
Colleges
- American Athletic
- Atlantic Coast
- Big 12
- Big East
- Big Ten
- Colonial
- Conference USA
- Independents (FBS)
- Junior College
- Mountain West
- Northeast
- Pac-12
- Patriot League
- Pioneer League
- Southeastern
- Sun Belt
- Army
- Charlotte
- East Carolina
- Florida Atlantic
- Memphis
- Navy
- North Texas
- Rice
- South Florida
- Temple
- Tulane
- Tulsa
- UAB
- UTSA
- Boston College
- California
- Clemson
- Duke
- Florida State
- Georgia Tech
- Louisville
- Miami (FL)
- North Carolina
- North Carolina State
- Pittsburgh
- Southern Methodist
- Stanford
- Syracuse
- Virginia
- Virginia Tech
- Wake Forest
- Arizona
- Arizona State
- Baylor
- Brigham Young
- Cincinnati
- Colorado
- Houston
- Iowa State
- Kansas
- Kansas State
- Oklahoma State
- TCU
- Texas Tech
- UCF
- Utah
- West Virginia
- Illinois
- Indiana
- Iowa
- Maryland
- Michigan
- Michigan State
- Minnesota
- Nebraska
- Northwestern
- Ohio State
- Oregon
- Penn State
- Purdue
- Rutgers
- UCLA
- USC
- Washington
- Wisconsin
High Schools
- Illinois HS Sports
- Indiana HS Sports
- Iowa HS Sports
- Kansas HS Sports
- Michigan HS Sports
- Minnesota HS Sports
- Missouri HS Sports
- Nebraska HS Sports
- Oklahoma HS Sports
- Texas HS Hoops
- Texas HS Sports
- Wisconsin HS Sports
- Cincinnati HS Sports
- Delaware
- Maryland HS Sports
- New Jersey HS Hoops
- New Jersey HS Sports
- NYC HS Hoops
- Ohio HS Sports
- Pennsylvania HS Sports
- Virginia HS Sports
- West Virginia HS Sports
ADVERTISEMENT
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
COVID-19 Pandemic: Transmissions, Deaths, Treatments, Vaccines, Interventions and More...
- Thread starter RU848789
- Start date
- Status
- Not open for further replies.
No further comment needed. Simply indefensible and nobody corrected him. Birx and Fauci must be out of their minds on this one. He really needs to stop talking about anything scientific. And no, this is not a political post.
https://thehill.com/homenews/corona...ght-heat-as-coronavirus-treatment?jwsource=cl
https://thehill.com/homenews/corona...ght-heat-as-coronavirus-treatment?jwsource=cl

Eh, what does Taiwan know? If they really had something important to offer the WHO would be working with them.Similarly, Taiwan ramped up mask production early on and distributed masks to the population, mandating their use in public transit and recommending their use in other public places—a recommendation that has been widely complied with. The country continues to function fully, and their schools have been open since the end of February, while their death total remains very low, at only six.
Go out any day and you will see too many jerseyites out and about mostly at the supermarkets where people used to shop perhaps once per week now it’s 3-4 times a week .They are continuing to go back to multiple stores for items which they want but haven’t been able to get. Wait for the pork OOS which is coming. Also there have been issues with cereals, flour , even vegetables ... too many people with nothing to do go to the only place they can walk around without the fear of being ticketed for being out... supermarkets have become our exercise outlet.Why is social distancing not working in NJ?
No further comment needed. Simply indefensible and nobody corrected him. Birx and Fauci must be out of their minds on this one. He really needs to stop talking about anything scientific. And no, this is not a political post.
https://thehill.com/homenews/corona...ght-heat-as-coronavirus-treatment?jwsource=cl
He probably thinks he’s immune from all his time in a tanning bed.
wow now who is attacking someone... like I said fool I was posting to another on this board about the dialysis question... I won’t grace your taunt about “drive a spike into my brain” ... that is more weird and shows just how f’d up you are to some on this board ... those you see as not agreeing with you are thought of as less but I will say this ... your comment is way too threatening...You're a psycho. Literally nothing you said has anything to do with anything I said. I wasn't addressing you in any way.
Here's a thought - go drive a spike into your brain hole. Let us know if you hit anything.
F*ckin' weirdo.
About 50% on board a packed flight to this area without masks but two in full hazmat suits.
https://nypost.com/2020/04/23/airline-passenger-describes-flight-with-many-not-wearing-masks/amp/
https://nypost.com/2020/04/23/airline-passenger-describes-flight-with-many-not-wearing-masks/amp/
No further comment needed. Simply indefensible and nobody corrected him. Birx and Fauci must be out of their minds on this one. He really needs to stop talking about anything scientific. And no, this is not a political post.
https://thehill.com/homenews/corona...ght-heat-as-coronavirus-treatment?jwsource=cl
[roll]
Summary/commentary for some key World/US data through 4/18.
Some comments on NY/NJ/US and from Cuomo’s 4/19 presser
- The most important number in comparing outbreak severity, IMO, is deaths per 1MM people (cases and hospitalizations are important too, but are subject to much more error). Italy, Spain and Belgium are the highest in the world, in the neighborhood of 400-500 deaths/1MM. The US is in the middle of the pack with ~120 deaths/1MM, although the US is earlier in its outbreak and will likely catch up somewhat.
- While the US, overall, looks better by comparison, if NY were a country it would have the worst outbreak in the world at 900 deaths/1MM, while NJ is in the range of those European countries at ~460 deaths/1MM. Have talked about why this is in other posts and will revisit shortly...
- Excluding NY/NJ, the rest of the US is “only” at 53 deaths per 1MM, which is similar to Germany, the “best” of the populous European countries with 55 deaths/1MM. But that needs to be put in context of what is considered “good” control of the epidemic: South Korea, China, Taiwan, Japan, Singapore and more all have <10 deaths/1MM and were all hit with their first waves before the US and Europe. Most experts believe the differences are primarily due to how much better these countries did with early/aggressive testing, aggressive contact tracing and quarantining, moderate to aggressive social distancing, and establishing a mask culture.
- Of course, there are also many other countries in South/Central America, Africa, and Asia with <10 deaths/1MM, but it’s possible some of that is due to some combo of low population density and much less travel to these locations and perhaps some of it is due to “seasonality” (like flu) where the virus is less virulent in warm/humid climates – will be interesting to see if these locations (especially in the southern hemisphere) start to see increases soon.
- It’s worth noting that Iran is the only country outside of Europe and the US which has >50 deaths/1MM (62) US deaths have roughly plateaued in the 1500-2500/day range for about the past 12 days (with some fluctuations, including a huge fluctuation when NY added 3800 deaths on 4/14 that were presumed due to COVID, but never had a viral test done (most were in hospitals and it was obvious they had COVID, so the tests were skipped); hopefully we’ll see this start to decline in a week or so, as deaths lag cases. NY deaths per day plateaued around 700-800 per day for over a week, but have slowly dropped to about 500/day over the last 4 days. NJ deaths look like they are starting to decline.
- 39.0K, 17.7K and 4.0K 28.5K total deaths, respectively, through 4/18 in the US, NY, and NJ. It’s now looking like my 4/5 guesstimate of 40-50K US deaths in this first wave will be a little low; the U of Washington latest projection is for 60K deaths (they were at 82K on 4/5).
- The Earth hit 2.33MM positive cases on 4/18 with 739K cases in the US, 241K in NY and 81K in NJ.
