they've had good clinical trial results, so far (especially the Regeneron one).
https://www.cnn.com/2020/11/21/health/regeneron-fda-clearance-trump-coronavirus/index.html
"Regeneron now expects to have REGEN-COV2 treatment doses ready for approximately 80,000 patients by the end of November, approximately 200,000 patients by the first week of January, and approximately 300,000 patients in total by the end of January 2021," the company said in their news release yesterday.
This is a start, but only a start, given that we're almost seeing 200,000 cases per day now - these monoclonal antibody drugs will be reserved for elderly patients and those with high risk factors (like Trump and Christie, who both received the Regeneron treatment). Unfortunately, the Regeneron cocktail clinical trial was put on hold for patients on ventilators and those receiving supplemental oxygen - many (including me) had hoped it would work as well in seriously ill patients.
https://investor.regeneron.com/news...cov2-first-antibody-cocktail-covid-19-receive
More good news on monoclonal antibodies from Eli Lilly's single mAb, bamlanivimab (which will likely apply to the Regeneron mixture of two antibodies, which have generally had better clinical results so far), which was shown to significantly reduce infection with COVID by ~80% in LTC residents and staff vs. those who did not recieve a prophylactic mAb treatment.
Haven't seen prevention data from the general public yet but no reason to think these people are unique. The problem with the mAbs is that they're expensive and there are nowhere near enough doses for more than a small fraction of the public (maybe a few million doses by end of 1Q21 vs. tens of millions of vaccine doses and the vaccines are better). But right now, with the vaccine rollout being slow, there's no reason to not use these mAbs up as fast as possible, especially in vulnerable LTC/elderly populations.
https://investor.lilly.com/news-rel...zing-antibody-bamlanivimab-ly-cov555-prevente
The 965 participants who tested negative for the SARS-CoV-2 virus at baseline (299 residents and 666 staff) were included in the analysis of primary and key secondary endpoints for assessing prevention, while the 132 participants (41 residents and 91 staff) who tested positive for the virus at baseline were included in exploratory analyses for assessing treatment, adding to the growing body of evidence for treatment with bamlanivimab. All participants were randomized to receive either 4,200 mg of bamlanivimab or placebo.
After all participants reached 8 weeks of follow-up, there was a significantly lower frequency of symptomatic COVID-19 (the primary endpoint) in the bamlanivimab treatment arm versus placebo (odds ratio 0.43, p=0.00021). Results for all key secondary endpoints also reached statistical significance in both the overall and resident populations.
For the pre-specified subgroup of nursing home residents, there was also a significantly lower frequency of symptomatic COVID-19 in those treated with bamlanivimab versus placebo in this important population (odds ratio 0.20; p=0.00026). These results suggest that residents randomized to bamlanivimab have up to an 80 percent lower risk of contracting COVID-19 versus residents in the same facility randomized to placebo.
Are you calling this medical journal not sciencePosts like these and others from questionable twitter feeds are why you have low credibility on the topic of COVID. Did you even read the paper? It is not, in any way, a "recommendation" of use of HCQ. This is about potential off-label use of HCQ for mildly ill COVID patients, since HCQ is not approved for use for COVID (bold part in the excerpt below from the paper), given its general failure to show any efficacy in post-exposure prophylaxis and in both mildly ill and hospitalized COVID patients in randomized, controlled clinical trials, none of which the article even acknowledges.
Combination Antiviral Therapy
Rapid and amplified viral replication is the hallmark of most acute viral infections. By reducing the rate, quantity, or duration of viral replication, the degree of direct viral injury to the respiratory epithelium, vasculature, and organs may be lessened.16 Additionally, secondary processes that depend on viral stimulation, including the activation of inflammatory cells, cytokines, and coagulation, could potentially be lessened if viral replication is attenuated. Because no form of readily available medication has been designed specifically to inhibit SARS-CoV-2 replication, 2 or more of the nonspecific agents listed here can be entertained. None of the approaches listed have specific regulatory approved advertising labels for their manufacturers; thus all would be appropriately considered acceptable “off-label” use.
