
For those who have done the antibody test, are the test environments clean? I feel like a labcorp facility would probably have the virus circulating on the premises with a higher risk of infection than not getting the test. Currently debating whether or not to get the test.
Colleges
- American Athletic
- Atlantic Coast
- Big 12
- Big East
- Big Ten
- Colonial
- Conference USA
- Independents (FBS)
- Junior College
- Mountain West
- Northeast
- Pac-12
- Patriot League
- Pioneer League
- Southeastern
- Sun Belt
- Army
- Charlotte
- East Carolina
- Florida Atlantic
- Memphis
- Navy
- North Texas
- Rice
- South Florida
- Temple
- Tulane
- Tulsa
- UAB
- UTSA
- Boston College
- California
- Clemson
- Duke
- Florida State
- Georgia Tech
- Louisville
- Miami (FL)
- North Carolina
- North Carolina State
- Pittsburgh
- Southern Methodist
- Stanford
- Syracuse
- Virginia
- Virginia Tech
- Wake Forest
- Arizona
- Arizona State
- Baylor
- Brigham Young
- Cincinnati
- Colorado
- Houston
- Iowa State
- Kansas
- Kansas State
- Oklahoma State
- TCU
- Texas Tech
- UCF
- Utah
- West Virginia
- Illinois
- Indiana
- Iowa
- Maryland
- Michigan
- Michigan State
- Minnesota
- Nebraska
- Northwestern
- Ohio State
- Oregon
- Penn State
- Purdue
- Rutgers
- UCLA
- USC
- Washington
- Wisconsin
High Schools
- Illinois HS Sports
- Indiana HS Sports
- Iowa HS Sports
- Kansas HS Sports
- Michigan HS Sports
- Minnesota HS Sports
- Missouri HS Sports
- Nebraska HS Sports
- Oklahoma HS Sports
- Texas HS Hoops
- Texas HS Sports
- Wisconsin HS Sports
- Cincinnati HS Sports
- Delaware
- Maryland HS Sports
- New Jersey HS Hoops
- New Jersey HS Sports
- NYC HS Hoops
- Ohio HS Sports
- Pennsylvania HS Sports
- Virginia HS Sports
- West Virginia HS Sports
ADVERTISEMENT
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
COVID-19 Pandemic: Transmissions, Deaths, Treatments, Vaccines, Interventions and More...
- Thread starter RU848789
- Start date
- Status
- Not open for further replies.
This one's for you @SkilletHead2 - not sure if I've seen you post on this, but New Zealand thinks they have "effectively eliminated" the coronavirus, via a travel ban from China on 2/2, full quarantine of all visitors starting 3/15 (when they only had 6 cases), aggressive early testing/tracing (they're in the top 10% of countries on testing per capita) and a strict lockdown starting 3/25, which is largely over now that new cases are down to zero. The country's 39-year old PM was able to get buy-in on the approach with the help of a team of scientists and health professionals, who are with her every day at their press updates. They've also been truthful with their people that this will require some austerity for awhile and the populace has responded, as they generally trust their government. Hmmm, trust and leadership.
https://www.nationalgeographic.com/...20200505&rid=3F7A7D00850AD922736B3173646A296D
The sudden austerity could have been a cause for panic. But each day, the 39-year-old Ardern, or “Jaz” as she’s popularly known, made clear, concise statements about the situation to the nation, bolstered by a team of scientists and health professionals. A few days after the lockdown, she announced that instead of just slowing the transmission of the virus, New Zealand had set a course of eradicating COVID-19 from its shores, by cutting off the arrival of new cases and choking out existing ones with the restrictions. “We have the opportunity to do something no other country has achieved: elimination of the virus,” said Ardern at one of her daily briefings.
From an outsider’s perspective, the interesting thing about New Zealand is that the country simply got on board. On day one of the lockdown, the streets and highways were empty, the shops were closed, and everyone stayed home. “I think it’s easier for us Kiwis to fall in line because we trust our leaders,” Sue Webster, the owner of the Airbnb where my wife and I holed up for almost four weeks, told me.
https://www.nationalgeographic.com/...20200505&rid=3F7A7D00850AD922736B3173646A296D
The sudden austerity could have been a cause for panic. But each day, the 39-year-old Ardern, or “Jaz” as she’s popularly known, made clear, concise statements about the situation to the nation, bolstered by a team of scientists and health professionals. A few days after the lockdown, she announced that instead of just slowing the transmission of the virus, New Zealand had set a course of eradicating COVID-19 from its shores, by cutting off the arrival of new cases and choking out existing ones with the restrictions. “We have the opportunity to do something no other country has achieved: elimination of the virus,” said Ardern at one of her daily briefings.
From an outsider’s perspective, the interesting thing about New Zealand is that the country simply got on board. On day one of the lockdown, the streets and highways were empty, the shops were closed, and everyone stayed home. “I think it’s easier for us Kiwis to fall in line because we trust our leaders,” Sue Webster, the owner of the Airbnb where my wife and I holed up for almost four weeks, told me.

Interesting BBC video about how Mahan Air, an Iranian airline linked to the Iranian Revolutionary Guard, continued to operate in the region up until April 20th despite bans on air travel. It appears they played a significant role in spreading the Wuhan Virus throughout the region.