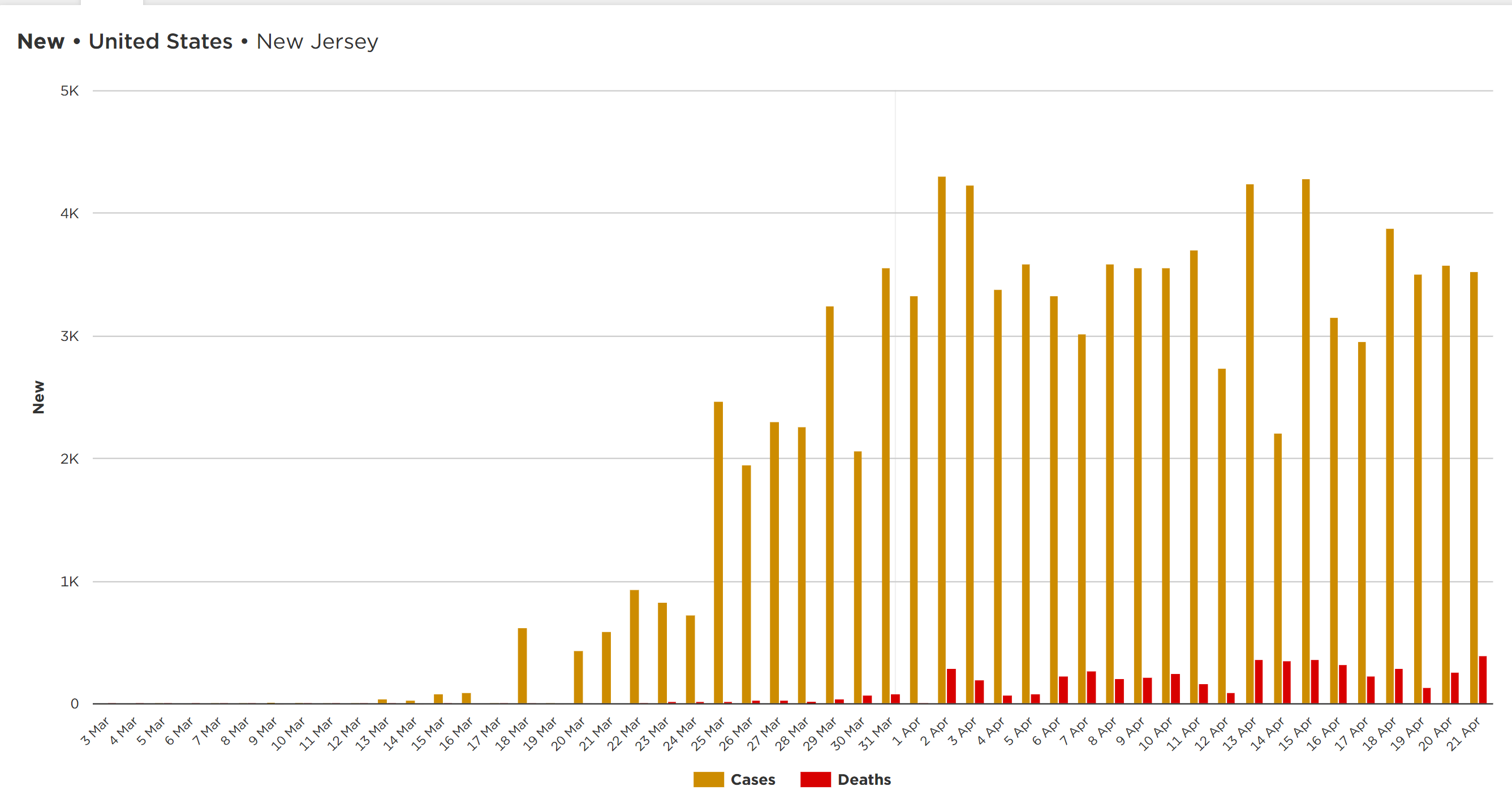
- Both NY and NJ have reached the “peak plateau” in new cases, with some decline starting to occur, especially in NY, which saw its lowest new case number (6K) since 3/25although there have been a few large fluctuations, likely related to testing rates; the US has reached a peak plateau also and has stayed there for about 2 weeks, although it looks like a decline might be starting.
- NY now has done about 30K tests per 1MM in population, which is more than almost any other country; NJ is at 18K tests per 1MM and the US is at 11K tests per 1MM, both of which are middle-of-the-pack (vs. countries with major outbreaks)
- Some very good news: total number of hospitalized in NY has steadily declined from about 19K to 16K over the last 4-5 days.
- As promised, NY is now sending ventilators to other needy states, like Massachusetts, Michigan and Maryland
- Currently three states are showing close to a 10% increase on 4/18 vs. 4/17: Nebraska (13%), Ohio (12.2% and South Dakota 9.3%).
- Cuomo thanked the 1.1MM front line health care workers in NY, as well as the 95K medical staff who voluntarily came to NY simply to help.
- He talked at length on the path back to the “new normal” with the major focus on the need for fast, massive testing for the virus, to know who is sick or getting sick, so they can be quarantined and their contacts traced, as well as massive antibody testing to know who already has had the virus and now likely has immunity, at least for months to maybe years.
- He then announced NY’s ambitious program, starting tomorrow, to test thousands of people from a random, representative sample of the population, to estimate the percentage of people in NY who have had the virus: 1.2% of NY has tested positive by the virus test and there are estimates of 5-15-30% of the general population having been infected (and having antibodies) with most not knowing it. That number greatly impacts how many can go back to work without risks of getting or giving the virus and how much more transmission will occur (with less targets).
- He reiterated the plan for NY/NJ/CT/RI/PA/MA/DE to manage the process of staged “reopenings” for their areas in a regionally coordinated fashion – doesn’t mean “identical” but it will at least be “coordinated.” Also talked about how we should be thinking of how this is an opportunity to improve health care, transportation and education, especially with technology.
