Probably temp and humidity impacts the virus. Hope so.IMHO, warm weather is a factor in the spread of this disease.

Colleges
- AAC
- ACC
- Big 12
- Big East
- Big Ten
- Pac-12
- SEC
- Atlantic 10
- Conference USA
- Independents
- Junior College
- Mountain West
- Sun Belt
- MAC
- More
- Navy
- UAB
- Tulsa
- UTSA
- Charlotte
- Florida Atlantic
- Temple
- Rice
- East Carolina
- USF
- SMU
- North Texas
- Tulane
- Memphis
- Miami
- Louisville
- Virginia
- Syracuse
- Wake Forest
- Duke
- Boston College
- Virginia Tech
- Georgia Tech
- Pittsburgh
- North Carolina
- North Carolina State
- Clemson
- Florida State
- Cincinnati
- BYU
- Houston
- Iowa State
- Kansas State
- Kansas
- Texas
- Oklahoma State
- TCU
- Texas Tech
- Baylor
- Oklahoma
- UCF
- West Virginia
- Wisconsin
- Penn State
- Ohio State
- Purdue
- Minnesota
- Iowa
- Nebraska
- Illinois
- Indiana
- Rutgers
- Michigan State
- Maryland
- Michigan
- Northwestern
- Arizona State
- Oregon State
- UCLA
- Colorado
- Stanford
- Oregon
- Arizona
- California
- Washington
- USC
- Utah
- Washington State
- Texas A&M
- Auburn
- Mississippi State
- Kentucky
- South Carolina
- Arkansas
- Florida
- Missouri
- Ole Miss
- Alabama
- LSU
- Georgia
- Vanderbilt
- Tennessee
- Louisiana Tech
- New Mexico State
- Middle Tennessee
- Western Kentucky
- UTEP
- Florida International University
High School
- West
- Midwest
- Northeast
- Southeast
- Other
- Alaska
- Arizona
- California
- Colorado
- Nevada
- New Mexico
- Northern California
- Oregon
- Southern California Preps
- Washington
- Edgy Tim
- Indiana
- Kansas
- Nebraska
- Iowa
- Michigan
- Minnesota
- Missouri
- Oklahoma Varsity
- Texas Basketball
- Texas
- Wisconsin
- Delaware
- Maryland
- New Jersey Basketball
- New Jersey
- New York City Basketball
- Ohio
- Pennsylvania
- Greater Cincinnati
- Virginia
- West Virginia Preps
ADVERTISEMENT
Install the app
How to install the app on iOS
Follow along with the video below to see how to install our site as a web app on your home screen.
Note: This feature may not be available in some browsers.
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
COVID-19 Pandemic: Transmissions, Deaths, Treatments, Vaccines, Interventions and More...
- Thread starter RU848789
- Start date
- Status
- Not open for further replies.
IMHO, warm weather is a factor in the spread of this disease.
Sunlight, airflow, I would think would be all helpful.Probably temp and humidity impacts the virus. Hope so.
Conversely a meat packing plant where a bunch of people are working in a stagnant air environment is no good. I imagine they keep it pretty cold in there as well.
This isn’t an opinion, this is a scientific facts.IMHO, warm weather is a factor in the spread of this disease.

If warm weather impacts the virus, why is Brazil seeing exponential growth? Seriously check their charts, they're screwed if they can't get a handle on it. And it's in the mid 80s and humid in the Amazonas region which is the hotspot in their outbreak.
Warm weather could have an effect, but only a relatively minor one, and if other factors, such as density of population, which shows itself in the work place or living conditions, and that outweighs the warm weather effect, then the virus will spread.If warm weather impacts the virus, why is Brazil seeing exponential growth? Seriously check their charts, they're screwed if they can't get a handle on it. And it's in the mid 80s and humid in the Amazonas region which is the hotspot in their outbreak.
I think what being outdoors provides which is so important is the ability to keep distance, but there are certainly situations where you are outdoors where the distance person to person is very minimal.
Edit: and you wonder if Brazil is practicing any level of social distancing, wearing masks, or sanitizing.
Super llamas to the rescue? :Wink:
https://www.nytimes.com/2020/05/06/science/llama-coronavirus-antibodies.html
https://www.nytimes.com/2020/05/06/science/llama-coronavirus-antibodies.html
I think that also depends upon what segment of the population is being affected down there, i.e., is it the indigenous population or those who came in from Europe? The Spanish Flu decimated many Native American groups in our country far worse than those whose ancestors had emigrated here.If warm weather impacts the virus, why is Brazil seeing exponential growth? Seriously check their charts, they're screwed if they can't get a handle on it. And it's in the mid 80s and humid in the Amazonas region which is the hotspot in their outbreak.
Except in Louisiana.IMHO, warm weather is a factor in the spread of this disease.