Coronavirus by air: The spread of Covid-19 in the Middle East
Coronavirus by air: The spread of Covid-19 in the Middle East
CV kills Fed Ex workers in NJ
https://www.foxbusiness.com/lifestyle/fedex-worker-coronavirus-death-safety-protocols
https://www.foxbusiness.com/lifestyle/fedex-worker-coronavirus-death-safety-protocols
Doctors in France discover a Covid case there from December
https://www.wsj.com/articles/corona...as-france-discovers-december-case-11588700408
https://www.wsj.com/articles/corona...as-france-discovers-december-case-11588700408

The obese represent what, half of the US population? Thats an enormous number thif wouldpeoplle who can't return. You would think this would be good motivation for people to lose weight.We should have done this to begin with, but way too many CLs. By the way, UK's reopening plan calls for everyone to return to life and work except for people over 70+ or obese (the 2 biggest risk groups). Interesting.
For those who have done the antibody test, are the test environments clean? I feel like a labcorp facility would probably have the virus circulating on the premises with a higher risk of infection than not getting the test. Currently debating whether or not to get the test.
My brother had it done on Thursday at a LabCorp in Manhattan. No one is allowed in the waiting room, unless accompanying a minor. No problems. Very clean. He should hear any day now.
You're correct that neither is definitive, but I think the weight of evidence of the trials so far leans heavily towards lack of efficacy and several of my clinical expert colleagues agree, as does Derek Lowe and Dr. Bright, who was just sacked and the fact that HCQ is being used so much without any startlingly good results is enough for me to say that, at best, it's efficacy is marginal. Also, convalescent plasma is certainly viable in poor countries, with just a little help - hell, it was used in the 1890s and the 1918 pandemic.
Did you see Dr. Bright's comments after being sacked from his post at HHS, where he was deputy assistant secretary for preparedness and response and director of BARDA, the Biomedical Advanced Research and Development Authority (excerpted below)? Lowe and Bright are two of our best minds and I'll take their take on HCQ (as well as my friends' views).
https://blogs.sciencemag.org/pipeline/archives/2020/04/22/the-politics-of-hydroxychloroquine
“. . .To this point, I have led the government’s efforts to invest in the best science available to combat the Covid-19 pandemic. Unfortunately, this resulted in clashes with H.H.S. political leadership, including criticism for my proactive efforts to invest early into vaccines and supplies critical to saving American lives. I also resisted efforts to fund potentially dangerous drugs promoted by those with political connections.
Specifically, and contrary to misguided directives, I limited the broad use of chloroquine and hydroxychloroquine, promoted by the administration as a panacea, but which clearly lack scientific merit. While I am prepared to look at all options and to think ‘outside the box’ for effective treatments, I rightly resisted efforts to provide an unproven drug on demand to the American public. I insisted that these drugs be provided only to hospitalized patients with confirmed Covid-19 while under the supervision of a physician. . .”
Well, Dr. Bright has filed a whistleblower complaint related to his "reassignment," alleging his coronavirus warnings were being ignored. Was wondering if he was going to go that route after reading his interview with the Times quoted above. While this should probably be a separate thread on the CE board, I do think it's news and that people reading this thread should be aware of it. To try to keep it from going off the rails here, I'll leave it without further comment.
https://www.cnn.com/2020/05/05/politics/rick-bright-complaint/index.html
+1The obese represent what, half of the US population? Thats an enormous number thif wouldpeoplle who can't return. You would think this would be good motivation for people to lose weight.
The nation needs to lose weight:
The U.S. Obesity Rate Now Tops 40%
https://www.usnews.com/news/healthi.../2020-02-27/us-obesity-rate-passes-40-percent
What exactly is the point of getting an "antibody" test?
Other than being able to post online "I got an antibody test".
It's not like if you are positive then you are exempt from SD restrictions.
A negative test is worthless and doesn't prove anything.
It's a point in time test.
If you've gone outside, you are back in the "could have it maybe or not have it" bucket.
Has it even been definitively determined that you cannot become infected a 2nd time?
Other than being able to post online "I got an antibody test".
It's not like if you are positive then you are exempt from SD restrictions.
A negative test is worthless and doesn't prove anything.
It's a point in time test.
If you've gone outside, you are back in the "could have it maybe or not have it" bucket.
Has it even been definitively determined that you cannot become infected a 2nd time?
What exactly is the point of getting an "antibody" test?
Other than being able to post online "I got an antibody test".
It's not like if you are positive then you are exempt from SD restrictions.
A negative test is worthless and doesn't prove anything.
It's a point in time test.
If you've gone outside, you are back in the "could have it maybe or not have it" bucket.
Has it even been definitively determined that you cannot become infected a 2nd time?
For the most part, yes. If I test positive, I’m on the next flight to the Caribbean.
Being antibody positive is very meaningful. Those folks should be exempt from most restrictions since you are protected from getting or passing it along any more.What exactly is the point of getting an "antibody" test?
Other than being able to post online "I got an antibody test".
It's not like if you are positive then you are exempt from SD restrictions.
A negative test is worthless and doesn't prove anything.
It's a point in time test.
If you've gone outside, you are back in the "could have it maybe or not have it" bucket.
Has it even been definitively determined that you cannot become infected a 2nd time?
Damn straight!For the most part, yes. If I test positive, I’m on the next flight to the Caribbean.
:ThumbsUp
Being antibody positive is very meaningful. Those folks should be exempt from most restrictions since you are protected from getting or passing it along any more.
In an ideal state.
But that's not the case currently.
I understand the point of getting tested later but dont understand the point of getting tested under current restriction laws.