- He also reiterated the bipartisan NGA’s (Nat’l Gov’s Assoc) call for $500BB to help state/local budget shortfalls which were not addressed in CARES.






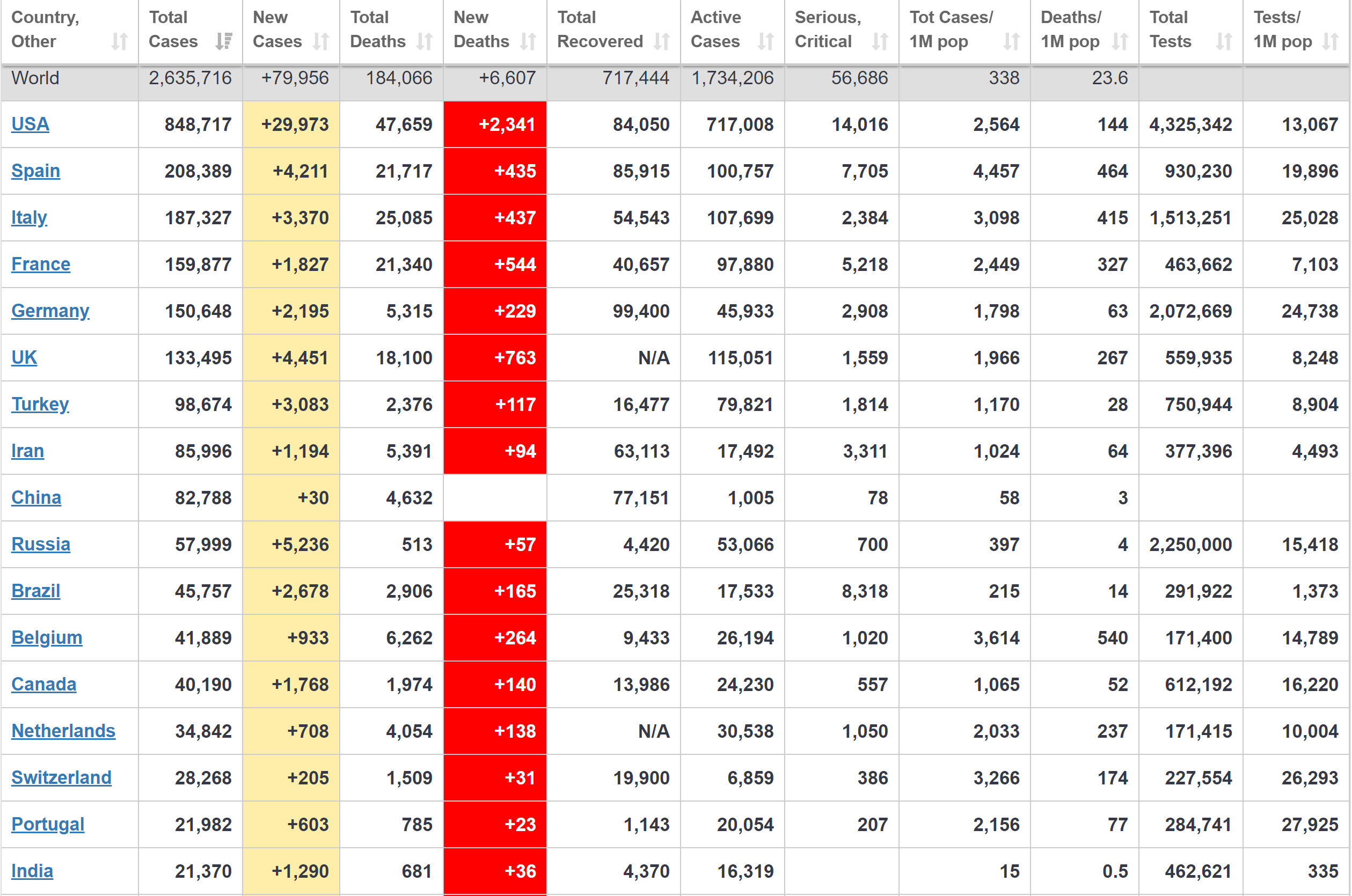
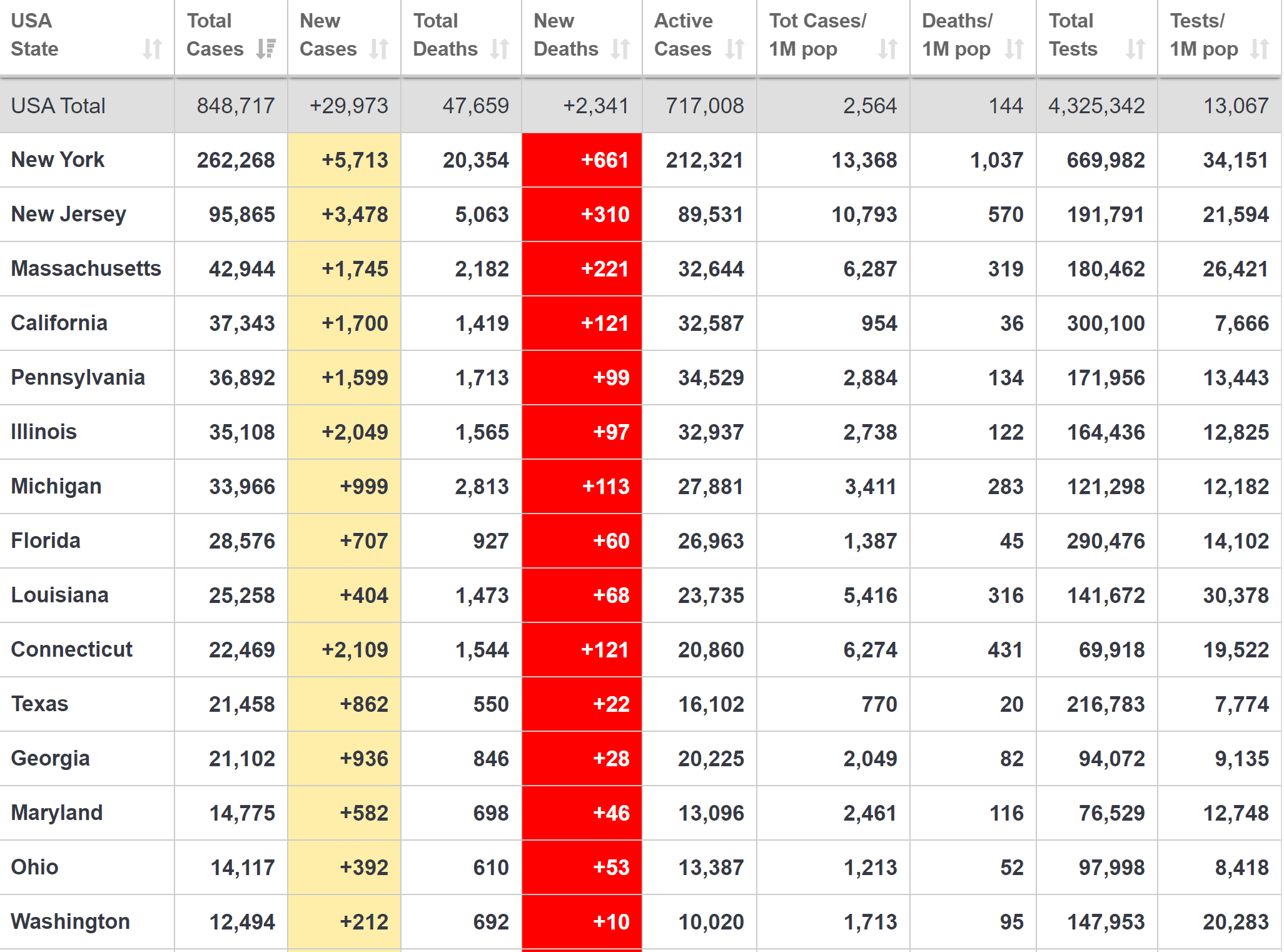
Summary/commentary for some key World/US data through 4/22.
- The most important number in comparing outbreak severity, IMO, is deaths per 1MM people. Italy, Spain and Belgium are the highest in the world, in the neighborhood of 400-500 deaths/1MM, although Belgium is the only one of the major countries reporting “presumed COVID” deaths, which are ~54% of their total. The US is in the middle of the pack with ~144 deaths/1MM, although the US is earlier in its outbreak and will likely catch up somewhat.
- While the US, overall, looks better by comparison, if NY were a country it would have the worst outbreak in the world at 1037 deaths/1MM, while NJ is a little worse than the worst European countries at ~570 deaths/1MM.
- Excluding NY/NJ, the rest of the US is “only” at 74 deaths per 1MM, which is similar to Germany, the “best” of the populous European countries with 63 deaths/1MM. But that needs to be put in context of what is considered “good” control of the epidemic: South Korea, China, Taiwan, Japan, Singapore and more all have <10 deaths/1MM and were all hit with their first waves before the US and Europe. Most believe the differences are primarily due to early/aggressive testing, aggressive contact tracing and quarantining, moderate to aggressive social distancing, and establishing a mask culture.
- The news today from the Northeastern study that NYC likely had 10K cases on 3/1 (with none known and <200 tested through 3/6) means the outbreak was far worse than anyone knew and it’s no surprise that the NYC metro area has gone on to become the worst outbreak in the world, given high density/high commuting density and a very late start on testing and interventions/social distancing (3/16 schools/restaurants/bars closed and 3/22 stay at home orders). In hindsight, the NYC area would have likely needed to lockdown on 3/1 or earlier to have avoided 80-90% of the deaths, once again highlighting why we should have had aggressive early testing to know we had such a bad outbreak.