In case anyone is interested, below is the link to a WaPo article summarizing the two RCTs on mildly ill outpatients being treated with HCQ mentioned above. I posted these awhile back, but basically, the studies by Boulware (MN) and Mitja (Spain) show fairly conclusively that HCQ has no efficacy in mildly ill COVID patients. This is bad science and Elsevier should know better than to publish this, especially since the article didn't even mention these two definitive studies.
https://www.washingtonpost.com/heal...-not-effective-early-treatment-mild-covid-19/
You are full of it
Is the chart fake..its not random twitter..its in the freaking journel
Follow the science bro
All science matters
I also see you conveniently ignoring the pcr news
Will you please take your silly nonsense to the CE board.YEAAAAAAAAAA . You believe the numbers and what public servants say ? And how many have died because of murphy ? It is his state and HIS plans in long tear care facilities . How about HIS plan in vet homes ? Have a swell night .
Now they just need to use the drugs in some systematic fashion.More good news on monoclonal antibodies from Eli Lilly's single mAb, bamlanivimab (which will likely apply to the Regeneron mixture of two antibodies, which have generally had better clinical results so far), which was shown to significantly reduce infection with COVID by ~80% in LTC residents and staff vs. those who did not recieve a prophylactic mAb treatment.
Haven't seen prevention data from the general public yet but no reason to think these people are unique. The problem with the mAbs is that they're expensive and there are nowhere near enough doses for more than a small fraction of the public (maybe a few million doses by end of 1Q21 vs. tens of millions of vaccine doses and the vaccines are better). But right now, with the vaccine rollout being slow, there's no reason to not use these mAbs up as fast as possible, especially in vulnerable LTC/elderly populations.
https://investor.lilly.com/news-rel...zing-antibody-bamlanivimab-ly-cov555-prevente
The 965 participants who tested negative for the SARS-CoV-2 virus at baseline (299 residents and 666 staff) were included in the analysis of primary and key secondary endpoints for assessing prevention, while the 132 participants (41 residents and 91 staff) who tested positive for the virus at baseline were included in exploratory analyses for assessing treatment, adding to the growing body of evidence for treatment with bamlanivimab. All participants were randomized to receive either 4,200 mg of bamlanivimab or placebo.
After all participants reached 8 weeks of follow-up, there was a significantly lower frequency of symptomatic COVID-19 (the primary endpoint) in the bamlanivimab treatment arm versus placebo (odds ratio 0.43, p=0.00021). Results for all key secondary endpoints also reached statistical significance in both the overall and resident populations.
For the pre-specified subgroup of nursing home residents, there was also a significantly lower frequency of symptomatic COVID-19 in those treated with bamlanivimab versus placebo in this important population (odds ratio 0.20; p=0.00026). These results suggest that residents randomized to bamlanivimab have up to an 80 percent lower risk of contracting COVID-19 versus residents in the same facility randomized to placebo.
You have no idea what you're talking about. Yes, it's a medical journal, but it's not a high quality one and their peer review sucks if they let this be published. I've published about a dozen peer-reviewed articles in the scientific literature (not medical, but the systems are similar), so I know what I'm talking about. To publish that article without referencing/discussing the "gold standard" RCTs showing no efficacy in mildly ill COVID outpatients is an egregious error. Full stop. Now go find some even worse nonsense and post it breathlessly, as if it means something. I haven't put anyone on ignore on this site, but you're close - if it weren't for hoops, I think you'd be the first. If I could do it by thread that would be nice.Are you calling this medical journal not science
You are full of it
Is the chart fake..its not random twitter..its in the freaking journel
Yes I believe I suggested this along with a few others here. It is the only possible solution other than more vaccine availability. Fed and State directed by the Fed. The states have enough issues.Defense Production Act, FEMA and the National Guard. Get it all going. Can we produce more vaccine more quickly? The actual vaccine?
Numbers any thoughts?
Them numbers are not real. It is sad but they are inflated.400k died from Covid under Trump. Let's see how many die under Biden, the President with an actual plan.
You guys just don’t stop do you? Enough already. Plenty of evidence of the deadliness of this virus from excess deaths and declining age expectancy to back up these numbers in this country and many others. Move your Q nonsense elsewhere please.Them numbers are not real. It is sad but they are inflated.
You have no idea what you're talking about. Yes, it's a medical journal, but it's not a high quality one and their peer review sucks if they let this be published. I've published about a dozen peer-reviewed articles in the scientific literature (not medical, but the systems are similar), so I know what I'm talking about. To publish that article without referencing/discussing the "gold standard" RCTs showing no efficacy in mildly ill COVID outpatients is an egregious error. Full stop. Now go find some even worse nonsense and post it breathlessly, as if it means something. I haven't put anyone on ignore on this site, but you're close - if it weren't for hoops, I think you'd be the first. If I could do it by thread that would be nice.