I know a guy who is 65ish and a smoker, his job is still open but he is concerned about spending 8 hours in a work place where hundreds of patrons enter everyday. If he tests positive for antibodies, that means(I think?) he is in the clear.What exactly is the point of getting an "antibody" test?
Other than being able to post online "I got an antibody test".
It's not like if you are positive then you are exempt from SD restrictions.
A negative test is worthless and doesn't prove anything.
It's a point in time test.
If you've gone outside, you are back in the "could have it maybe or not have it" bucket.
Has it even been definitively determined that you cannot become infected a 2nd time?
In theory, yes, but most of the tests out there have way too high a level of false positives to give high confidence that one truly is positive and has protective antibodies. At low prevalence rates (and almost everywhere is <5% outside of highly urban areas that have much higher case rates, like NYC metro, which is around 20% prevalence), such as ~3%, a positive test, even with a 99% specificity test likely only gives one 75% confidence in it being a true positive and a lot less confidence with most of the tests being used (that often have 95% specificity). Last thing I'd want to do is think I'm immune and then find out the hard way I'm not.Being antibody positive is very meaningful. Those folks should be exempt from most restrictions since you are protected from getting or passing it along any more.
The new Roche/Abbott tests claim 99.8/99.5% specificity, which means very low false positives, but not zero and I'd at least like to see some real world use data first. There are a few tests out there that list 100% specificity (no false positives), but I'm not even sure that's possible. Of course, if I were fairly young and had no other issues and had a positive test, I'd go out and not worry about getting infected, but I'd still wear a mask, just in case the test was wrong, so as to not infect anyone else on the small chance I might still get COVID. If I were at any risk, I'd likely get a 2nd confirming test to be sure.
https://www.evaluate.com/vantage/ar.../roche-takes-abbott-covid-19-antibody-testing
Here's the paper upon which I assume Abbott made their claims. Methodology looks sound (tested in pre-COVID negative samples and known positive viral samples), which is great; presumably Roche has done something similar. Great to have two tests that look so good.
https://www.medrxiv.org/content/10.1101/2020.04.27.20082362v1
However, keep in mind that when the prevalence of a condition being tested, like those with antibodies, is low, the math makes it very hard to "know" for sure if your positive antibody test is correct.
For example, with a prevalence of 5% antibodies in the population and a 99.9% sensitivity (hard to imagine any test being truly 100.0% accurate) and a 99.5% specificity, the calculator in the link below still shows that if you took the test and got a positive result, there’s a 90.9% chance it’s correct. If you got a negative result, there’s a 100% chance your result is accurate. Some might not take this chance.
If the prevalence is greater, like it is in NYC (~20%), then if you took the test and got a positive result, there’s a 99.5% chance it’s correct. If you got a negative result, there’s a 100% chance your result is accurate. Most would likely take this small chance of a false positive.
https://qz.com/1848674/how-to-interpret-the-specificity-sensitivity-of-antibody-tests/
I had mine done yesterday at Quest. Only 2 people were allowed in the waiting room, masks were required and gloves were provided for when you check in on the touch screen. The only concern would be if the phlebotomist is sick but they're just as worried about patients being sick. And yes, Quest is using the Abbott test. The Abbott test was being used by and tested by the University of Washington when it was released. An article I read quoted one of their researchers as saying, "It's a fantastic test".For those who have done the antibody test, are the test environments clean? I feel like a labcorp facility would probably have the virus circulating on the premises with a higher risk of infection than not getting the test. Currently debating whether or not to get the test.
Positive test = no mask, no restrictions, big partying!In theory, yes, but most of the tests out there have way too high a level of false positives to give high confidence that one truly is positive and has protective antibodies. At low prevalence rates (and almost everywhere is <5% outside of highly urban areas that have much higher case rates, like NYC metro, which is around 20% prevalence), such as ~3%, a positive test, even with a 99% specificity test likely only gives one 75% confidence in it being a true positive and a lot less confidence with most of the tests being used (that often have 95% specificity). Last thing I'd want to do is think I'm immune and then find out the hard way I'm not.
The new Roche/Abbott tests claim 99.8/99.5% specificity, which means very low false positives, but not zero and I'd at least like to see some real world use data first. There are a few tests out there that list 100% specificity (no false positives), but I'm not even sure that's possible. Of course, if I were fairly young and had no other issues and had a positive test, I'd go out and not worry about getting infected, but I'd still wear a mask, just in case the test was wrong, so as to not infect anyone else on the small chance I might still get COVID. If I were at any risk, I'd likely get a 2nd confirming test to be sure.
https://www.evaluate.com/vantage/ar.../roche-takes-abbott-covid-19-antibody-testing
I'm 50/50 that we already had it. There was a weird non-flu yet flu-like something going around my daughter's class throughout Feb. Our daughter picked up something mild and we always get what she gets. Also, had a work colleague pick-up something after a conference in Milan in late Feb. We met numerous times prior to the office closing and her symptoms popping up (never confirmed with a test, but her doc said it likely was corona). She's a MD and said it definitely wasn't the flu.
We may be lucky already.
I had mine done yesterday at Quest. Only 2 people were allowed in the waiting room, masks were required and gloves were provided for when you check in on the touch screen. The only concern would be if the phlebotomist is sick but they're just as worried about patients being sick. And yes, Quest is using the Abbott test. The Abbott test was being used by and tested by the University of Washington when it was released. An article I read quoted one of their researchers as saying, "It's a fantastic test".
Finger prick or do they draw a vial from your arm?