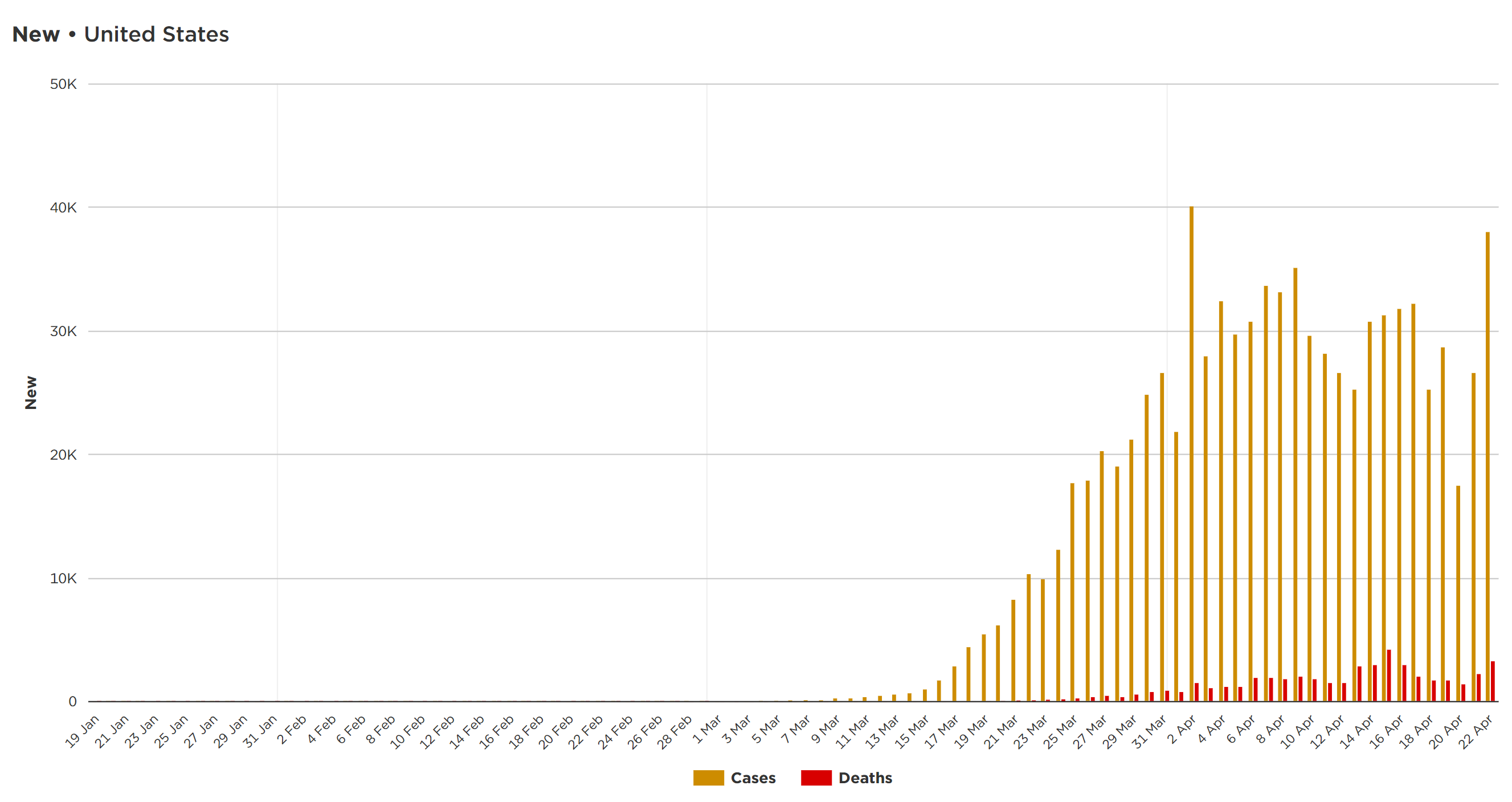
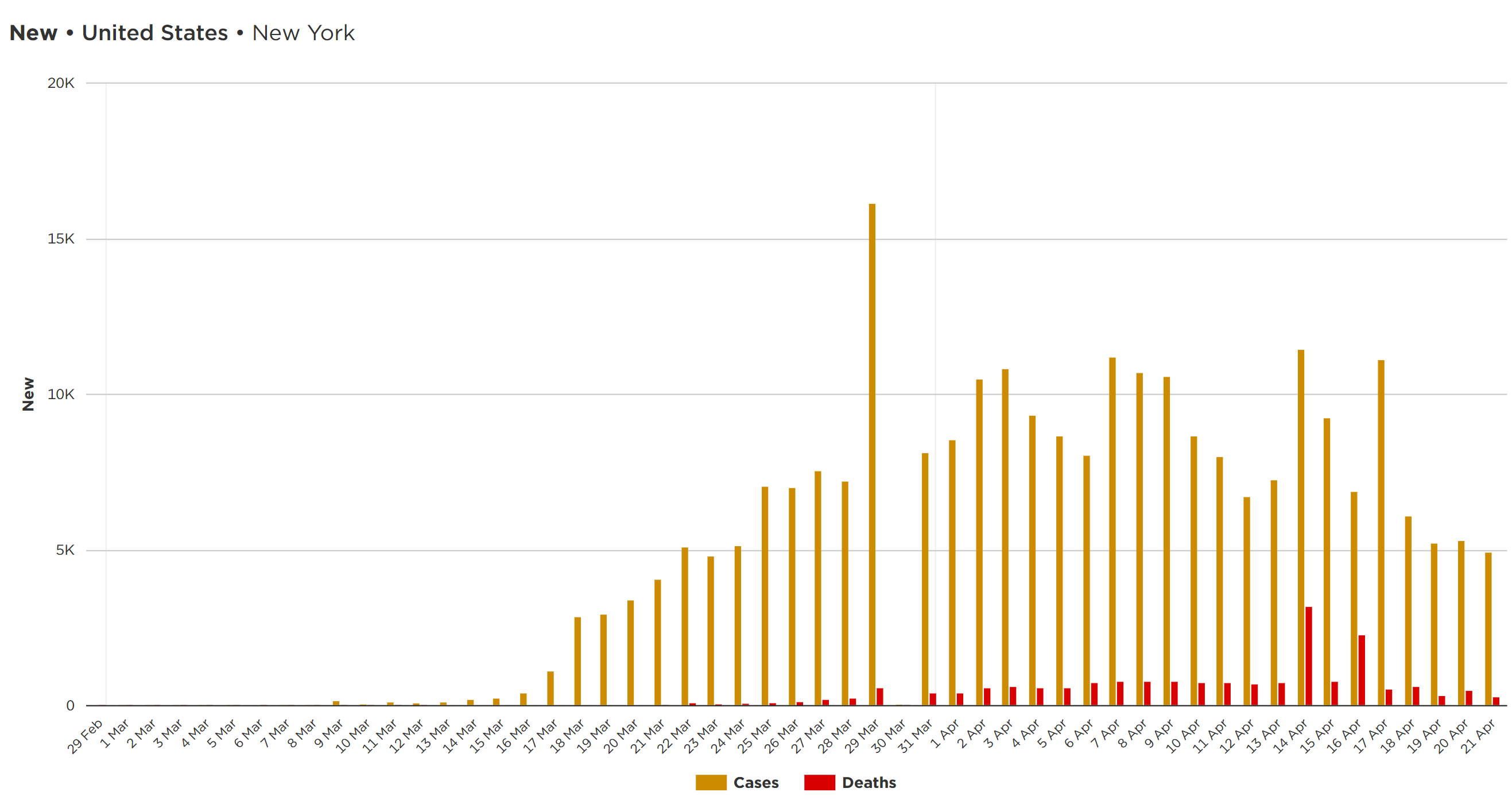
- US deaths have roughly plateaued in the 1500-2500/day range for about the past 12 days (with some fluctuations, including a huge fluctuation when NY added 3800 deaths on 4/14 that were presumed due to COVID, but never had a viral test done (most were in hospitals and it was obvious they had COVID0) and on 4/22 (3300 deaths, but not sure why the jump). Hopefully we’ll see this start to decline in a week or so, as deaths lag cases. NY deaths per day plateaued around 700-800/day for over a week, but declined and have now been 400-500/day over the last 5 days. NJ deaths have fluctuated a fair amount lately, but the moving average shows we’re in a plateau and Gov Murphy said today, that they feel the outbreak is slowing a bit with regard to cases.
- 47.6K, 20.3K and 5.0K total deaths, respectively, through 4/22 in the US, NY, and NJ. The latest U of Washington projection of 66K US deaths might be low at this rate. One oddity though: Worldometer has NY deaths at 20.3K, while Cuomo has NY deaths at 15.5K – NY is still not including the “presumed COVID” (i.e., not tested) deaths.
- The Earth hit 2.63MM cases on 4/18 with 739K cases in the US, 241K in NY and 81K in NJ.