Lol because its not your science..wow this is amazing
U are actually deciding which peer reviewed medical studies are acceptable
Your arrogance is showing
Telling you threatening ignoring when you don't like the science
Defense Production Act, FEMA and the National Guard. Get it all going. Can we produce more vaccine more quickly? The actual vaccine?
Numbers any thoughts?
This is off the top of my head (I rarely do that, so take it with a grain of salt. IMO, it would be very difficult to bring on more vaccine production facilities in under 4 months, as it's really, really complicated to make sterile vaccines without compromising sterility (which is a key safety issue), so I don't think it's going to help with the current state - it could help with bringing more vaccines on line this summer, although I think simply providing more OWS funding to existing manufacturers is a better move for that.
The Act is more suited, IMO, to helping produce key "cogs" like vials, syringes, machinery/equipment for manufacturing, etc. However, FEMA and the National Guard could certainly help with logistics and distribution - in the article I linked the other day about Israel's vaccination success (nearly 30% vaccinated already), one of the key elements was the involvement of their military in logistics/distribution.
I've been right on every aspect of HCQ all along, including anticipating the medical community dismissing HCQ, since I'm able to read scientific articles and sniff out BS, especially when comparing them vs. much better studies already published. This is just one more example. Just because you don't have those skills is no reason for me not to exercise them. We're done on this topic as you clearly lack the abiility to understand even basic science if you're trying to argue this point.Lol because its not your science..wow this is amazing
U are actually deciding which peer reviewed medical studies are acceptable
Your arrogance is showing
Telling you threatening ignoring when you don't like the science

COVID-19 early treatment: real-time analysis of 5,015 studies
COVID-19 early treatment: real-time analysis of 5,015 studies for 104 treatments
 c19study.com
c19study.com
I am not say it isnt deadly by any means. I worked in hospitals in the beginning as saw how jammed they were. I know it is real. However even on the CDC website it has over 12,000 deaths from Intentional and unintentional injury, poisoning and other adverse events that is counted as a Covid death. Has nothing to do with the letter QYou guys just don’t stop do you? Enough already. Plenty of evidence of the deadliness of this virus from excess deaths and declining age expectancy to back up these numbers in this country and many others. Move your Q nonsense elsewhere please.
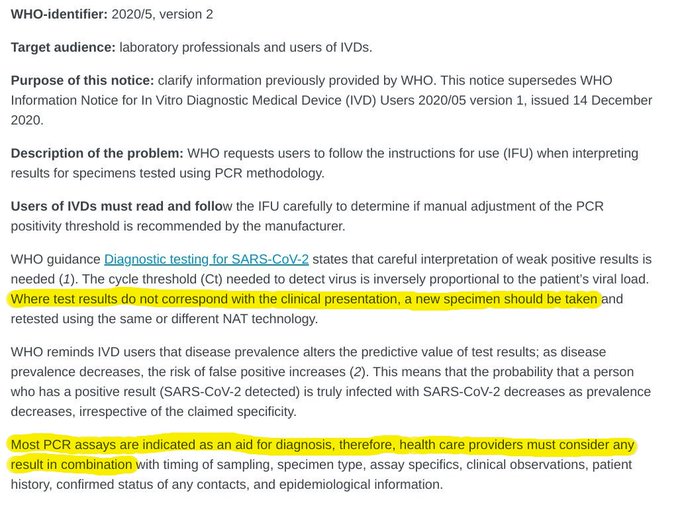
and now the WHO comes out and questions the PCR testing, some of us were onto this before but it was shouted down..ie NY Times article.
means that if you are showing no symptoms and test positive with PCR testing, ANOTHER test should be run to confirm
wow
the timing of the announcement makes my head spin but I wont go there
yup and crickets from the usual suspects who downplayed the nytimes article that was posted months ago.
This woman is a liberal and she is stunned at the admission of WHO on pcr..shes been saying it for months
Not much "new" here. This was discussed months ago, as per the first 2 links below and nobody I saw "shouted" anyone down. I'm actually surprised it took them this long to reduce the number of amplification cycles in the PCR viral test for COVID. I've been arguing for months, as per Dr. Mina's positions on this, that we're misusing the PCR test and should be using less sensitive antigen-style screening tests, but doing them very frequently (like the B1G is doing), but this would've required a large investment that the Trump Administration was unwilling to make (they bungled testing at every step of the way), in order to make such tests widely available for everyone (and even at-home). Maybe we can get this kind of massive, frequent testing going now.