Of course, if I were fairly young and had no other issues and had a positive test, I'd go out and not worry about getting infected, but I'd still wear a mask, just in case the test was wrong, so as to not infect anyone else on the small chance I might still get COVID.
That's what I don't understand about getting the test now.
I'm fairly young, no other issues and not overly worried about getting infected (go to Dunkin daily but am smart and wipe stuff down, etc.).
If I got a positive antibody test and went to Dunkin to get a coffee - I still have to wear a mask. I can't tell them "oh I'm good."
If I go grocery shopping I still have to wear a mask and follow SD rules.
There is no real incentive to bother getting a test currently.
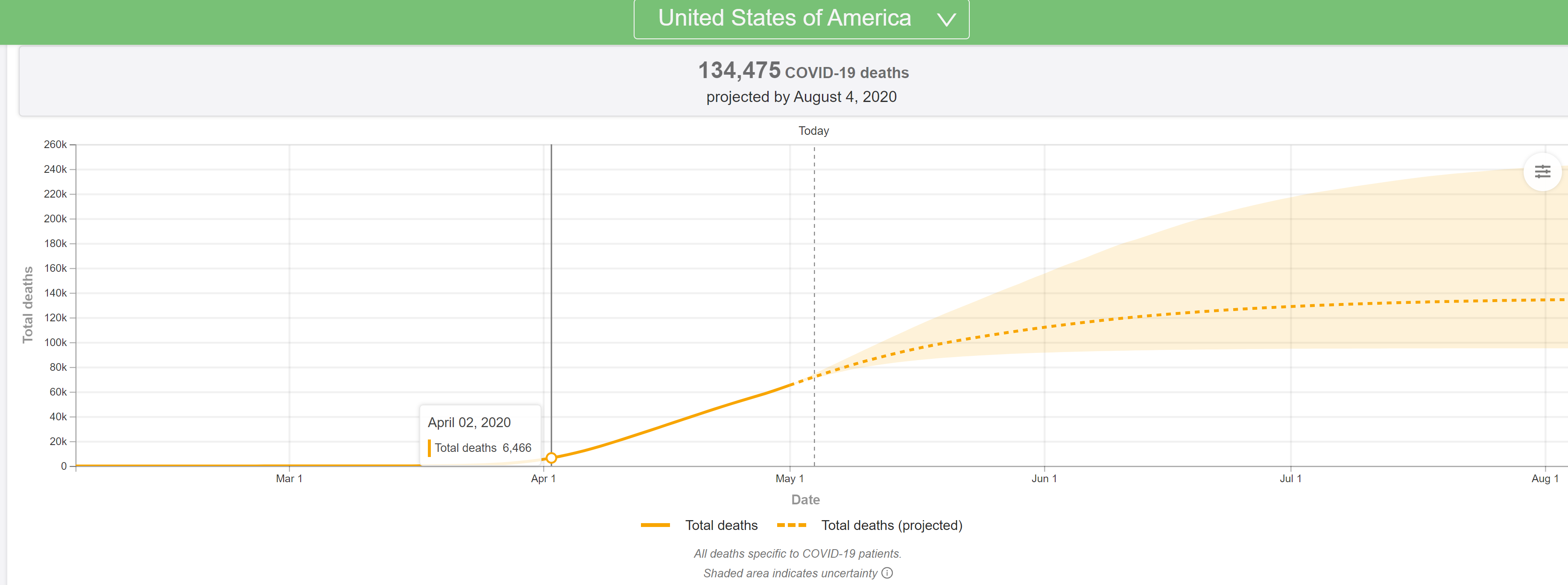
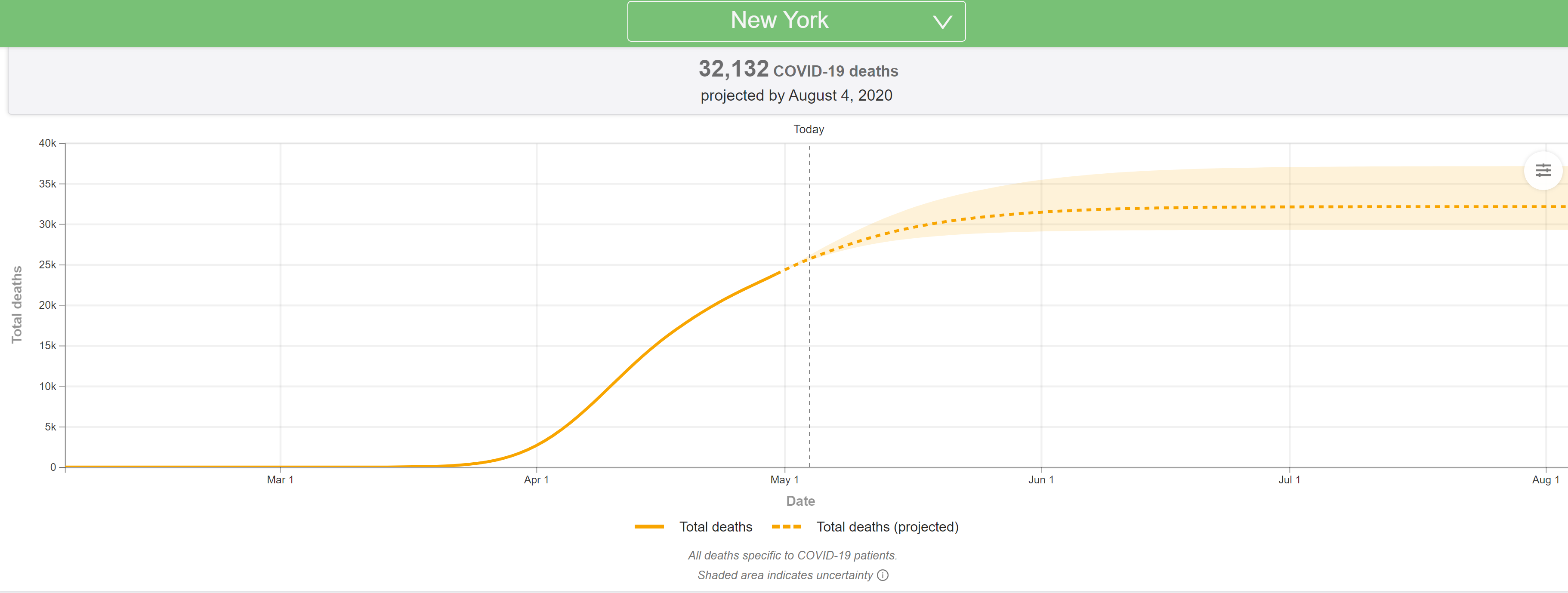
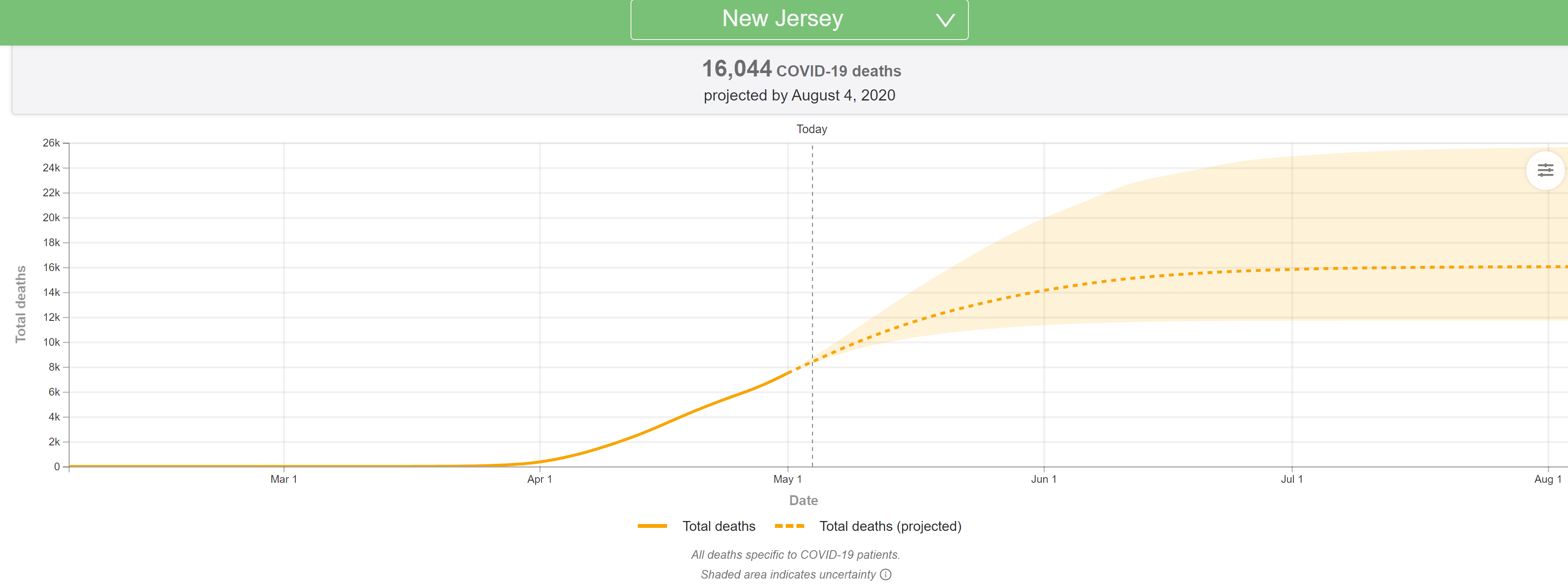
The latest (5/4) projections are out from the U of Washington/IHME and they're very bad, with the US deaths predicted to jump from the 72K in the 4/27 model to 134K through the end of July in the 5/4 model run. NY deaths are modeled to increase from 24K in the 4/27 model to 32K in the 5/4 model (more distancing modeled, hence the smaller increase vs. the US) and NJ deaths are modeled to increase from 7,2K in the 4/27 mode to 16K in the 5/4 model (not clear why NJ wasn't treated like NY).
They've completely overhauled the model and are now factoring in an increase in deaths due to expected significant increases in transmissions related to significant relaxation of stay at home policies and social distancing efforts, as well as slower than expected declines in deaths everywhere, once peaks are reached and passed. Haven't had time to go through it all, as there's a ton of new info, but did include the updated US/NY/NJ graphics. Will update this post with more later...