- Both NY and NJ have reached the “peak plateau” in new cases, with some decline in cases definitely occurring in NY, but it’s hard to say that for NJ with so much fluctuation. The big question for NY and eventually NJ is how quickly does the new case rate decline and to what level? Not known now. The US new case rate has been at a plateau for awhile, but has also had some major fluctuations, including yesterday with a huge backlog of tests being reported. It’s why 5-day moving averages are better for trend analyses, but I don’t have those charts.
- NY now has done about 34K tests per 1MM in population, which is more than almost any other country; NJ is at 21K tests per 1MM and the US is at 13K tests per 1MM, both of which are middle-of-the-pack (vs. countries with major outbreaks). As discussed elsewhere, though, it’s not total tests that is critical – it’s testing very aggressively early in an outbreak so that it can be controlled – when that is done, the ratio of positives to tests is low and that never happened in the US or Europe as we feel way behind the oubreak. Fortunately, NY/NYC positives are now down around 25% of total tests from a long plateau in the 40-50% range. NJ test are still up around 50% positive, meaning NJ isn’t testing enough.
- Total number of hospitalized in NY continues to decline steadily.
- As promised, NY is now sending ventilators to other needy states, like Massachusetts, Michigan and Maryland
- Currently, the latest hotspot is Arkansas where new cases jumped nearly 20% yesterday; CT jumped almost 10%.
- He talked at length on the path back to the “new normal”: “Test – Trace – Isolate” is the slogan, with the major focus on the need for fast, massive testing for the virus, to know who is sick or getting sick, so they can be quarantined and their contacts traced, as well as massive antibody testing to know who already has had the virus and now likely has immunity, at least for months to maybe years.
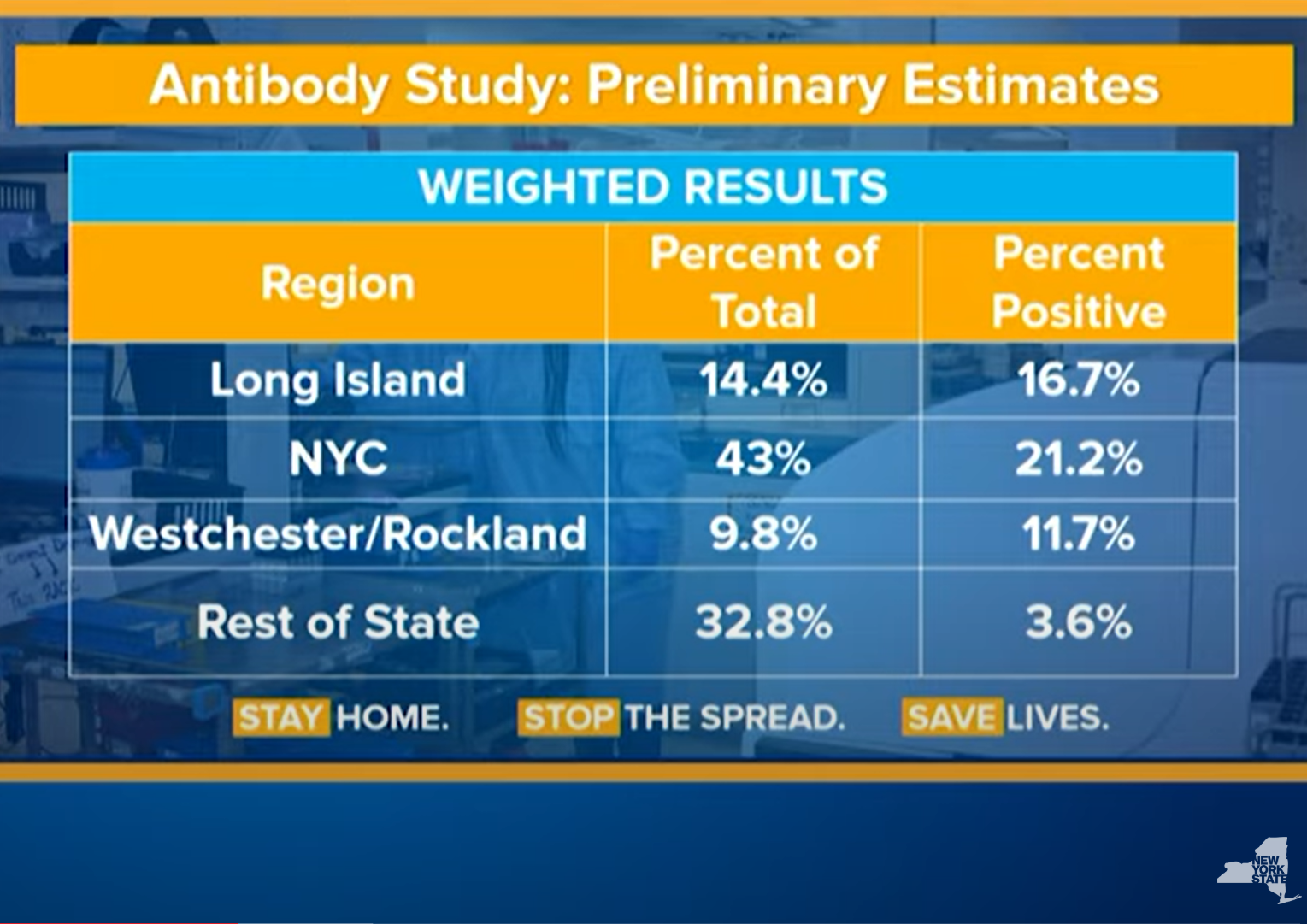
- He also revealed prelimiinary results from their testing of thousands of people from a random, representative sample of the population (3000 so far), to estimate the percentage of people in NY who have had the virus: 1.3% of NY has tested positive by the virus test and preliminary antibody tests show that ~14% of NYers have antibodies, while ~21% of NYC residents have antibodies. Note that these were people who were out and about in stores, so it may be an overestimate. That number greatly impacts how many can go back to work without risks of getting or giving the virus and how much more transmission will occur (with less targets).
- The antibody results also might mean the R0 is very high (5.7 as recently postulated) and that up to 80% of the US/world could become infected if we do nothing, killing hundreds of thousands in the US alone, even if this means the current 7.6% case fatality rate in NY (20K deaths/264K positives) can now finally be translated to an infection fatality rate of 0.7% (20K/2.66MM w/antibodies); if that IFR held and 80% of the US became infected if we did nothing (as we’ve seen in the Ohio prison), that would translate to 330MM x 0.8 x 0.007 = 1.8MM deaths. That’s why we need testing/tracing/isolating and social distancing until we have a proven treatment or vaccine to prevent a calamithy. It’s likely the IFR will continue to decline and the infected % won’t really reach 80%, but even with an IFR of 0.1%, like the flu) and 60% infected, that’s still 200K dead if we do nothing – these were essentially the original arguments for interventions before the outbreak, which way too many downplayed.
- Cuomo rightly slammed Senate Majority Leader McConnell’s frankly heinous statements about not funding states hardest hit by this virus, including funds for health care workers, fire, police, schools, etc., because they’re “blue states.” No words.
I said 20 ft for dramatic effect.
6' would be great, but how possible is it? I go to the grocery store, and as much as I try, I get within 6' of people multiple times per visit.
In one of the recent posts on this thread there is a link which references I think Hong Kong which notes the importance of masks and how they have been able to keep infections so low.
And imo it is obvious via empirical evidence, it sucks to wear the mask because your breath is trapped.
Edit: From previous page,
Hong Kong’s health authorities credit their citizens’ near-universal mask-wearing as a key factor (surveys show almost 100 percent voluntary compliance). Similarly, Taiwan ramped up mask production early on and distributed masks to the population, mandating their use in public transit and recommending their use in other public places—a recommendation that has been widely complied with. The country continues to function fully, and their schools have been open since the end of February, while their death total remains very low, at only six.
Your response does not provide what I asked you for: which is a statement that the mask is more important. All your quote does is say that the mask is important it doesn't say the mask is more important. But I don't wish to debate the point further; it would not be a productive use of time.
