
another fake news post from the flu bro. Can you ever tell the truth?FL confirmed cases are trending down, deaths are trending down, and % of positive tests are going down.
https://experience.arcgis.com/experience/96dd742462124fa0b38ddedb9b25e429
Colleges
- American Athletic
- Atlantic Coast
- Big 12
- Big East
- Big Ten
- Colonial
- Conference USA
- Independents (FBS)
- Junior College
- Mountain West
- Northeast
- Pac-12
- Patriot League
- Pioneer League
- Southeastern
- Sun Belt
- Army
- Charlotte
- East Carolina
- Florida Atlantic
- Memphis
- Navy
- North Texas
- Rice
- South Florida
- Temple
- Tulane
- Tulsa
- UAB
- UTSA
- Boston College
- California
- Clemson
- Duke
- Florida State
- Georgia Tech
- Louisville
- Miami (FL)
- North Carolina
- North Carolina State
- Pittsburgh
- Southern Methodist
- Stanford
- Syracuse
- Virginia
- Virginia Tech
- Wake Forest
- Arizona
- Arizona State
- Baylor
- Brigham Young
- Cincinnati
- Colorado
- Houston
- Iowa State
- Kansas
- Kansas State
- Oklahoma State
- TCU
- Texas Tech
- UCF
- Utah
- West Virginia
- Illinois
- Indiana
- Iowa
- Maryland
- Michigan
- Michigan State
- Minnesota
- Nebraska
- Northwestern
- Ohio State
- Oregon
- Penn State
- Purdue
- Rutgers
- UCLA
- USC
- Washington
- Wisconsin
High Schools
- Illinois HS Sports
- Indiana HS Sports
- Iowa HS Sports
- Kansas HS Sports
- Michigan HS Sports
- Minnesota HS Sports
- Missouri HS Sports
- Nebraska HS Sports
- Oklahoma HS Sports
- Texas HS Hoops
- Texas HS Sports
- Wisconsin HS Sports
- Cincinnati HS Sports
- Delaware
- Maryland HS Sports
- New Jersey HS Hoops
- New Jersey HS Sports
- NYC HS Hoops
- Ohio HS Sports
- Pennsylvania HS Sports
- Virginia HS Sports
- West Virginia HS Sports
ADVERTISEMENT
COVID-19 Pandemic: Transmissions, Deaths, Treatments, Vaccines, Interventions and More...
- Thread starter RU848789
- Start date
- Status
- Not open for further replies.

he can never tell the truth occasionally he stumbles into it.Cases are rising and deaths are rising..and that's based on your link above with 5/11 as the latest data reported. Check in a week or two. That will give a better idea how its trending and about the time I would expect to see a jump... if it happens.
it's lazy to say corona is like the flu, flu bro. It is also lazy to say 15 cases soon to be zero, and I'm not a shipping clerk.Most counties should be able to open more quickly. One size fits all is lazy leadership.
Did you watch the video? From your response it does not seem like it. I have read the explanations the "experts" have given and they are laughable. Watch the video, preferably with an open mind. The same US scientist (Baric) who collabs with Wuhan Lab is also the author of No See'm technology and has published Coronavirus GOF research through chimeric virus creation. In fact his work 2014 is what caused GOF research to be stopped here in the US. Again, watch the video.
FYI, I came to the same conclusion as CM weeks before he did. I posted a thread on the CE board a month ago laying several of the pieces out. Wuhan Lab is the most elegant and also most likely explanation. The whole Wuhan Lab blackout from Oct 7-24 seems to fit this puzzle nicely.
So, in addition to the New England Journal of Medicine and Journal of the American Medical Association (and the people who recently published HCQ papers in those prestigious journals), you're now adding many of the most renowned evolutionary virologists to your list of people whose explanations you find laughable. That's quite a list.
I watched the video and he simply pieces together parts of what is known about viruses and then tries to convince people that somehow people in a lab, who had zero knowledge of what SARS-CoV-2 was (since the outbreak hadn't started yet), knew to take pieces from other viruses most closely related to CV2 and link them together into a new chimeric virus that became "almost CV2" and then evolved that chimeric virus into CV2 somehow. How the hell could they know to shoot for that endpoint out of the nearly infinite number of amino acid sequences that are possible for both the RNA and protein parts of the virus? That's simply not credible.
As per today's excellent article published by CIDRAP, another top-notch infectious disease research group out of the U of MN (led by world expert Michael Osterholm), the idea that someone was able to "create" CV2 is preposterous. Sure, if they were given the blueprints to CV2, someone could likely make it, but how would anyone know to make it out of so many possibilities? And as per the comment below, if someone were trying to create a bioweapon in a lab, why wouldn't they start from SARS or MERS, which were very close to being pandemic-worthy (and far deadlier than CV2)? And even if they somehow "made" CV2 in the lab, why would they have released it in their own country?
Furthermore, he questions why anyone would go through the work of creating a new virus when they could simply take an existing virulent pathogen like the SARS (severe acute respiratory syndrome) or MERS (Middle East respiratory syndrome) coronaviruses and make them even worse, as all bioweapons programs so far have done.
"It doesn't make any sense to make a new virus that you don't know can cause disease in humans and try to create a bioweapon out of it," Andersen said. "That would be a really bad bioweapons person."