In addition, the Times obtained an internal CDC report from internal modeling, which is also predicting roughly a doubling of deaths from the current 68K (that would be 136K) by mid-summer, but the Administration is pushing back on that saying the report hasn't been fully vetted yet. However, President Trump on Sunday said deaths could reach 100K, so it certainly seems like forecasts are getting worse, even if not final yet. In that CDC report, it shows deaths per day increasing from the current ~2000/day to over 3000 per day by June.
https://covid19.healthdata.org/united-states-of-america
https://www.nytimes.com/2020/05/04/us/coronavirus-live-updates.html#link-32993cff
https://int.nyt.com/data/documenthe...f7319f4a55fd0ce5dc9/optimized/full.pdf#page=1
As I have been saying for the past week or so and which the Wharton model clearly confirmed on Friday, if restrictive policies are relaxed and social distancing lessened significantly, as looks to be happening, without an infrastructure to test massively and rapidly to detect outbreaks and to trace contacts and isolate positives and contacts, like South Korea and Taiwan have done (which we don't appear to be ready/willing to implement), deaths will get far worse than most have been projecting (including me). If one assumes a 60% infection endpoint (near herd immunity) and a very conservative 0.2% infection fatality rate (NY is at 0.7% now), then about ~400K US deaths would occur in the next 6-12 months if we open it all back up, but if we use an IFR of 0.5% (plausible), the estimate would be 1000K US deaths, which is pretty damn close to Wharton's 950K estimate in their model with limited controls/distancing.
https://rutgers.forums.rivals.com/t...social-distancing.191275/page-94#post-4539724
The only other hope we have to not hit the modeled numbers of deaths in the next 2 months is if we have a bona fide cure (or close to it) in place in the next month or so. We all better hope convalescent plasma is as good as the anecdotal reports are indicating, since that can help now, whereas even the engineered antibodies, which could be available by late summer, will be too late to prevent many of these deaths, and a vaccine is at least several more months beyond late summer.
NY's regional plan for reopening discussed in Cuomo's press conference, yesterday (very long)
Thought their team did a great job of outlining the specifics of NY essentially trying to mimic South Korea's model for controlling outbreaks, i.e., aggressive testing, tracing, and isolating, combined with a mask-wearing culture and appropriate social distancing (with controls where that's not possible) and that Cuomo did a masterful job of presenting all the data/info - great leadership and understanding. I also liked that he made it clear that "I don't know" is ok to say and is, in fact, required when one doesn't know and there are many things we still don't know, but we prepare as best we can with what we do know. I included graphics from the presser below, too, as they're probably easier to read.
Requirements for Reopening in each region
- Regions must have at least 14 days of decline in total hospitalizations and deaths on a 3-day rolling average.
- In regions with few COVID cases, it cannot exceed 15 new total cases or 5 new deaths on a 3-day rolling average.
- In order to monitor the potential spread of infection in the region, a region must have fewer than two new COVID patients admitted per 100k residents per day.
- NY must make sure every region has the capacity to handle a potential surge in cases: Regions must have at least 30% total hospital and ICU beds available.
- This is coupled with the new requirement that hospitals have at least 90 days of PPE stockpile.
- As far as testing for viral infections, NY will follow the CDC guidance of having the capacity to perform 30 tests for every 1,000 residents in a region.
- Regions must have a baseline of 30 contact tracers for every 100,000 residents and additional tracers based on the projected number of cases in the region.
- NY is building an army of tracers in partnership with Mayor Bloomberg (head and financial sponsor of the task force on tracing), to meet statewide needs.
Cuomo said that businesses that are most essential and pose the lowest risk will be the first to open, with less essential and riskier businesses opening later, as per the phases below. He also said that each phase will be followed by a pause to reassess whether flare-ups/outbreaks were being observed and, if so, controlled before moving to the next phase, so that an outbreak doesn't get way ahead of the response as occurred in the initial wave, obviously. And noted that businesses are going to need to reassess and reimagine the workplace with regard to people, places/facilities, and processes/procedures. I know where I work, every aspect of work has been reorganized to reduce COVID risks.
- Phase 1: Manufacturing, construction, curbside pickup etc.
- Phase 2: Professional services, retail, real estate
- Phase 3: Restaurants, food services etc.
- Phase 4: Arts, sports, education.
Slides from Press Conference










A few words on projected deaths/calcs
One more thought for skeptics. Unless NY is somehow "different" and I doubt it is, apart from the rate of deaths being greater due to the far greater undetected infection rates in late Feb/March that we simply didn't know about due to lack of testing (meaning it might take NY 6 months to reach herd immunity and a rural area 2 years, due to population density differences, which slow transmission rates, but the eventual endpoints should be the same, barring a cure/vaccine. .
But we know a ton more than we did before, so death calcs are not nearly as dependent on models any more, especially since we now know reasonably well the current infection fatality ratio, at least for a decent population (NY state), which has statewide antibody testing results. NY had about 23,000 deaths late last week while they were doing the antibody testing, which showed 12.3% infected (2.46MM infected with antibodies), which is an IFR of 0.9%. While the error bars on the IFR are moderately high, due to the errors on the antibody testing (denominator), I don't think we're going to find out we have 50% infected instead of 12.3% (would be fantastic if we did, though).
So if we take the 12.3% as correct and assume we have another 30-60% of NY left to infect to reach 42% to 72% infected (to come close to herd immunity of 54-82% - should slow down greatly near the herd immunity level - the range most think is herd immunity, depending on the transmission rate, which is still not known for sure; 54% is if R0 is 2.2 and 82% is if R0 is 5.7), that would mean another 30/12.3 x 23K or 56K deaths to go on the low side and another 60/12.3 x 23K or 112K deaths to go on the high side (in addition to the 23K dead).