I'll answer you: the social distancing is far more important than the masks. The problem is people don't really practice it very well. If you keep more than 6 feet from others (face to face distance) and wash your hands before touching your face after touching any questionable surface, you simply won't catch the virus short of an NBA 3-pointer of a supersneeze. The mask is a backup solution for when people get closer than 6 feet and it's a decent visual reminder to people to not get closer than 6 feet - it's not unimportant, but it's way less important than the preceding. Every epidemiologist and virologist will tell you this.Your response does not provide what I asked you for: which is a statement that the mask is more important. All your quote does is say that the mask is important it doesn't say the mask is more important. But I don't wish to debate the point further; it would not be a productive use of time.
Pretty big news: a Chinese team has shown that rhesus macaques (similar immune system to humans) vaccinated with an "old school" deactivated SARS-CoV-2 virus, were all immune from infection with the virus, even at fairly low vaccine doses. Human trials have just begun with this virus. It's not as "advanced" technology-wise as many of the other vaccines under development, but getting one to work is all that matters and most vaccines on the market are weakened/deactivated viruses. It was only 8 monkeys and there are still many challenges ahead, but this is still pretty big news and a huge step forward. There are 6 other vaccines in early clinical trials and 77 other vaccines under development.
https://www.sciencemag.org/news/202...nkeys-new-coronavirus-chinese-biotech-reports
For the first time, one of the many COVID-19 vaccines in development has protected an animal, rhesus macaques, from infection by the new coronavirus, scientists report. The vaccine, an old-fashioned formulation consisting of a chemically inactivated version of the virus, produced no obvious side effects in the monkeys, and human trials began on 16 April.
Researchers from Sinovac Biotech, a privately held Beijing-based company, gave two different doses of their COVID-19 vaccine to a total of eight rhesus macaque monkeys. Three weeks later, the group introduced SARS-CoV-2, the virus that causes COVID-19, into the monkeys’ lungs through tubes down their tracheas, and none developed a full-blown infection.
“I like it,” says Florian Krammer, a virologist at the Icahn School of Medicine at Mount Sinai who has co-authored a status report about the many different COVID-19 vaccines in development. “This is old school but it might work. What I like most is that many vaccine producers, also in lower–middle-income countries, could make such a vaccine.”
But Douglas Reed of the University of Pittsburgh, who is developing and testing COVID-19 vaccines in monkey studies, says the number of animals was too small to yield statistically significant results. His team also has a manuscript in preparation that raises concerns about the way the Sinovac team grew the stock of novel coronavirus used to challenge the animals: It may have caused changes that make it less reflective of the ones that infect humans.
https://www.sciencemag.org/news/202...nkeys-new-coronavirus-chinese-biotech-reports
For the first time, one of the many COVID-19 vaccines in development has protected an animal, rhesus macaques, from infection by the new coronavirus, scientists report. The vaccine, an old-fashioned formulation consisting of a chemically inactivated version of the virus, produced no obvious side effects in the monkeys, and human trials began on 16 April.
Researchers from Sinovac Biotech, a privately held Beijing-based company, gave two different doses of their COVID-19 vaccine to a total of eight rhesus macaque monkeys. Three weeks later, the group introduced SARS-CoV-2, the virus that causes COVID-19, into the monkeys’ lungs through tubes down their tracheas, and none developed a full-blown infection.
“I like it,” says Florian Krammer, a virologist at the Icahn School of Medicine at Mount Sinai who has co-authored a status report about the many different COVID-19 vaccines in development. “This is old school but it might work. What I like most is that many vaccine producers, also in lower–middle-income countries, could make such a vaccine.”
But Douglas Reed of the University of Pittsburgh, who is developing and testing COVID-19 vaccines in monkey studies, says the number of animals was too small to yield statistically significant results. His team also has a manuscript in preparation that raises concerns about the way the Sinovac team grew the stock of novel coronavirus used to challenge the animals: It may have caused changes that make it less reflective of the ones that infect humans.
More fairly big news. Nice update on convalescent plasma from the CEO of the Mayo Clinic, which is overseeing the national CP program. He said there are close to 300 people now on CP nationwide (there are over 1000 centers who are participating and another 900 or so patients lined up to be treated ASAP) and initial results are "very promising."
https://www.cnbc.com/2020/04/23/fda...olumbia-study-of-plasma-covid-19-therapy.html
They've seen some similar results as the two very small studies done in China (5 and 10 people) with some very ill patients on ventilators recovering. They're also seeing some good results in preventing some patients who are in serious condition, but not on ventilators yet, from getting any worse and also think it could work to even prevent new cases from becoming hospitalized in the first place.
They don't have enough data yet to declare victory, but one can tell by all the comments in the media and on-line by top docs that people are pretty excited about this technology being our first really good treatment for this disease. As for other applications of this technology, there are questions of whether recovered patients all have enough antibodies (and the right ones), as well as what stage the treatment is most effective in and how much is needed, and how long the "immunity" lasts (and more). Have heard we'll hear more definitive info by the end of April...
https://www.cnbc.com/2020/04/23/fda...olumbia-study-of-plasma-covid-19-therapy.html
They've seen some similar results as the two very small studies done in China (5 and 10 people) with some very ill patients on ventilators recovering. They're also seeing some good results in preventing some patients who are in serious condition, but not on ventilators yet, from getting any worse and also think it could work to even prevent new cases from becoming hospitalized in the first place.
They don't have enough data yet to declare victory, but one can tell by all the comments in the media and on-line by top docs that people are pretty excited about this technology being our first really good treatment for this disease. As for other applications of this technology, there are questions of whether recovered patients all have enough antibodies (and the right ones), as well as what stage the treatment is most effective in and how much is needed, and how long the "immunity" lasts (and more). Have heard we'll hear more definitive info by the end of April...
Must have missed this in Cuomo's presser, but great to hear that Mike Bloomberg has agreed to take on leadership (and funding) of a massive regional effort to design and implement a testing, tracing and isolation infrastructure to allow NY, NJ, and CT to reopen with far more confidence in being able to "stamp out" the inevitable flare-ups that will occur. Fantastic news.
https://apicciano.commons.gc.cuny.e...ead-massive-effort-to-test-trace-coronavirus/
During his daily press briefing yesterday, Governor Andrew Cuomo of New York announced that Michael Bloomberg has volunteered to help lead a massive regional effort to test and trace the contacts of people infected with the coronavirus in the tri-state region of New York, New Jersey and Connecticut. The plan announced by Cuomo on Wednesday will be done across city, county and state lines around New York. As reported by NBC News.
“I thank him for taking this on with us,” Cuomo said in a tweet of the former New York City mayor and recent Democratic presidential contender. “It will be expensive, challenging & require an army of tracers. But it must be done.”
Tracing the contacts of people found to be infected with the coronavirus virus is a public health strategy that’s been widely credited for limiting its spread in South Korea.
“Michael Bloomberg will design the program, design the training. He’s going to make a financial contribution also and put together an organization that can help hire the people,” Cuomo said.
“You have weeks to have this up and running, (it’s a) super-ambitious undertaking. And Mayor Bloomberg will help coordinate the entire effort,” Cuomo said. “He’ll be working with the state, I’m working with the city and Nassau and Suffolk (Counties) and Jersey and Connecticut.”
https://apicciano.commons.gc.cuny.e...ead-massive-effort-to-test-trace-coronavirus/
During his daily press briefing yesterday, Governor Andrew Cuomo of New York announced that Michael Bloomberg has volunteered to help lead a massive regional effort to test and trace the contacts of people infected with the coronavirus in the tri-state region of New York, New Jersey and Connecticut. The plan announced by Cuomo on Wednesday will be done across city, county and state lines around New York. As reported by NBC News.
“I thank him for taking this on with us,” Cuomo said in a tweet of the former New York City mayor and recent Democratic presidential contender. “It will be expensive, challenging & require an army of tracers. But it must be done.”