And with regard to the other possibility people talk about, i.e., that they had somehow obtained CV2 from the wild and were working with it and accidentally released it, there's also no evidence for that. Dr. Shi Zhengli (the "batwoman") published all kinds of genetic sequences from various bat coronaviruses she and her research group have found and they published nothing that close to CV2 - if they had, perhaps lab release could be an issue.
Even Kristian Anderson (an expert virologist and lead author on the Nature paper), who originally thought it possible that the virus could have been accidentally released from a lab, said that while "he can't completely rule out the possibility that the virus came from a lab, the odds of that happening are very small. He says the new coronavirus clearly originated in nature, no question about it by now."
Lastly, Martenson's use of Occam's Razor is what's laughable. What's more likely: that CV2 came into being in the same way every other virus in the history of the planet did, i.e., by evolution in some species, like bats, and probable zoonotic transfer to humans either directly or through an intermediate host, or that some researchers in a lab, not knowing the endpoint blueprint for CV2 somehow figured out a way to construct CV2? Hint: it's not the latter.
Also, there's no proof of a blackout at the lab in October, either and Dr. Shi Zhengli is not missing. The Chinese have acted very badly with regard to lying and covering up the true extent of the outbreak, but they almost certainly didn't create the virus in a lab.
Shi Zhengli, PhD, director of the Center for Emerging Infectious Diseases at the Wuhan Institute of Virology, a biosafety level 4 (BSL-4) lab in China relatively close (25 to 35 kilometers [15 to 22 miles]) to the Wuhan live-animal market at the epicenter of China's outbreak, has extensively published the genetic sequences of isolates from the bat coronaviruses she studies.
None of them match those of COVID-19, Andersen said, something Shi herself confirmed in a recent interview in Scientific American. "If she would have published a sequence for the virus and then this pops up, then we would have known it came from the lab," Andersen said. "There's no evidence for this, but there is plenty of evidence against it."
https://www.cidrap.umn.edu/news-per...tists-exactly-zero-evidence-covid-19-came-lab
https://www.scientificamerican.com/...wn-viruses-from-sars-to-the-new-coronavirus1/
More info is needed to determine if FL re-opened too soon. Their hot spot was the 3 south east counties which include Miami, Ft. Lauderdale and Palm Beach which have not been given permission to re-open. I'd like to see some info on the rest of the state - and keep in mind, their "re-opening" is still very restricted.
Posted this on a thread on the board but figured I'd post it here too.
Here's an article about a particle testing company who used the machine that is used to certify N95 masks to test different materials that people have used to make masks. Doesn't speak to the safety of some of the materials used and breathing in those particles of such material like vacuum bags/furnace filters...etc. They tested breathability and filtration levels and then also gave sort of a rating taking into account both breathability/filtration together. This isn't an expert study by scientists and such but after those fashion designers did those tests with the blue shop towels etc...they got some help from that particle testing company to take it a step further with the actual testing machine to test various materials....so while not formal lab setting it is some sort of gauge at least.
https://www.businessinsider.com/the...rticles-best-in-homemade-masks-testing-2020-4
https://www.maskfaq.com/test-results
Here's an article about a particle testing company who used the machine that is used to certify N95 masks to test different materials that people have used to make masks. Doesn't speak to the safety of some of the materials used and breathing in those particles of such material like vacuum bags/furnace filters...etc. They tested breathability and filtration levels and then also gave sort of a rating taking into account both breathability/filtration together. This isn't an expert study by scientists and such but after those fashion designers did those tests with the blue shop towels etc...they got some help from that particle testing company to take it a step further with the actual testing machine to test various materials....so while not formal lab setting it is some sort of gauge at least.
https://www.businessinsider.com/the...rticles-best-in-homemade-masks-testing-2020-4
https://www.maskfaq.com/test-results
another fake news post from the flu bro. Can you ever tell the truth?
It is balant BS posting by a clueless clown.
The number of hospitalizations for COVID currently in Florida is nearly at 8000. The highest it’s ever been.
Of course the 8000 is the highest ever, it's the cumulative count. D'uh. SHM.It is balant BS posting by a clueless clown.
The number of hospitalizations for COVID currently in Florida is nearly at 8000. The highest it’s ever been.

^ no acknowledgement of his errors and latches onto one thing to argue about. This nonsense is the basis of the CE board
+1^ no acknowledgement of his errors and latches onto one thing to argue about. This nonsense is the basis of the CE board
Agreed. RU#1 keeps throwing out numbers that he doesn't even know what they are.
T2K. Nice attempt to deflect.
(That was sarcasm in case I needed to explain it to you).
(That was sarcasm in case I needed to explain it to you).
8-minutes lingering in the air?
I'll continue to stay away from going inside of any structures
I'll continue to stay away from going inside of any structures
I'm starting to wonder about Martenson a bit. Don't get me wrong, I've watched every one of his videos since he started talking about covid and he has generally been on target. His early intuitions about this becoming a major/deadly pandemic obviously turned out to be true. However, his almost fanatical attachment to a couple of controversial points - HCQ and now the lab-engineered virus idea - have me questioning his motives. Is he just taking controversial/opposing viewpoints hoping to be proven right later? Back in January most didn't really seem too concerned with covid so at the time that was an opposing viewpoint. Since I never paid any attention to him before covid, I have no idea whether this is how he operates, i.e. harp on something controversial and if it pans out he looks like a star (and obviously he would benefit financially through subscriptions to his website). If he turns out wrong that kind of stuff will probably be quickly forgotten, for instance he'll just stop talking about HCQ if all the random trials show no benefit.