The same calculation for the US, assuming a prevalence of 3% in the US (1/4 of NY - a guess based on cases, roughly), means probably 15-25X as many deaths as we've seen to date or 1.05-1.75MM total US deaths at herd immunity (depending on what that level is) and at an IFR of 0.9%. Perhaps NY's IFR truly is a bit higher than other areas for reasons I don't know yet (demographics? hospitals stressed?), but even if the US's IFR were only 0.5%, that's 580-970K US deaths. The Wharton model is predicting 950K US deaths eventually, assuming current death rates and no controls/distancing and no cure/vaccine before herd immunity is reached.
I still believe convalescent plasma is going to save many lives in the next few months and then the engineered antibodies will save a lot more and I think we'll have a vaccine by the end of the year, but the path that Cuomo outlined, following South Korea's model, is what we need to do until we have a cure/vaccine, IMO. Flattening the curve isn't just about not overwhelming hospitals - it's also about buying time to develop cures/vaccines, so hundreds of thousands of lives can be saved, hopefully while reopening most of the economy (but in new ways).
Last edited:
Too long, not reading. Post cliff notes.NY's regional plan for reopening discussed in Cuomo's press conference, yesterday (very long)
Thought their team did a great job of outlining the specifics of NY essentially trying to mimic South Korea's model for controlling outbreaks, i.e., aggressive testing, tracing, and isolating, combined with a mask-wearing culture and appropriate social distancing (with controls where that's not possible) and that Cuomo did a masterful job of presenting all the data/info - great leadership and understanding. I also liked that he made it clear that "I don't know" is ok to say and is, in fact, required when one doesn't know and there are many things we still don't know, but we prepare as best we can with what we do know. I included graphics from the presser below, too, as they're probably easier to read.
Requirements for Reopening in each region
Phased Reopening Plan
- Regions must have at least 14 days of decline in total hospitalizations and deaths on a 3-day rolling average.
- In regions with few COVID cases, it cannot exceed 15 new total cases or 5 new deaths on a 3-day rolling average.
- In order to monitor the potential spread of infection in the region, a region must have fewer than two new COVID patients admitted per 100k residents per day.
- NY must make sure every region has the capacity to handle a potential surge in cases: Regions must have at least 30% total hospital and ICU beds available.
- This is coupled with the new requirement that hospitals have at least 90 days of PPE stockpile.
- As far as testing for viral infections, NY will follow the CDC guidance of having the capacity to perform 30 tests for every 1,000 residents in a region.
- Regions must have a baseline of 30 contact tracers for every 100,000 residents and additional tracers based on the projected number of cases in the region.
- NY is building an army of tracers in partnership with Mayor Bloomberg (head and financial sponsor of the task force on tracing), to meet statewide needs.
Cuomo said that businesses that are most essential and pose the lowest risk will be the first to open, with less essential and riskier businesses opening later, as per the phases below. He also said that each phase will be followed by a pause to reassess whether flare-ups/outbreaks were being observed and, if so, controlled before moving to the next phase, so that an outbreak doesn't get way ahead of the response as occurred in the initial wave, obviously. And noted that businesses are going to need to reassess and reimagine the workplace with regard to people, places/facilities, and processes/procedures. I know where I work, every aspect of work has been reorganized to reduce COVID risks.
Cuomo also addressed the fact that NY Pause ends on May 15. "May 15th, regions can start to reopen and do their own analysis, but these are the facts that they have to have in place to do it. Start now. Don't wait until May 15th. Don't call me up on May 15th, and say, well, the pause order expired. I want to open. Because I'm going to ask you the questions I just asked." And he also mentioned that the Governors in the NE region working with each other (NY/NJ/CT/MA/RI/PA/DE) will also be unveiling similar plans. Given what's at stake in terms of potential deaths, as per the quoted post, including IHME doubling estimated deaths to 134K by August and the Wharton model showing scenarios with up to 950K dead over many months if we stop all interventions/social distancing, let's hope this works.
- Phase 1: Manufacturing, construction, curbside pickup etc.
- Phase 2: Professional services, retail, real estate
- Phase 3: Restaurants, food services etc.
- Phase 4: Arts, sports, education.
Slides from Press Conference
A few words on projected deaths/calcs
One more thought for skeptics. Unless NY is somehow "different" and I doubt it is, apart from the rate of deaths being greater due to the far greater undetected infection rates in late Feb/March that we simply didn't know about due to lack of testing (meaning it might take NY 6 months to reach herd immunity and a rural area 2 years, due to population density differences, which slow transmission rates, but the eventual endpoints should be the same, barring a cure/vaccine. .
But we know a ton more than we did before, so death calcs are not nearly as dependent on models any more, especially since we now know reasonably well the current infection fatality ratio, at least for a decent population (NY state), which has statewide antibody testing results. NY had about 23,000 deaths late last week while they were doing the antibody testing, which showed 12.3% infected (2.46MM infected with antibodies), which is an IFR of 0.9%. While the error bars on the IFR are moderately high, due to the errors on the antibody testing (denominator), I don't think we're going to find out we have 50% infected instead of 12.3% (would be fantastic if we did, though).
So if we take the 12.3% as correct and assume we have another 30-60% of NY left to infect to reach 42% to 72% infected (to come close to herd immunity of 54-82% - should slow down greatly near the herd immunity level - the range most think is herd immunity, depending on the transmission rate, which is still not known for sure; 54% is if R0 is 2.2 and 82% is if R0 is 5.7), that would mean another 30/12.3 x 23K or 56K deaths to go on the low side and another 60/12.3 x 23K or 112K deaths to go on the high side (in addition to the 23K dead).