Tracing the contacts of people found to be infected with the coronavirus virus is a public health strategy that’s been widely credited for limiting its spread in South Korea.
“Michael Bloomberg will design the program, design the training. He’s going to make a financial contribution also and put together an organization that can help hire the people,” Cuomo said.
“You have weeks to have this up and running, (it’s a) super-ambitious undertaking. And Mayor Bloomberg will help coordinate the entire effort,” Cuomo said. “He’ll be working with the state, I’m working with the city and Nassau and Suffolk (Counties) and Jersey and Connecticut.”
Go out any day and you will see too many jerseyites out and about mostly at the supermarkets where people used to shop perhaps once per week now it’s 3-4 times a week .They are continuing to go back to multiple stores for items which they want but haven’t been able to get.
Pure, unadulterated bullshit. It's quite the opposite.
Please don't post anymore. Your perception of reality is inconsistent with actual reality.
The problem is the impracticality of it. In rural areas sure, not that big of a deal, in NYC, it's just not going to happen, unless you shut down the economy, which as we know has some adverse effects.I'll answer you: the social distancing is far more important than the masks. The problem is people don't really practice it very well. If you keep more than 6 feet from others (face to face distance) and wash your hands before touching your face after touching any questionable surface, you simply won't catch the virus short of an NBA 3-pointer of a supersneeze. The mask is a backup solution for when people get closer than 6 feet and it's a decent visual reminder to people to not get closer than 6 feet - it's not unimportant, but it's way less important than the preceding. Every epidemiologist and virologist will tell you this.
The super market checkout is the perfect example of why masks are more important.
1)Your distance to the cashier is going to be less then 6 ft.
2)and more importantly, the surfaces. You put your food on the belt the cashier passes it through to another surface, you pick it up and put it in your bag. Not to mention just touching the rails or the credit card machine, or the cash. The mask keeps the virus from being on these surfaces. Social distancing is not an option in these situations.
1)Your distance to the cashier is going to be less then 6 ft.
2)and more importantly, the surfaces. You put your food on the belt the cashier passes it through to another surface, you pick it up and put it in your bag. Not to mention just touching the rails or the credit card machine, or the cash. The mask keeps the virus from being on these surfaces. Social distancing is not an option in these situations.
Good point about surfaces. In addition to reducing breathing or sneezing directly on someone else, a mask also reduces breathing or sneezing directly on surfaces. It also helps reduce touching your mouth or nose and then touching surfaces, further aiding virus spread.The super market checkout is the perfect example of why masks are more important.
1)Your distance to the cashier is going to be less then 6 ft.
2)and more importantly, the surfaces. You put your food on the belt the cashier passes it through to another surface, you pick it up and put it in your bag. Not to mention just touching the rails or the credit card machine, or the cash. The mask keeps the virus from being on these surfaces. Social distancing is not an option in these situations.
Yesterday I was watching a woman walk on the sidewalk with her mask down. When a car came by she put it on and then took it down after it passed. Working outside all day I see more humorous things than a comedy show at the Stress Factory.
So numbers when do realistically think a vaccine will come to market?Pretty big news: a Chinese team has shown that rhesus macaques (similar immune system to humans) vaccinated with an "old school" deactivated SARS-CoV-2 virus, were all immune from infection with the virus, even at fairly low vaccine doses. Human trials have just begun with this virus. It's not as "advanced" technology-wise as many of the other vaccines under development, but getting one to work is all that matters and most vaccines on the market are weakened/deactivated viruses. It was only 8 monkeys and there are still many challenges ahead, but this is still pretty big news and a huge step forward. There are 6 other vaccines in early clinical trials and 77 other vaccines under development.
https://www.sciencemag.org/news/202...nkeys-new-coronavirus-chinese-biotech-reports
For the first time, one of the many COVID-19 vaccines in development has protected an animal, rhesus macaques, from infection by the new coronavirus, scientists report. The vaccine, an old-fashioned formulation consisting of a chemically inactivated version of the virus, produced no obvious side effects in the monkeys, and human trials began on 16 April.
Researchers from Sinovac Biotech, a privately held Beijing-based company, gave two different doses of their COVID-19 vaccine to a total of eight rhesus macaque monkeys. Three weeks later, the group introduced SARS-CoV-2, the virus that causes COVID-19, into the monkeys’ lungs through tubes down their tracheas, and none developed a full-blown infection.
“I like it,” says Florian Krammer, a virologist at the Icahn School of Medicine at Mount Sinai who has co-authored a status report about the many different COVID-19 vaccines in development. “This is old school but it might work. What I like most is that many vaccine producers, also in lower–middle-income countries, could make such a vaccine.”
But Douglas Reed of the University of Pittsburgh, who is developing and testing COVID-19 vaccines in monkey studies, says the number of animals was too small to yield statistically significant results. His team also has a manuscript in preparation that raises concerns about the way the Sinovac team grew the stock of novel coronavirus used to challenge the animals: It may have caused changes that make it less reflective of the ones that infect humans.
I agree masks are important for very crowded areas (or certain jobs), where SD can be impossible, but for those, I'd far rather see people wearing N95 masks to protect both others and themselves. It's sad that we can't figure out how to make enough of them, when we know they're far better for keeping viruses out than cloth/surgical masks. And if people are a little bit creative, they don't need to treat them as "disposable" as they can just rotate 3-4 of them, so that each time they use a mask it has sat for >72 hours, which should be enough to ensure no viable viruses remain.The problem is the impracticality of it. In rural areas sure, not that big of a deal, in NYC, it's just not going to happen, unless you shut down the economy, which as we know has some adverse effects.
Assuming we pursue the "healthy volunteer human challenge" approach (see link) which could cut "many months" off the development/approval timeline (and I can't imagine why we wouldn't pursue it to save potentially hundreds of thousands of lives), I could see a vaccine being ready for at least high risk people (health care workers, elderly, underlying conditions) by Nov/Dec (scaling up production for the world will take many months though). I know that sounds too good to be true, but with dozens of vaccine approaches being evaluated and now knowing that an old school vaccine works in monkeys, which is huge, I think the combined power of the pharma industry will come through.So numbers when do realistically think a vaccine will come to market?
https://rutgers.forums.rivals.com/t...social-distancing.191275/page-79#post-4521358
Last edited:
So numbers when do realistically think a vaccine will come to market?
There are a couple of key dates you need to look at:
- When is a vaccine developed, tested, and approved under Emergency Use Authorization. Best case scenario is late this year. Reasonable expectation is March-May next year. Long time-line is around Sept 2021. Worst case scenario is no viable vaccine is discovered within the next 2 years.
- When will there be enough doses of the vaccine to inoculate the most vulnerable and front-line workers. Probably about 2 months after the vaccine is approved. If the manufacturer is willing to start producing the vaccine at risk, before testing is complete, then you can shorten that time-line by 2-3 months (though obviously the vaccine can't be administered before it is tested and approved).
- When will there be enough doses of the vaccine for a good portion of the general public. Probably about 6 months after the vaccine is approved (again, this can be shortened by about 2-3 months if the manufacturer starts production before testing is complete).
- When will there be enough doses of the vaccine for everyone on the planet. Probably at least a year after the vaccine is approved.
That's an understatement...if I had a loved one in a nursing home I would have removed them by now.
100% agree with that. Unfortunately some of the residents require higher levels of care than many can (or be willing to) provide in the home. Some residents don't have relocation options. And unfortunately, at this time, anyone taking someone out of a nursing home has to factor in that person may very well be infected with the virus. It's a tough call, but being inside inside a nursing home now is a very, very risky proposition.
No further comment needed. Simply indefensible and nobody corrected him. Birx and Fauci must be out of their minds on this one. He really needs to stop talking about anything scientific. And no, this is not a political post.
https://thehill.com/homenews/corona...ght-heat-as-coronavirus-treatment?jwsource=cl
I didn't see this last night. My wife mentioned it this morning. The best would be if the camera was on Fauci and Birx and they both did massive eye rolls as soon as he said it. What's next? Cramming into a microwave for 45 seconds and hitting the defrost cycle?