I don't know...still watch but starting to get a bit suspicious.
His latest is short but I highly recommend everyone watch it. My take is not that CM has taken a fanatical position on those things you mentioned. It is he is questioning the science behind statements and folks are having their BELIEFS challenged. I do not have a belief that HCQ works, only an opinion that we have not approached evaluating it in early use yet. I have no belief that the virus is man made only an opinion that what has been said is not proof that is wasn't. I have no emotion to those positions. If the UMN study shows definitively there is no help from HCQ, which it might very well, then out it goes as a treatment. If a virologist presents an explanation based on facts that this virus has not escaped from a lab so be it. That has not happened despite what some experts suggest. Read this paper by expert virologists:
https://wwwnc.cdc.gov/eid/article/26/7/20-0092_article
Although the Wuhan market was initially suspected to be the epicenter of the epidemic, the immediate source remains elusive. The close relatedness among SARS-CoV-2 strains suggested that the Wuhan outbreak probably originated from a point source with subsequent human-to-human transmission, in contrast to the polyphyletic origin of Middle East respiratory syndrome coronavirus (14). If the Wuhan market was the source, a possibility is that bats carrying the parental SARSr-BatCoVs were mixed in the market, enabling virus recombination. However, no animal samples from the market were reported to be positive. Moreover, the first identified case-patient and other early case-patients had not visited the market (15), suggesting the possibility of an alternative source.
Because the RBD is considered a hot spot for construction of recombinant CoVs for receptor and viral replication studies, the evolutionarily distinct SARS-CoV-2 RBD and the unique insertion of S1/S2 cleavage site among Sarbecovirus species have raised the suspicion of an artificial recombinant virus. However, there is currently no evidence showing that SARS-CoV-2 is an artificial recombinant, which theoretically might not carry signature sequences. Further surveillance studies in bats are needed to identify the possible source and evolutionary path of SARS-CoV-2.
She is covering her a$$. Read the article I posted please. I ran a ballistics test on my own gun, and it wasnt used in the crime. Trust me. https://www.nature.com/articles/nm.3985.pdfSo, in addition to the New England Journal of Medicine and Journal of the American Medical Association (and the people who recently published HCQ papers in those prestigious journals), you're now adding many of the most renowned evolutionary virologists to your list of people whose explanations you find laughable. That's quite a list.
I watched the video and he simply pieces together parts of what is known about viruses and then tries to convince people that somehow people in a lab, who had zero knowledge of what SARS-CoV-2 was (since the outbreak hadn't started yet), knew to take pieces from other viruses most closely related to CV2 and link them together into a new chimeric virus that became "almost CV2" and then evolved that chimeric virus into CV2 somehow. How the hell could they know to shoot for that endpoint out of the nearly infinite number of amino acid sequences that are possible for both the RNA and protein parts of the virus? That's simply not credible.
As per today's excellent article published by CIDRAP, another top-notch infectious disease research group out of the U of MN (led by world expert Michael Osterholm), the idea that someone was able to "create" CV2 is preposterous. Sure, if they were given the blueprints to CV2, someone could likely make it, but how would anyone know to make it out of so many possibilities? And as per the comment below, if someone were trying to create a bioweapon in a lab, why wouldn't they start from SARS or MERS, which were very close to being pandemic-worthy (and far deadlier than CV2)? And even if they somehow "made" CV2 in the lab, why would they have released it in their own country?
Furthermore, he questions why anyone would go through the work of creating a new virus when they could simply take an existing virulent pathogen like the SARS (severe acute respiratory syndrome) or MERS (Middle East respiratory syndrome) coronaviruses and make them even worse, as all bioweapons programs so far have done.
"It doesn't make any sense to make a new virus that you don't know can cause disease in humans and try to create a bioweapon out of it," Andersen said. "That would be a really bad bioweapons person."
And with regard to the other possibility people talk about, i.e., that they had somehow obtained CV2 from the wild and were working with it and accidentally released it, there's also no evidence for that. Dr. Shi Zhengli (the "batwoman") published all kinds of genetic sequences from various bat coronaviruses she and her research group have found and they published nothing that close to CV2 - if they had, perhaps lab release could be an issue.
Even Kristian Anderson (an expert virologist and lead author on the Nature paper), who originally thought it possible that the virus could have been accidentally released from a lab, said that while "he can't completely rule out the possibility that the virus came from a lab, the odds of that happening are very small. He says the new coronavirus clearly originated in nature, no question about it by now."
Lastly, Martenson's use of Occam's Razor is what's laughable. What's more likely: that CV2 came into being in the same way every other virus in the history of the planet did, i.e., by evolution in some species, like bats, and probable zoonotic transfer to humans either directly or through an intermediate host, or that some researchers in a lab, not knowing the endpoint blueprint for CV2 somehow figured out a way to construct CV2? Hint: it's not the latter.