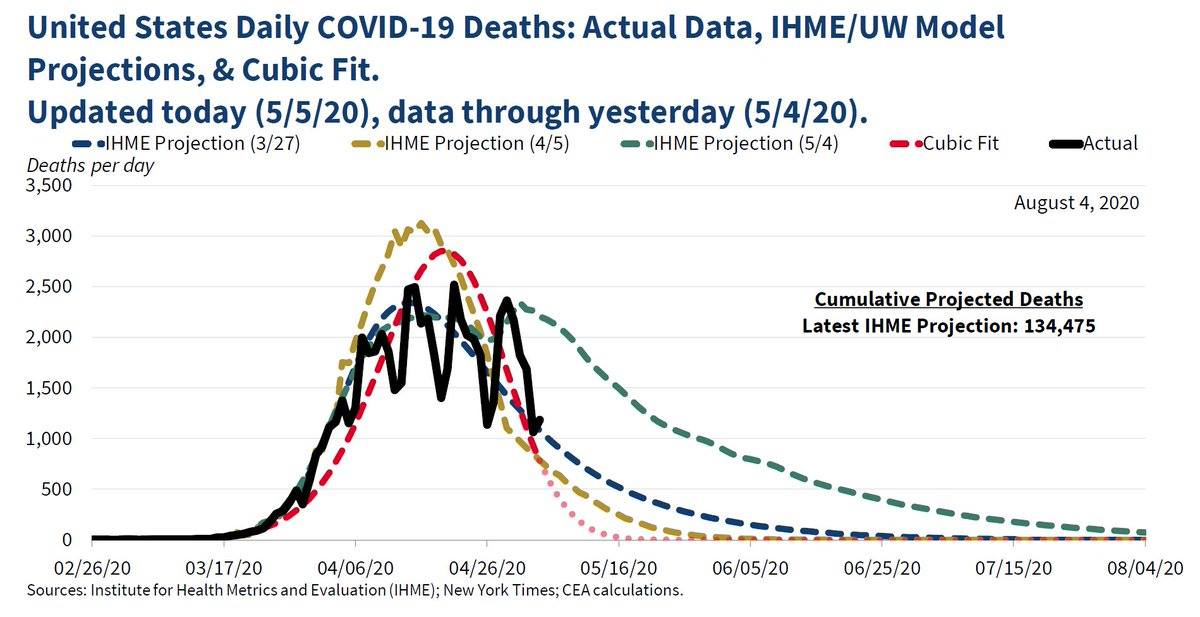
As someone in this Twitter thread said, this tweet from the CEA (White House Council of Economic Advisors) is not going to age well. Notice the "Paint" style graphic of actual deaths that looks a bit like a Sharpie from you-know-who and the decision to put a cubic polynomial function into the mix with actual models as part of someone's idea of how to extrapolate data into the future. This was sent to me from my son who is finishing up his MS at RU in Data Science and he couldn't stop laughing.
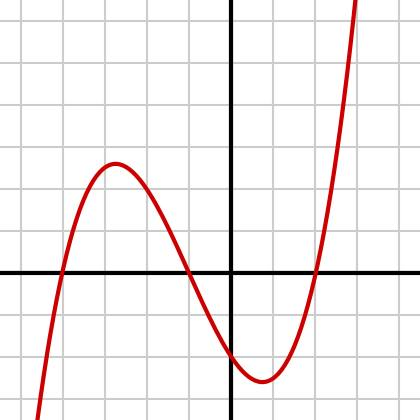
Whoever Sean Taylor is in that Twitter thread nailed it - you simply don't ever use polynomials or any other math function to extrapolate (ok to interpolate) from existing data to future data without a deeper understanding of the process or system being evaluated. Ever. They're trying to use just a small piece of a cubic function to forecast future deaths going to zero - if you look at the standard graphic for a general cubic function, it looks like the graphic below, which would go into "negative deaths" and then go to infinity eventually.
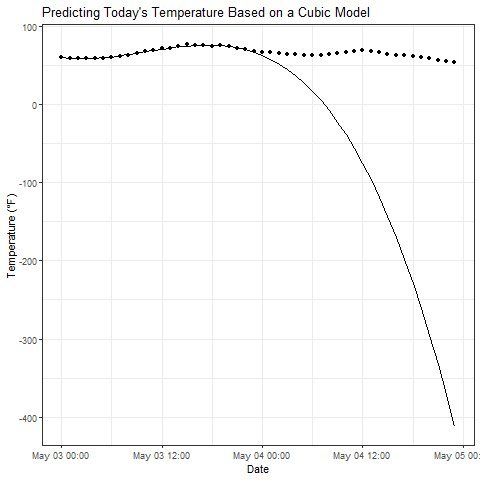
On one level, this is hilarious, but when you realize that these are the people in charge of our country and analyzing when to reopen it, it's sad. This is 9th grade math folks. More embarrassment. First graphic is the CEA tweet, second is a generic cubic polynomial and the third just made me chuckle.
And yet, no one has been more wrong than the Washington model that governments relied on to shut down. It was off by multiples on the most critical point -- hospital capacity and needs.
Cuomo was screaming for weeks on tv about 30,000 ventilators. Then, that just went away with hardly a mention.
This model is no less bad than the others that the officials are apparently relying on.