Good point about surfaces. In addition to reducing breathing or sneezing directly on someone else, a mask also reduces breathing or sneezing directly on surfaces. It also helps reduce touching your mouth or nose and then touching surfaces, further aiding virus spread.
Good points. I made this point well over a month ago when our esteemed leaders failed to realize a face barrier would greatly reduce the potential for transmission of this virus: imagine walking into a crowded, small room with two handfuls of marbles. Lob each handful in separate directions. Marbles who contact anyone, anywhere infect them. Now repeat the same scenario but as soon as you enter the room, there is plexiglass almost completely segregating you from the crowded room. Throw the same handfuls of marbles and almost no one is contacted and therefore not infected. A simple concept that Birx and Fauci punted on. It's kinda like a Chris Ash 4th and short, inside the opponents 40 yard line and he punts. A "WTH!!" type of decision.
The best would be if the camera was on Fauci and Birx and they both did massive eye rolls as soon as he said it.
Assuming we pursue the "healthy volunteer human challenge" approach (see link) which could cut "many months" off the development/approval timeline (and I can't imagine why we wouldn't pursue it to save potentially hundreds of thousands of lives), I could see a vaccine being ready for at least high risk people (health care workers, elderly, underlying conditions) by Nov/Dec (scaling up production for the world will take many months though). I know that sounds too good to be true, but with dozens of vaccine approaches being evaluated and now knowing that an old school vaccine works in monkeys, which is huge, I think the combined power of the pharma industry will come through.
https://rutgers.forums.rivals.com/t...social-distancing.191275/page-79#post-4521358
IMHO, these guys will be first .......
https://www.biospace.com/article/moderna-vaccine-clinical-trial-moves-into-2nd-round-of-dosing/
If that clip is not spliced or altered in any way, it is absolutely priceless! She looked as if she was about to scream and her head was gonna explode like Mt. Vesuvius!!!
If that clip is not spliced or altered in any way, it is absolutely priceless! She looked as if she was about to scream and her head was gonna explode like Mt. Vesuvius!!!
Personally, I don't understand how she didn't just say, "Oh for f*ck's sake..." and walk out.
IMHO, these guys will be first .......
https://www.biospace.com/article/moderna-vaccine-clinical-trial-moves-into-2nd-round-of-dosing/
I think China has a vaccine that just entered Phase II the other week and is currently in the lead. Moderna is close behind though and just got $500mil to help.
Disagree as I said over a month ago...IMHO, these guys will be first .......
https://www.biospace.com/article/moderna-vaccine-clinical-trial-moves-into-2nd-round-of-dosing/
More on people potentially having had coronavirus infections as early as December...
https://www.nytimes.com/2020/04/23/us/coronavirus-early-cases.html
https://www.nytimes.com/2020/04/23/us/coronavirus-early-cases.html
Probably a lot of us have a few n95 type masks around the house. I know I've used them for various projects (woodworking mainly).
I have a few old used ones in my shop too. They are certainly not is a condition that any health care worker would want. With that said, I have been hesitant to wear them out of the house for fear of N95 shaming. You surgical mask over top is a good idea.
Excellent blog entry by Derek Lowe (In the Pipeline) on the major vaccine candidates under development right now, although he acknowledges there are dozens more. Interesting to see J&J's comments about being able to deliver a billion doses if needed. I would imagine the other major vaccine manufacturers, like Merck, GSK, and Sanofi, will also offer up manufacturing capability for an effort like this, even if they don't develop the new vaccines, much like Merck did with the Ebola vaccine several years ago.
https://blogs.sciencemag.org/pipeli...ntrunning-coronavirus-vaccines-as-of-april-23
https://blogs.sciencemag.org/pipeli...ntrunning-coronavirus-vaccines-as-of-april-23
I agree masks are important for very crowded areas (or certain jobs), where SD can be impossible, but for those, I'd far rather see people wearing N95 masks to protect both others and themselves.
Even significantly lower quality masks than an N95 can be quite beneficial.
If you're wearing a mask that has, let's say, only 40% effectiveness against spreading the virus and I'm wearing a mask that has, let's say, only a 20% effectiveness against receiving the virus from others, that would cut in half the probability of you transmitting the virus to me versus neither of us wearing any mask at all.
Last edited:
J&J and Sanofi are leading the way and doing a great job. My former colleague now leads the Sanofi US Vaccine BU. She's bullish on how quickly a product will make it to market.Excellent blog entry by Derek Lowe (In the Pipeline) on the major vaccine candidates under development right now, although he acknowledges there are dozens more. Interesting to see J&J's comments about being able to deliver a billion doses if needed. I would imagine the other major vaccine manufacturers, like Merck, GSK, and Sanofi, will also offer up manufacturing capability for an effort like this, even if they don't develop the new vaccines, much like Merck did with the Ebola vaccine several years ago.
https://blogs.sciencemag.org/pipeli...ntrunning-coronavirus-vaccines-as-of-april-23
From CNBC:
The Food and Drug Administration warned consumers Friday against taking malaria drugs chloroquine and hydroxychloroquine to treat Covid-19 outside a hospital or formal clinical trial setting after “serious” poisoning and deaths were reported.
The agency said it became aware of reports of “serious heart rhythm problems” in patients with the virus who were treated with the malaria drugs, often in combination with antibiotic azithromycin, commonly known as a Z-Pak. It also warned physicians against prescribing the drugs to treat the coronavirus outside of a hospital.
https://www.cnbc.com/2020/04/24/fda...ter-serious-poisoning-and-death-reported.html
The Food and Drug Administration warned consumers Friday against taking malaria drugs chloroquine and hydroxychloroquine to treat Covid-19 outside a hospital or formal clinical trial setting after “serious” poisoning and deaths were reported.
The agency said it became aware of reports of “serious heart rhythm problems” in patients with the virus who were treated with the malaria drugs, often in combination with antibiotic azithromycin, commonly known as a Z-Pak. It also warned physicians against prescribing the drugs to treat the coronavirus outside of a hospital.
https://www.cnbc.com/2020/04/24/fda...ter-serious-poisoning-and-death-reported.html
Unreal.About 50% on board a packed flight to this area without masks but two in full hazmat suits.
https://nypost.com/2020/04/23/airline-passenger-describes-flight-with-many-not-wearing-masks/amp/
https://nypost.com/2020/04/23/airline-passenger-describes-flight-with-many-not-wearing-masks/amp/
Article on a chloroquine study being cut short due to safety concerns.
From CNBC:
Citing a “primary outcome” of death, researchers cut short a study testing anti-malaria drug chloroquine as a potential treatment for Covid-19 after some patients developed irregular heart rates and nearly two dozen of them died after taking doses of the drug daily.
Scientists say the findings, published Friday in the peer-reviewed Journal of the American Medical Association, should prompt some degree of skepticism from the public toward enthusiastic claims about and perhaps “serve to curb the exuberant use” of the drug, which has been touted by President Donald Trump as a potential “game-changer” in the fight against the coronavirus.
https://www.cnbc.com/2020/04/24/cor...roquine-study-short-over-safety-concerns.html
From CNBC:
Citing a “primary outcome” of death, researchers cut short a study testing anti-malaria drug chloroquine as a potential treatment for Covid-19 after some patients developed irregular heart rates and nearly two dozen of them died after taking doses of the drug daily.
Scientists say the findings, published Friday in the peer-reviewed Journal of the American Medical Association, should prompt some degree of skepticism from the public toward enthusiastic claims about and perhaps “serve to curb the exuberant use” of the drug, which has been touted by President Donald Trump as a potential “game-changer” in the fight against the coronavirus.
https://www.cnbc.com/2020/04/24/cor...roquine-study-short-over-safety-concerns.html
- Status
- Not open for further replies.
Similar threads
- Replies
- 93
- Views
- 3K
- Replies
- 8
- Views
- 1K
- Replies
- 7
- Views
- 726
- Replies
- 0
- Views
- 1K
ADVERTISEMENT
ADVERTISEMENT