Also, there's no proof of a blackout at the lab in October, either and Dr. Shi Zhengli is not missing. The Chinese have acted very badly with regard to lying and covering up the true extent of the outbreak, but they almost certainly didn't create the virus in a lab.
Shi Zhengli, PhD, director of the Center for Emerging Infectious Diseases at the Wuhan Institute of Virology, a biosafety level 4 (BSL-4) lab in China relatively close (25 to 35 kilometers [15 to 22 miles]) to the Wuhan live-animal market at the epicenter of China's outbreak, has extensively published the genetic sequences of isolates from the bat coronaviruses she studies.
None of them match those of COVID-19, Andersen said, something Shi herself confirmed in a recent interview in Scientific American. "If she would have published a sequence for the virus and then this pops up, then we would have known it came from the lab," Andersen said. "There's no evidence for this, but there is plenty of evidence against it."
https://www.cidrap.umn.edu/news-per...tists-exactly-zero-evidence-covid-19-came-lab
https://www.scientificamerican.com/...wn-viruses-from-sars-to-the-new-coronavirus1/
They don't have permission, but the ppl there certainly aren't following the rules, nor are they being enforced by LEO. Have a buddy who lives in Boca Raton and says that outdoor seating restaurants are packed, no one wears masks unless they're going into the grocery store.More info is needed to determine if FL re-opened too soon. Their hot spot was the 3 south east counties which include Miami, Ft. Lauderdale and Palm Beach which have not been given permission to re-open. I'd like to see some info on the rest of the state - and keep in mind, their "re-opening" is still very restricted.
I have in-laws in FL, little north of Daytona. You are right, restaurants are packed, no masks, beaches packed. Most of society is fully operational - big exception is theme parks and big events.They don't have permission, but the ppl there certainly aren't following the rules, nor are they being enforced by LEO. Have a buddy who lives in Boca Raton and says that outdoor seating restaurants are packed, no one wears masks unless they're going into the grocery store.
With regard to Florida, again some are declaring victory when the game is in the beginning of the 2nd quarter.
Let's revisit Florida at the end of the year. Same goes for Georgia.
Let's revisit Florida at the end of the year. Same goes for Georgia.
De Santis is doing an outstanding job in Florida rebuffing all those who piled on 8 weeks ago
Thank you for this. The Chris Martenson disciples on this thread and others are almost as insufferable as he is.So, in addition to the New England Journal of Medicine and Journal of the American Medical Association (and the people who recently published HCQ papers in those prestigious journals), you're now adding many of the most renowned evolutionary virologists to your list of people whose explanations you find laughable. That's quite a list.
I watched the video and he simply pieces together parts of what is known about viruses and then tries to convince people that somehow people in a lab, who had zero knowledge of what SARS-CoV-2 was (since the outbreak hadn't started yet), knew to take pieces from other viruses most closely related to CV2 and link them together into a new chimeric virus that became "almost CV2" and then evolved that chimeric virus into CV2 somehow. How the hell could they know to shoot for that endpoint out of the nearly infinite number of amino acid sequences that are possible for both the RNA and protein parts of the virus? That's simply not credible.
As per today's excellent article published by CIDRAP, another top-notch infectious disease research group out of the U of MN (led by world expert Michael Osterholm), the idea that someone was able to "create" CV2 is preposterous. Sure, if they were given the blueprints to CV2, someone could likely make it, but how would anyone know to make it out of so many possibilities? And as per the comment below, if someone were trying to create a bioweapon in a lab, why wouldn't they start from SARS or MERS, which were very close to being pandemic-worthy (and far deadlier than CV2)? And even if they somehow "made" CV2 in the lab, why would they have released it in their own country?
Furthermore, he questions why anyone would go through the work of creating a new virus when they could simply take an existing virulent pathogen like the SARS (severe acute respiratory syndrome) or MERS (Middle East respiratory syndrome) coronaviruses and make them even worse, as all bioweapons programs so far have done.
"It doesn't make any sense to make a new virus that you don't know can cause disease in humans and try to create a bioweapon out of it," Andersen said. "That would be a really bad bioweapons person."
And with regard to the other possibility people talk about, i.e., that they had somehow obtained CV2 from the wild and were working with it and accidentally released it, there's also no evidence for that. Dr. Shi Zhengli (the "batwoman") published all kinds of genetic sequences from various bat coronaviruses she and her research group have found and they published nothing that close to CV2 - if they had, perhaps lab release could be an issue.
Even Kristian Anderson (an expert virologist and lead author on the Nature paper), who originally thought it possible that the virus could have been accidentally released from a lab, said that while "he can't completely rule out the possibility that the virus came from a lab, the odds of that happening are very small. He says the new coronavirus clearly originated in nature, no question about it by now."
Lastly, Martenson's use of Occam's Razor is what's laughable. What's more likely: that CV2 came into being in the same way every other virus in the history of the planet did, i.e., by evolution in some species, like bats, and probable zoonotic transfer to humans either directly or through an intermediate host, or that some researchers in a lab, not knowing the endpoint blueprint for CV2 somehow figured out a way to construct CV2? Hint: it's not the latter.