The same calculation for the US, assuming a prevalence of 3% in the US (1/4 of NY - a guess based on cases, roughly), means probably 15-25X as many deaths as we've seen to date or 1.05-1.75MM total US deaths at herd immunity (depending on what that level is) and at an IFR of 0.9%. Perhaps NY's IFR truly is a bit higher than other areas for reasons I don't know yet (demographics? hospitals stressed?), but even if the US's IFR were only 0.5%, that's 580-970MM US deaths. The Wharton model is predicting 950K US deaths eventually, assuming current death rates and no controls/distancing and no cure/vaccine before herd immunity is reached.
I still believe convalescent plasma is going to save many lives in the next few months and then the engineered antibodies will save a lot more and I think we'll have a vaccine by the end of the year, but the path that Cuomo outlined, following South Korea's model, is what we need to do until we have a cure/vaccine, IMO. Flattening the curve isn't just about not overwhelming hospitals - it's also about buying time to develop cures/vaccines, so hundreds of thousands of lives can be saved, hopefully while reopening most of the economy (but in new ways).
Mask until told otherwise.Too long, not reading. Post cliff notes.
Thank you. Saved me a lot of time! Thankfully we don't live in NY.Mask until told otherwise.
:ThumbsUp
Too long, not reading. Post cliff notes.
Drink bleach, stick that tanning bulb up your ass. You'll be fine. Like magic.
You forgot the squeeze tight step after said insertion.Drink bleach, stick that tanning bulb up your ass. You'll be fine. Like magic.
Drink bleach, stick that tanning bulb up your ass. You'll be fine. Like magic.
Doesn’t even have to be a tanning bulb, I believe a tremendous light will suffice.
I bet this response went over well when you were mayor...Too long, not reading. Post cliff notes.
Never was so long winded, don't like wasting time. I remember the relief effort for Sandy that I led, all perfect and concise info. Wow, that was a hell of an experience.I bet this response went over well when you were mayor...
Last edited:
Latest preprint paper and Twitter posts from Florian Krammer, one of the leads from Mt. Sinai on antibodies, testing and convalescent plasma - this paper was on assessing hundreds of plasma donation volunteers for antibodies. The Twitter feed is much easier to understand than the paper, actually.
https://twitter.com/florian_krammer...om/florian_krammer/status/1257828922638700546
https://www.medrxiv.org/content/10.1101/2020.04.30.20085613v1.full.pdf
Was interesting to see so many (62%) who thought they had COVID but didn't based on antibody assays, while almost everyone who had a positive PCR viral test (565 of 568) had at least some antibodies. Like he said, still need to confirm that antibodies means immunity, but goddamn it, it should and we need the break (sorry, I know science doesn't work that way, but this crap can get to you after awhile).

Another interesting observation was that many patients with antibodies still show residual virus by the PCR test, even up to 28 days after symptoms have ended, but they think this is simply genetic material and not viable virus (the test can't differentiate to that level), so they don't think these people are contagious at all. This also shows how the South Korean researchers could easily be fooled into thinking some people were reinfected, when they were not, seeing positive PCR viral tests after recovery.

Wish he'd post something on how convalescent plasma is going...
https://twitter.com/florian_krammer...om/florian_krammer/status/1257828922638700546
https://www.medrxiv.org/content/10.1101/2020.04.30.20085613v1.full.pdf
Was interesting to see so many (62%) who thought they had COVID but didn't based on antibody assays, while almost everyone who had a positive PCR viral test (565 of 568) had at least some antibodies. Like he said, still need to confirm that antibodies means immunity, but goddamn it, it should and we need the break (sorry, I know science doesn't work that way, but this crap can get to you after awhile).
Another interesting observation was that many patients with antibodies still show residual virus by the PCR test, even up to 28 days after symptoms have ended, but they think this is simply genetic material and not viable virus (the test can't differentiate to that level), so they don't think these people are contagious at all. This also shows how the South Korean researchers could easily be fooled into thinking some people were reinfected, when they were not, seeing positive PCR viral tests after recovery.
Wish he'd post something on how convalescent plasma is going...
T2Kplus10 was a mayor? That’s a scary thought.
90% of his posts are shtick, intended to troll people (although once in awhile I'm just not sure it's all schtick). He's nowhere near as moronic as he appears, but for reasons that elude me, he enjoys this persona on line.
Another retrospective study preprint article (meaning a decent sized grain of salt is required), this time on immunocompromised patients, suggesting they have less incidence of severe ARDS (acute respiratory distress syndrome), potentially related to not having the "cytokine storm" over-response of the immune system. @LETSGORU91
https://www.researchsquare.com/article/rs-27095/v1
https://www.researchsquare.com/article/rs-27095/v1
Let's open up. Food for thought who don't mind this, being told what to do, not working collecting $600 a week plus another $600 a week bonus , plus a 1200 stimulus check, 3 months from now when you have to find a job and there are 1,000 other people applying for it you may just rethink your thinking.
They draw a vile from your arm. I read an article that said drawing blood from a vein will give a far more accurate test than the finger prick. Note that Quest does not offer testing to see if one is actively infected so people needing testing for the virus are not going to Quest.Finger prick or do they draw a vial from your arm?
- Status
- Not open for further replies.
Similar threads
- Replies
- 93
- Views
- 2K
- Replies
- 8
- Views
- 896
- Replies
- 7
- Views
- 594
- Replies
- 0
- Views
- 669
ADVERTISEMENT
ADVERTISEMENT