The PCR test is better suited as a confirmatory test or as a test for people with clear COVID symptoms just to be sure (since the antigen tests aren't as good). Or, as I said in August, using the PCR test with 35-40 cycles is ok, as long as we have no other tests and as long as we're telling people how many cycles are being used, so they can know the risk. I also don't have much issue with false positives, as those merely tell people they should be isolating and there isn't a huge downside of isolating for most - but for essential workers, that's where the daily antigen test would be better, as that is sensitive enough to alert the person to when they're already or just becoming contagious (even if asymptomatic), which is what is really important, plus it's fast/frequent enough that one can do it every day to "exonerate" false positives (while the PCR test is much more complex/expensive and takes too much time).
https://rutgers.forums.rivals.com/t...es-interventions-and-more.198855/post-4680980
https://rutgers.forums.rivals.com/t...es-interventions-and-more.198855/post-4683701
You guys just don’t stop do you? Enough already. Plenty of evidence of the deadliness of this virus from excess deaths and declining age expectancy to back up these numbers in this country and many others. Move your Q nonsense elsewhere please.
Can you take your accusations of Q elsewhere..its childish
Not much "new" here. This was discussed months ago, as per the first 2 links below and nobody I saw "shouted" anyone down. I'm actually surprised it took them this long to reduce the number of amplification cycles in the PCR viral test for COVID. I've been arguing for months, as per Dr. Mina's positions on this, that we're misusing the PCR test and should be using less sensitive antigen-style screening tests, but doing them very frequently (like the B1G is doing), but this would've required a large investment that the Trump Administration was unwilling to make (they bungled testing at every step of the way), in order to make such tests widely available for everyone (and even at-home). Maybe we can get this kind of massive, frequent testing going now.
The PCR test is better suited as a confirmatory test or as a test for people with clear COVID symptoms just to be sure (since the antigen tests aren't as good). Or, as I said in August, using the PCR test with 35-40 cycles is ok, as long as we have no other tests and as long as we're telling people how many cycles are being used, so they can know the risk. I also don't have much issue with false positives, as those merely tell people they should be isolating and there isn't a huge downside of isolating for most - but for essential workers, that's where the daily antigen test would be better, as that is sensitive enough to alert the person to when they're already or just becoming contagious (even if asymptomatic), which is what is really important, plus it's fast/frequent enough that one can do it every day to "exonerate" false positives (while the PCR test is much more complex/expensive and takes too much time).
https://rutgers.forums.rivals.com/t...es-interventions-and-more.198855/post-4680980
https://rutgers.forums.rivals.com/t...es-interventions-and-more.198855/post-4683701
Sorry there is downside to isolating..are you even serious with that
Its unnecessary if you arent positive..stop acting like its normal to stay inside
More good news on monoclonal antibodies from Eli Lilly's single mAb, bamlanivimab (which will likely apply to the Regeneron mixture of two antibodies, which have generally had better clinical results so far), which was shown to significantly reduce infection with COVID by ~80% in LTC residents and staff vs. those who did not recieve a prophylactic mAb treatment.
Haven't seen prevention data from the general public yet but no reason to think these people are unique. The problem with the mAbs is that they're expensive and there are nowhere near enough doses for more than a small fraction of the public (maybe a few million doses by end of 1Q21 vs. tens of millions of vaccine doses and the vaccines are better). But right now, with the vaccine rollout being slow, there's no reason to not use these mAbs up as fast as possible, especially in vulnerable LTC/elderly populations.
https://investor.lilly.com/news-rel...zing-antibody-bamlanivimab-ly-cov555-prevente
The 965 participants who tested negative for the SARS-CoV-2 virus at baseline (299 residents and 666 staff) were included in the analysis of primary and key secondary endpoints for assessing prevention, while the 132 participants (41 residents and 91 staff) who tested positive for the virus at baseline were included in exploratory analyses for assessing treatment, adding to the growing body of evidence for treatment with bamlanivimab. All participants were randomized to receive either 4,200 mg of bamlanivimab or placebo.
After all participants reached 8 weeks of follow-up, there was a significantly lower frequency of symptomatic COVID-19 (the primary endpoint) in the bamlanivimab treatment arm versus placebo (odds ratio 0.43, p=0.00021). Results for all key secondary endpoints also reached statistical significance in both the overall and resident populations.