Also, there's no proof of a blackout at the lab in October, either and Dr. Shi Zhengli is not missing. The Chinese have acted very badly with regard to lying and covering up the true extent of the outbreak, but they almost certainly didn't create the virus in a lab.
Shi Zhengli, PhD, director of the Center for Emerging Infectious Diseases at the Wuhan Institute of Virology, a biosafety level 4 (BSL-4) lab in China relatively close (25 to 35 kilometers [15 to 22 miles]) to the Wuhan live-animal market at the epicenter of China's outbreak, has extensively published the genetic sequences of isolates from the bat coronaviruses she studies.
None of them match those of COVID-19, Andersen said, something Shi herself confirmed in a recent interview in Scientific American. "If she would have published a sequence for the virus and then this pops up, then we would have known it came from the lab," Andersen said. "There's no evidence for this, but there is plenty of evidence against it."
https://www.cidrap.umn.edu/news-per...tists-exactly-zero-evidence-covid-19-came-lab
https://www.scientificamerican.com/...wn-viruses-from-sars-to-the-new-coronavirus1/
Last edited:
Finally, some data are starting to trickle in on convalescent plasma from the blood of infected/recovered COVID patients. A study in Italy with 46 patients reported a decrease in mortality from 15% typically observed to 6% for those receiving the plasma, which is huge. Not a "cure" but potentially huge. Not a lot of medical details in the attached translated article (so it's choppy), but this could be the most promising news yet on plasma. The intend to publish their findings on Thursday.
We've now treated almost 9000 patients with plasma at various participating hospitals in a program being overseen by the Mayo Clinic - dying to see results, although there have been lots of great success stories in the media so far.
https://www.ilgiorno.it/milano/cronaca/coronavirus-cura-plasma-1.5144652
Much more data in today in a paper by Joyner et al (preprint), evaluating the use of convalescent plasma in 5000 severely ill COVID-19 patients participating in the large observational trial (no control arm - essentially an emergency use "expanded access program") being run by the Mayo Clinic. Bottom line is it appears to be safe and "promising" with respect to lowering morality rates, although the study wasn't designed to evaluate that.
https://www.medrxiv.org/content/10.1101/2020.05.12.20099879v1.full.pdf
First off they concluded that CP is generally "safe" in the context of not adding additional risk to patients - all 5000 patients had "severe or life-threatening" cases of COVID-19. With regard to effectiveness, the analysis wasn't designed to evaluate that specifically, but they shared some data on 7-day mortality and to me the most striking data was that of the 3,316 patients admitted to the ICU, 456 mortalities were observed (16.7% after adjustments) vs. the typical mortality rate for ICU patients of 57% - that's a 71% reduction in morality rate for patients in the ICU and this wasn't a 10-person study or even a 46-person study (with 60% mortality reduction with CP), like the one above. However, it was only a 7-day analysis and perhaps those mortality numbers will increase significantly over time - would be nice to know what percentage of deaths occur beyond 7 days for such severely ill patients.
Of the 1682 hospitalized patients not admitted to the ICU the 7-day mortality rate was 11.2% vs. 15-20% typical for hospitalized patients, more like a 25-45% reduction; again, this was a 7-day mortality rate. However, NYC hospitalization mortality rates are about 33%, so the overall hospitalization mortality rate for this study, so far at 7 days (so not complete data yet) of 14.9% would be a 55% reduction. As an aside, I was a bit confused here, though - I would have thought patients sick enough to eventually die would go into the ICU first.
Anyway, it's not time to go out and celebrate yet, as this was not a placebo (plasma without antibodies)/standard of care controlled randomized double blind clinical study (that is ongoing), meaning the study was not designed to evaluate efficacy of CP per se, as per the excerpt below. However, the data above, especially the ICU data, are still pretty impressive, IMO, although it's only 7-day mortality data, so it's not complete yet. It's also a little bit odd that they didn't include the 57% typical ICU mortality rate comment together with the 13.7% ICU mortality rate data in this study - it's almost as if they don't want people hyping the potentially positive result (which I'm trying not to do; just sharing the data).
Over the first seven days after the convalescent plasma transfusion, a total of 602 mortalities were observed. The overall seven-day mortality rate was estimated to be 14.9% (95% CI: 13.8%, 16.0%) using the product limit estimator; an estimate that was numerically higher than the crude estimate of 12.0% at day 7. Of the 3,316 patients admitted to the ICU, 456 mortalities were observed (16.7%, 95% CI: 15.3%, 18.1%). Of the 1,682 hospitalized patients not-admitted to the ICU, 146 mortalities were observed (11.2%, 95% CI: 9.5%, 12.9%)...
...Although this study was not designed to evaluate efficacy of convalescent plasma we note with optimism the relatively low mortality in treated patients. The case fatality rate of COVID-19 has been reported to be ~4% among all persons diagnosed with COVID-19 (2); however, the case fatality rate among hospitalized patients is much higher ~15-20% (3, 5) and even more so among patients admitted to the ICU (57%) (4). Thus, the seven-day mortality rate was 14.9% reported here is not alarming, particularly because some of these plasma transfusions may be characterized as attempts at rescue or salvage therapy in patients admitted to the ICU with multi-organ failure, sepsis and significant comorbidities.
