Because unless they're N95 or higher, they're not meant to protect the wearer. Masks are designed to different standards depending on what it is you need to filter out of the air. The non-N95 surgical or fabric masks aren't fine enough to filter out tiny viruses.
Much like a Brita filter, or even an outdoor water filter built for cysts and bacteria, does not work against viruses.
The surgical/fabric masks prevent the wearer from spewing coronavirus out when coughing, sneezing, wheezing, etc. They are not a controversial topic given that surgeons wear them every day for the same reason of keeping their germs in and some Drs offices (mine) encourage people to wear them when they come in during flu season.
The "numbers are still going up" is just an anecdotal talking point. Masks were never claimed to stop the virus, and numbers are going up for many reasons.
actually that's not exactly how the physics of face masks works... more complicated than a water filter.
the same physics that applies to n95 also applies to non n95 masks of reasonable quality as explained below:
Virus particles don’t exist alone
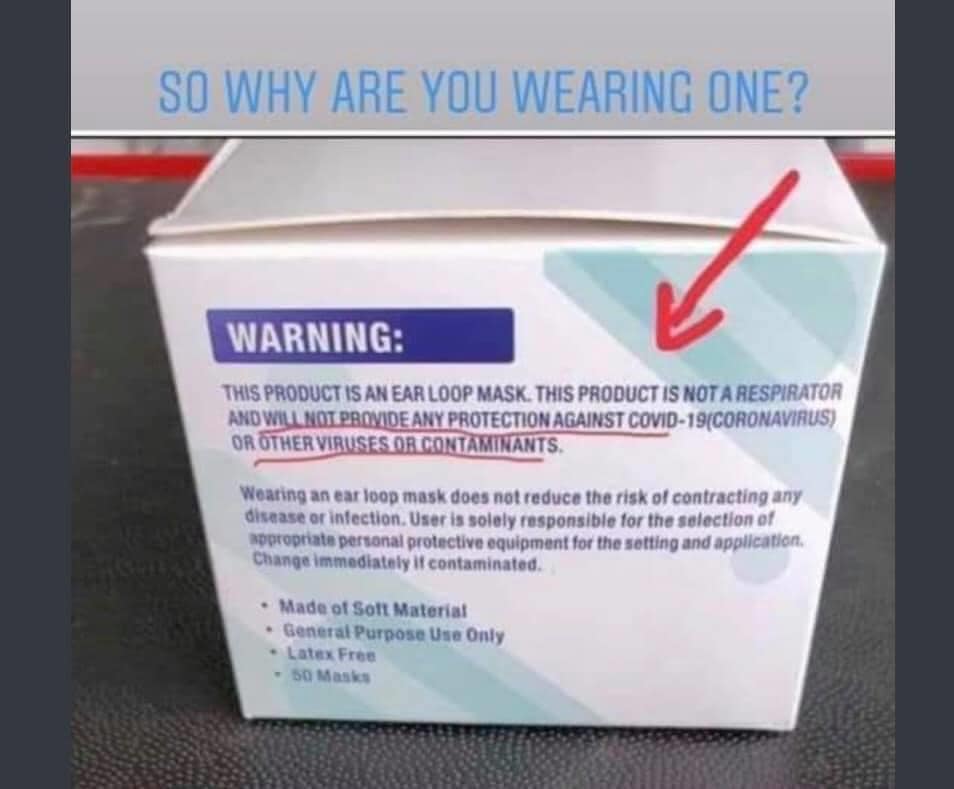
The science of mask functionality gets really small, really fast. The unit of measurement here is microns — 1/1000th of a millimeter.
The size-based argument against N95 laid out in this claim assumes mask filtering works something like water flowing through a net — particles in the water smaller than the net opening pass through, while larger items don’t.
But the physics involved don’t work like that at all.
The COVID-19 particle is indeed around 0.1 microns in size, but it is always bonded to something larger.
“There is never a naked virus floating in the air or released by people,” said Linsey Marr, a professor of civil and environmental engineering at Virginia Tech who specializes in airborne transmission of viruses.
N95 mask on table in front of medical worker
N95 mask on table in front of medical worker
GETTY IMAGES
The virus attaches to water droplets or aerosols (i.e. really small droplets) that are generated by breathing, talking, coughing, etc. These consist of water, mucus protein and other biological material and are all larger than 1 micron.
“Breathing and talking generate particles around 1 micron in size, which will be collected by N95 respirator filters with very high efficiency,” said Lisa Brosseau, a retired professor of environmental and occupational health sciences who spent her career researching respiratory protection.
Health care precautions for COVID-19 are built around stopping the droplets, since “there’s not a lot of evidence for aerosol spread of COVID-19,” said Patrick Remington, a former CDC epidemiologist and director of the Preventive Medicine Residency Program at the University of Wisconsin-Madison.
Fact check: What's true and what's false about coronavirus?
Size matters, but not how you think
But that’s not the only logical flaw in this claim.
The N95 filter indeed is physically around the 0.3 micron size. But that doesn’t mean it can only stop particles larger than that. The masks are actually best for particles either larger or smaller than that 0.3 micron threshold.
“N95 have the worst filtration efficiency for particles around 0.3,” Marr said. “If you’re smaller than that those are actually collected even better. It’s counterintuitive because masks do not work like sieving out larger particles. It’s not like pasta in a colander, and small ones don’t get through.”
N95 masks actually have that name because they are 95% efficient at stopping particles in their least efficient particle size range — in this case those around 0.3 microns.
Why do they work better for smaller ones? There are a number of factors at play, but here are two main ones noted by experts:
The first is something called “Brownian motion,” the name given to a physical phenomenon in which particles smaller than 0.3 microns move in an erratic, zig-zagging kind of motion. This motion greatly increases the chance they will be snared by the mask fibers.
Secondly, the N95 mask itself uses electrostatic absorption, meaning particles are drawn to the fiber and trapped, instead of just passing through.
“Although these particles are smaller than the pores, they can be pulled over by the charged fibers and get stuck,” said Professor Jiaxing Huang, a materials scientist at Northwestern University working to develop a new type of medical face mask. “When the charges are dissipated during usage or storage, the capability of stopping virus-sized particles diminishes. This is the main reason of not recommending the reuse of N95 masks.”
The COVID-19 virus itself is indeed smaller than the N95 filter size, but the virus always travels attached to larger particles that are consistently snared by the filter. And even if the particles were smaller than the N95 filter size, the erratic motion of particles that size and the electrostatic attraction generated by the mask means they would be consistently caught as well