For the pre-specified subgroup of nursing home residents, there was also a significantly lower frequency of symptomatic COVID-19 in those treated with bamlanivimab versus placebo in this important population (odds ratio 0.20; p=0.00026). These results suggest that residents randomized to bamlanivimab have up to an 80 percent lower risk of contracting COVID-19 versus residents in the same facility randomized to placebo.
Finally some data on the prophylactic use of mABs. Can’t believe it took this long. This is a much better use case than using in a hospital setting.
I hope Biden pours money into early treatments. It’s pathetic it’s been a year and we are nowhere with it. No inhaler treatments, no antiviral pills. So many trials for hospital settings, which we’ve all know for a long time is too late for most treatments.
Ugh, prob won’t see J&J data until sometime in the first half of Feb.
Bloomberg - Are you a robot?
www.bloomberg.com
Article said we'd have trial data by the last week in Jan or the first week in Feb, which I don't think is a change - that's when we'll see press releases. Just like for Pfizer/Moderna, it'll take a few weeks to a month to get an EUA.Ugh, prob won’t see J&J data until sometime in the first half of Feb.
Bloomberg - Are you a robot?
www.bloomberg.com
You're simply wrong on this and, in fact, the numbers are likely 10-20% higher, given excess death data, to date, as many have discussed previously in this thread.Them numbers are not real. It is sad but they are inflated.
I said there isn't a huge downside for most. Most people I know are working remotely, which is maybe inefficient for some, but not particularly hard. Sure, false positives are an issue for people who are on the front lines working and will lose time because of that. But like I said, I'd rather have a less sensitive, cheaper, more frequent antigen test for all so false positives become much less of an issue, but we aren't there yet. Also, isolating doesn't mean one is chained indoors, but it does usually mean not going to work with people, which I agree is an issue.Sorry there is downside to isolating..are you even serious with that
Its unnecessary if you arent positive..stop acting like its normal to stay inside
I said there isn't a huge downside for most. Most people I know are working remotely, which is maybe inefficient for some, but not particularly hard. Sure, false positives are an issue for people who are on the front lines working and will lose time because of that. But like I said, I'd rather have a less sensitive, cheaper, more frequent antigen test for all so false positives become much less of an issue, but we aren't there yet. Also, isolating doesn't mean one is chained indoors, but it does usually mean not going to work with people, which I agree is an issue.
I think you are assuming everyone is an office worker who can work from home. What about the people who really work for a living? They don’t have that luxury.
I know you’ve posted about this before but based on the preliminary data, any guesses on the efficacy of the J&J vaccine? Not sure if the 90-100% in the paper is the same as efficacy.Article said we'd have trial data by the last week in Jan or the first week in Feb, which I don't think is a change - that's when we'll see press releases. Just like for Pfizer/Moderna, it'll take a few weeks to a month to get an EUA.
Lol because its not your science..wow this is amazing
U are actually deciding which peer reviewed medical studies are acceptable
Your arrogance is showing
Telling you threatening ignoring when you don't like the science
Your idiocy is showing. You've been laughed out of this thread a dozen+ times already. Take the hint.
It’s hard to trust non-scientists to interpret scientific data from a journal article. It’s even harder when they spell journal wrong.Are you calling this medical journal not science
You are full of it
Is the chart fake..its not random twitter..its in the freaking journel
Follow the science bro
All science matters
I also see you conveniently ignoring the pcr news
I think you are wrong on this. How do you explain a decline in all other illnesses related to deaths. What about the 12000+ on the CDC that died from Intentional and unintentional injury, poisoning and other adverse events that is counted as a Covid death. Again Im not saying the virus is not real just feel that the deaths and positives are exaggerated.You're simply wrong on this and, in fact, the numbers are likely 10-20% higher, given excess death data, to date, as many have discussed previously in this thread.
I think you are assuming everyone is an office worker who can work from home. What about the people who really work for a living? They don’t have that luxury.
which is the majority of people and those people are not well off elitists either
Why would they publish data on projects they want to keep secret?Thanks, mostly. I would at least challenge you on one thing: I've been highly critical of China hiding the risks from this virus and the extent of the epidemic in Wuhan over the first few months of the outbreak. Since then, I don't think I've consciously been promoting viewpoints that come from the CCP, but will acknowledge it's possible I've simply missed such connections. Most of the virologist papers I've cited weren't from scientists associated with the CCP (Daszak hasn't been one of my sources). I also think quite a few basic virus/medical/clinical papers out of China have been quite good - at least the ones that get through peer review - probably because they have no conection to what the government did or did not do during the early months.