In addition, it's also noteworthy that the study did not find any obvious evidence of "antibody dependent enhancement" (ADE), which is a theoretical concern of the use of convalescent plasma, which could lead to "deteriorated clinical condition after plasma transfusion secondary to antibody-dependent enhancement (ADE) of infection or antibody-mediated proinflammatory effects." Limited evidence of this was seen with antibody therapies for other coronaviruses.
The absence of a toxicity signature with the use of convalescent plasma in individuals with COVID-19 implies that this phenomenon may be clinically inconsequential. COVID-19 is known to elicit high neutralizing antibody titers in individuals who have recently recovered from infection and three case series of convalescent plasma administration also describe no deleterious ADE effects after infusion (27-29).
Way, way too premature to conclude anything yet in Florida. De Santis has little understanding of the risks of the virus and reopening without data to support it and without requiring masks, especially in indoor spaces, but outdoor spaces, too, where social distancing isn't possible (city streets, certainly mass transit, any gatherings, etc.).De Santis is doing an outstanding job in Florida rebuffing all those who piled on 8 weeks ago
Anecdotal evidence of lack of mask wearing and social distancing in FL (my sister and father live there and have been appalled by both over the past week or so) likely means an increase in cases soon (remember it's a 5-day incubation period before symptoms) and deaths in a few weeks, although that will likely be significantly slower, still, than it would be if all large public/private gatherings were being held and they're still not. Let's see where we are in about 2-3 weeks.
Of course the 8000 is the highest ever, it's the cumulative count. D'uh. SHM.
No moron ... it’s the current number of Hospitalizations for Florida for COVID. Not an total number since the beginning.
Trumpanzee clowns like you , BAC, just don’t get it.
https://www.pharmacytimes.com/news/novel-drug-may-reduce-inflammation-in-critical-covid-19-patients
Leronlimab article posted 2 days ago
Leronlimab article posted 2 days ago
Just for a positive story. 108 year lady from NJ recovers from COVID.
from the article:
Last month, 108-year-old Sylvia Goldscholl of Allendale, New Jersey, was diagnosed with Covid-19.
Today Goldscholl has recovered from the virus, Gov. Phil Murphy said at a news conference.
“She was 7 years old during the 1918 flu pandemic and she survived it. Last month, Sylvia tested positive for Covid-19 and now we can say she has beaten that,” Murphy said.
The governor added: “A tremendous life. A tremendous spirit, A tremendous show of strength. A tremendous role model for all of the rest of us."
https://www.cnn.com/us/live-news/us-coronavirus-update-05-14-20/h_00ad6769c2a34e03749e6c8109e885f7
from the article:
Last month, 108-year-old Sylvia Goldscholl of Allendale, New Jersey, was diagnosed with Covid-19.
Today Goldscholl has recovered from the virus, Gov. Phil Murphy said at a news conference.
“She was 7 years old during the 1918 flu pandemic and she survived it. Last month, Sylvia tested positive for Covid-19 and now we can say she has beaten that,” Murphy said.
The governor added: “A tremendous life. A tremendous spirit, A tremendous show of strength. A tremendous role model for all of the rest of us."
https://www.cnn.com/us/live-news/us-coronavirus-update-05-14-20/h_00ad6769c2a34e03749e6c8109e885f7
Laughing at you:No moron ... it’s the current number of Hospitalizations for Florida for COVID. Not an total number since the beginning.
Trumpanzee clowns like you , BAC, just don’t get it.
https://floridadisaster.org/globala...id-19-data---daily-report-2020-05-14-10am.pdf
Page #1 - 3rd item on the right.
[roll]
Florida's hospitalization numbers are cumulative. This has been written about, critically, in many publications. Their numbers are also quite suspect, since their overall bed census (61% of capacity, statewide) is generally higher than other states. There are three possible conclusions to draw from this data point, alone:
1. Florida has a lower per capita bed capacity than other states (this is doubtful)
2. Florida's citizens are hospitalized at a higher rate than in other states
3. They're lying about their Covid admissions
It is more than a little curious that they won't publish current Covid census numbers, since all other states do. So when deSantis says "hospital admissions for Covid-19 are declining" there's no data to back up that claim.
1. Florida has a lower per capita bed capacity than other states (this is doubtful)
2. Florida's citizens are hospitalized at a higher rate than in other states
3. They're lying about their Covid admissions
It is more than a little curious that they won't publish current Covid census numbers, since all other states do. So when deSantis says "hospital admissions for Covid-19 are declining" there's no data to back up that claim.
BOOM!
:)
You'd be best served by reading and understanding everything, instead of finding the one word in a hundred that you think proves your point.
Your approach to things is infantile. My dog has better reasoning skills than you typically display, here.
Too bad, thought your dog was smarter than that...You'd be best served by reading and understanding everything, instead of finding the one word in a hundred that you think proves your point.
Your approach to things is infantile. My dog has better reasoning skills than you typically display, here.
Edit: as has been the case NJ get's a late day bump as data comes in. Deaths currently reported as 223 for the day, new cases at 727 and that will likely bump up even more as well given Bergen has not yet reported.
In NJ we continue to see our #'s trend in a very positive direction. Not all great news as our 219 reported death's today was the worst in the nation, and our 3 day average is still a hair over 200 per day.
But we do need to acknowledge the reporting patterns, and NJ does report more #'s Tues-Thurs then the rest of the week. Last week the 3 day average was 293 deaths Tues-Thrus. So week over week, significant decline even though we lead the nation.
Even better news is the 613 new cases, which is the lowest daily new case count since March 22, and the 10th highest in the country. Two day total of 1405 is lower then the states one day total from Sunday. We were consistently over 2000 daily new cases just 10 days ago.
I do wonder about the # of tests we are doing per day. But on the surface very encouraging news, and they might be even better then the surface #'s suggest if we are indeed testing more people.
https://www.worldometers.info/coronavirus/usa/new-jersey/
In NJ we continue to see our #'s trend in a very positive direction. Not all great news as our 219 reported death's today was the worst in the nation, and our 3 day average is still a hair over 200 per day.
But we do need to acknowledge the reporting patterns, and NJ does report more #'s Tues-Thurs then the rest of the week. Last week the 3 day average was 293 deaths Tues-Thrus. So week over week, significant decline even though we lead the nation.
Even better news is the 613 new cases, which is the lowest daily new case count since March 22, and the 10th highest in the country. Two day total of 1405 is lower then the states one day total from Sunday. We were consistently over 2000 daily new cases just 10 days ago.
I do wonder about the # of tests we are doing per day. But on the surface very encouraging news, and they might be even better then the surface #'s suggest if we are indeed testing more people.
https://www.worldometers.info/coronavirus/usa/new-jersey/
Last edited:
Florida's highest daily new case count in May, prior to Tuesday, was 772. And only 3 days in May over 700 new cases prior to Tuesday. The last 3 days have each been over 800.FL confirmed cases are trending down, deaths are trending down, and % of positive tests are going down.
https://experience.arcgis.com/experience/96dd742462124fa0b38ddedb9b25e429
The daily death count total can be deceiving if you are looking for trends in the near term as they retroactively attribute deaths to dates. When you look at Worldometer you see 47 deaths for 3 straight days(which in itself raises an eyebrow) but the dashboard is showing 17 for Tuesday. We will likely see the dashboard #'s rise. But you are correct on this one as both the dashboard and worldometer are showing a decline trend in death totals.
The site I was using from the Florida dept. of health that gave the breakdown in terms of daily positive test % is not working at the moment. I'll post it if and when it does.
Can't take it back, so I repeat:You'd be best served by reading and understanding everything, instead of finding the one word in a hundred that you think proves your point.
Your approach to things is infantile. My dog has better reasoning skills than you typically display, here.
BOOM!
:)
Double BOOM!But you are correct on this one as both the dashboard and worldometer are showing a decline trend in death totals.
:)
So getting one fact correct out of 3 is worthy of a BOOM!!! in your world?Double BOOM!
:)
:Wink:
Thanks for the posts, always find some good info in them. I know you have been waiting on clinical data for this approach for sometime. For those of us (raises hand) who don't know how this works, care to explain?Much more data in today in a paper by Joyner et al (preprint), evaluating the use of convalescent plasma in 5000 severely ill COVID-19 patients participating in the large observational trial (no control arm - essentially an emergency use "expanded access program") being run by the Mayo Clinic. Bottom line is it appears to be safe and "promising" with respect to lowering morality rates, although the study wasn't designed to evaluate that.
https://www.medrxiv.org/content/10.1101/2020.05.12.20099879v1.full.pdf
First off they concluded that CP is generally "safe" in the context of not adding additional risk to patients - all 5000 patients had "severe or life-threatening" cases of COVID-19. With regard to effectiveness, the analysis wasn't designed to evaluate that specifically, but they shared some data on 7-day mortality and to me the most striking data was that of the 3,316 patients admitted to the ICU, 456 mortalities were observed (16.7% after adjustments) vs. the typical mortality rate for ICU patients of 57% - that's a 71% reduction in morality rate for patients in the ICU and this wasn't a 10-person study or even a 46-person study (with 60% mortality reduction with CP), like the one above. However, it was only a 7-day analysis and perhaps those mortality numbers will increase significantly over time - would be nice to know what percentage of deaths occur beyond 7 days for such severely ill patients.
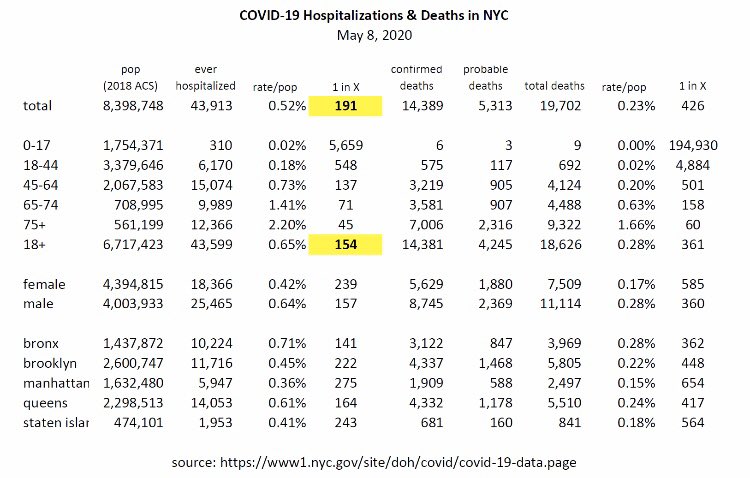
Of the 1682 hospitalized patients not admitted to the ICU the 7-day mortality rate was 11.2% vs. 15-20% typical for hospitalized patients, more like a 25-45% reduction; again, this was a 7-day mortality rate. However, NYC hospitalization mortality rates are about 33%, so the overall hospitalization mortality rate for this study, so far at 7 days (so not complete data yet) of 14.9% would be a 55% reduction. As an aside, I was a bit confused here, though - I would have thought patients sick enough to eventually die would go into the ICU first.