Also, bac may find this suprising, but I thought the CNET article was pretty well done. What I liked about it was it completely dismissed the possibility of SARS-CoV-2 being "engineered/created" in a lab, which is something I've been sharing for months. And its presentation of the potential lab release, which I still think is far less likely than natural evolution, was at least done from the perspective of: "here's something that could have happened as an accident," not "look, here's the aboslute truth we know from xyz shady source proving a lab leak is the source" and it also reiterates that natural evolution and a jump somewhere to humans is still the most likely explanation. The biggest reason why the "lab leak" theory is unlikely, as per my post below from months ago, is that the WIV lab never published any coronavirus sequences being worked on that were anywhere close to SARS-CoV-2 and they were fairly prolific producers of papers. Doesn't "prove" it wasn't accidentally released from there, but makes it far less likely.
https://rutgers.forums.rivals.com/t...es-interventions-and-more.191275/post-4558420
I think you are wrong on this. How do you explain a decline in all other illnesses related to deaths. What about the 12000+ on the CDC that died from Intentional and unintentional injury, poisoning and other adverse events that is counted as a Covid death. Again Im not saying the virus is not real just feel that the deaths and positives are exaggerated.
but the other day they just accepted a bunch old people dying in Norway after receiving the vaccine of dying because well they were old and old people die
I think you are wrong on this. How do you explain a decline in all other illnesses related to deaths. What about the 12000+ on the CDC that died from Intentional and unintentional injury, poisoning and other adverse events that is counted as a Covid death. Again Im not saying the virus is not real just feel that the deaths and positives are exaggerated.
Why were there so many more deaths year over year then? Was every COD up?
but the other day they just accepted a bunch old people dying in Norway after receiving the vaccine of dying because well they were old and old people die
Lie.
It’s hard to trust non-scientists to interpret scientific data from a journal article. It’s even harder when they spell journal wrong.
no he trashed it and says he knows better than medical professionals, its stunning to see his ego on display as he dismisses SCIENCE
Lie.
no thats what was said and yes they found no correlation but maybe it was just enough in their system to push them over the edge...kind of like Covid
no thats what was said and yes they found no correlation but maybe it was just enough in their system to push them over the edge...kind of like Covid
Sounds like maybe you think you know better than the medical professionals now ; \
I think I did, but briefly, there is zero known efficacy yet for J&J, as we simply don't have the data from the phase III trials comparing placebo to the vaccine. The paper on the earlier clinical trials discussed the very strong immune responses seen in vaccinated patients, but that won't necessarily translate to >90% efficacy (it could). Given that the J&J vaccine is an adenovirus vector vaccine, like the Astra-Zeneca one, I would think it would be closer to the AZ efficacy (which was murky given the issues in their trials), like maybe 70-80%, but OWS's Slaoui said he thought 80-85% efficacy is likely, but again, nobody knows.I know you’ve posted about this before but based on the preliminary data, any guesses on the efficacy of the J&J vaccine? Not sure if the 90-100% in the paper is the same as efficacy.
If it's 80% and a single shot and stable in the fridge, that's a lot of plusses, even though that's slightly less effective than the two mRNA vaccines - I think the key may then be how many of those who get the virus, still, have serious cases - if that's essentially zero, like the mRNA vaccines, I'd say that puts J&J in the lead; if not, it'll still get used but maybe not as much.
https://www.bloomberg.com/news/arti...decision-on-vaccine-clearance-coming-by-march
I trashed it because yeah, I do know better in this case and so does the medical community, which will trash it once they see it, since they know that the Boulware/Mitja RCTs on mildly ill patients are far more relevant than this crappy "recommendation" (it's not even a study) and they'll laugh their asses off when they see the "paper" didn't even mention these RCTs.no he trashed it and says he knows better than medical professionals, its stunning to see his ego on display as he dismisses SCIENCE
Sounds like maybe you think you know better than the medical professionals now ; \
No i dont..i actually believe in reading many sources
I trashed it because yeah, I do know better in this case and so does the medical community, which will trash it once they see it, since they know that the Boulware/Mitja RCTs on mildly ill patients are far more relevant than this crappy "recommendation" (it's not even a study) and they'll laugh their asses off when they see the "paper" didn't even mention these RCTs.
Laughing it off sounds so full of science
- Status
- Not open for further replies.
Similar threads
ADVERTISEMENT
ADVERTISEMENT