Anyway, it's not time to go out and celebrate yet, as this was not a placebo (plasma without antibodies)/standard of care controlled randomized double blind clinical study (that is ongoing), meaning the study was not designed to evaluate efficacy of CP per se, as per the excerpt below. However, the data above, especially the ICU data, are still pretty impressive, IMO, although it's only 7-day mortality data, so it's not complete yet. It's also a little bit odd that they didn't include the 57% typical ICU mortality rate comment together with the 13.7% ICU mortality rate data in this study - it's almost as if they don't want people hyping the potentially positive result (which I'm trying not to do; just sharing the data).
Over the first seven days after the convalescent plasma transfusion, a total of 602 mortalities were observed. The overall seven-day mortality rate was estimated to be 14.9% (95% CI: 13.8%, 16.0%) using the product limit estimator; an estimate that was numerically higher than the crude estimate of 12.0% at day 7. Of the 3,316 patients admitted to the ICU, 456 mortalities were observed (16.7%, 95% CI: 15.3%, 18.1%). Of the 1,682 hospitalized patients not-admitted to the ICU, 146 mortalities were observed (11.2%, 95% CI: 9.5%, 12.9%)...
...Although this study was not designed to evaluate efficacy of convalescent plasma we note with optimism the relatively low mortality in treated patients. The case fatality rate of COVID-19 has been reported to be ~4% among all persons diagnosed with COVID-19 (2); however, the case fatality rate among hospitalized patients is much higher ~15-20% (3, 5) and even more so among patients admitted to the ICU (57%) (4). Thus, the seven-day mortality rate was 14.9% reported here is not alarming, particularly because some of these plasma transfusions may be characterized as attempts at rescue or salvage therapy in patients admitted to the ICU with multi-organ failure, sepsis and significant comorbidities.
In addition, it's also noteworthy that the study did not find any obvious evidence of "antibody dependent enhancement" (ADE), which is a theoretical concern of the use of convalescent plasma, which could lead to "deteriorated clinical condition after plasma transfusion secondary to antibody-dependent enhancement (ADE) of infection or antibody-mediated proinflammatory effects." Limited evidence of this was seen with antibody therapies for other coronaviruses.
The absence of a toxicity signature with the use of convalescent plasma in individuals with COVID-19 implies that this phenomenon may be clinically inconsequential. COVID-19 is known to elicit high neutralizing antibody titers in individuals who have recently recovered from infection and three case series of convalescent plasma administration also describe no deleterious ADE effects after infusion (27-29).
I just read the part that agrees with me.So getting one fact correct out of 3 is worthy of a BOOM!!! in your world?
:Wink:
Just want to revisit this point, as I think it is a good one, in regards to states that have opened up.Yeah that’s what I hope. Well not gradual increase, maybe just a very long plateau, which at their levels would be ok.
Texas is seeing a jump in cases, 1600 yesterday was their highest total to date. Now as I noted above you have to consider they are likely testing more people, but you also have to consider that in a state as big as Texas, and similarly for Florida, that # is likely a level their health care system can handle, especially if, as I would suspect, it has been beefed up in preparation for reopening.
I think everyone was aware that the #'s were going to increase, and that includes deaths, but will those #'s go beyond a level a state's system can handle.
Will be interesting to see if any state can keep the virus out of their LTC's, not many states have proven proficient in this regard thus far.
That math adds up.I just read the part that agrees with me.
Florida's hospitalization numbers are cumulative. This has been written about, critically, in many publications. Their numbers are also quite suspect, since their overall bed census (61% of capacity, statewide) is generally higher than other states. There are three possible conclusions to draw from this data point, alone:
1. Florida has a lower per capita bed capacity than other states (this is doubtful)
2. Florida's citizens are hospitalized at a higher rate than in other states
3. They're lying about their Covid admissions
It is more than a little curious that they won't publish current Covid census numbers, since all other states do. So when deSantis says "hospital admissions for Covid-19 are declining" there's no data to back up that claim.
Florida's current hospitalization for Covid-19 is 472 with 232 in the ICU. FWIW, the covid tracking project, which compiles all of this information and the accuracy of which I have not seen questioned, gives Florida an "A+" in the amount of data it is making publicly available.
https://covidtracking.com/data/state/florida
- Status
- Not open for further replies.
Similar threads
- Replies
- 93
- Views
- 3K
- Replies
- 8
- Views
- 1K
- Replies
- 7
- Views
- 659
- Replies
- 0
- Views
- 1K
ADVERTISEMENT
ADVERTISEMENT