Nursing homes were a huge driver of indoor spreading of the virus.
The decision by the government in NY to force nursing homes to accept covid infected is one that really takes the cake. Those are the people where quarantine really matters. After Italy's early issues and their old age it is amazing such a thing could happen. The government should have prohibited such people from nursing homes and instead they did the exact opposite.
+1The decision by the government in NY to force nursing homes to accept covid infected is one that really takes the cake. Those are the people where quarantine really matters. After Italy's early issues and their old age it is amazing such a thing could happen. The government should have prohibited such people from nursing homes and instead they did the exact opposite.
Mindbogglingly awful decision. Caused a lot of deaths.
Those are just really tall sheep.:Wink:
Someone said a while ago that a thread will lock/break not based on the # of posts or pages, but the amount of text and characters. There is a limit of shear content a thread can handle.
IMHO, warm weather is a factor in the spread of this disease.
Not so much the warmth more so the UV rays from the abundant sunshine.
THe comparisons to New Orleans that the smart folks are puzzling over is not a true compare - Florida is much further south and sunnier, NO tends to be rainy.
They are not going to ban travel forever ut will make it's way thereThis one's for you @SkilletHead2 - not sure if I've seen you post on this, but New Zealand thinks they have "effectively eliminated" the coronavirus, via a travel ban from China on 2/2, full quarantine of all visitors starting 3/15 (when they only had 6 cases), aggressive early testing/tracing (they're in the top 10% of countries on testing per capita) and a strict lockdown starting 3/25, which is largely over now that new cases are down to zero. The country's 39-year old PM was able to get buy-in on the approach with the help of a team of scientists and health professionals, who are with her every day at their press updates. They've also been truthful with their people that this will require some austerity for awhile and the populace has responded, as they generally trust their government. Hmmm, trust and leadership.
https://www.nationalgeographic.com/...20200505&rid=3F7A7D00850AD922736B3173646A296D
The sudden austerity could have been a cause for panic. But each day, the 39-year-old Ardern, or “Jaz” as she’s popularly known, made clear, concise statements about the situation to the nation, bolstered by a team of scientists and health professionals. A few days after the lockdown, she announced that instead of just slowing the transmission of the virus, New Zealand had set a course of eradicating COVID-19 from its shores, by cutting off the arrival of new cases and choking out existing ones with the restrictions. “We have the opportunity to do something no other country has achieved: elimination of the virus,” said Ardern at one of her daily briefings.
From an outsider’s perspective, the interesting thing about New Zealand is that the country simply got on board. On day one of the lockdown, the streets and highways were empty, the shops were closed, and everyone stayed home. “I think it’s easier for us Kiwis to fall in line because we trust our leaders,” Sue Webster, the owner of the Airbnb where my wife and I holed up for almost four weeks, told me.
https://www.weather-us.com/en/louisiana-usa/new-orleans-climate#uv_indexNot so much the warmth more so the UV rays from the abundant sunshine.
THe comparisons to New Orleans that the smart folks are puzzling over is not a true compare - Florida is much further south and sunnier, NO tends to be rainy.
https://www.weather-us.com/en/florida-usa/orlando-climate#uv_index
THe comparisons to New Orleans that the smart folks are puzzling over is not a true compare - Florida is much further south and sunnier, NO tends to be rainy.
Huh?
New Orleans is at the same latitude as Gainesville. The weather in both places is basically the same.
IMO, they'll ban it until there's a cure (could be in the next few months with plasma/antibodies) or a vaccine, if no cure is found (most say at least 12 months, I say by the end of the year). They can live without tourism - it'll hurt, but they've made the decision that the economic impact is worth not having 0.2-0.5% of their population die. Or at least most of them feel that way. I'll try paging @SkilletHead2 one more time to see his perspective on this from the actual country, since it's possible I have some of this wrong.They are not going to ban travel forever ut will make it's way there
People don't do even the most minimal research before they post...Huh?
New Orleans is at the same latitude as Gainesville. The weather in both places is basically the same.
TruthPeople don't do even the most minimal research before they post...
And yet, no one has been more wrong than the Washington model that governments relied on to shut down. It was off by multiples on the most critical point -- hospital capacity and needs.
Cuomo was screaming for weeks on tv about 30,000 ventilators. Then, that just went away with hardly a mention.
This model is no less bad than the others that the officials are apparently relying on.
You have a lot of this wrong. The IHME/U of Washington model didn't even exist until 3/27, well after almost all shutdown orders were issued by the states and the first version of it predicted 92K dead by June 1st, which will likely be pretty close to what it is. Where they "missed" was not realizing the "tail" of the death curve would likely be prolonged and slow, plus they assumed social distancing would continue until all outbreaks were under control (they assumed we had common sense) - the combination is why the latest model went to 134K deaths by August.
http://www.healthdata.org/covid/updates
The US/White House didn't even issue a projection until 3/31 with their 100-240K projections (where IHME was consulted, but obviously not assumed to be correct).
https://www.nytimes.com/2020/03/31/us/politics/coronavirus-death-toll-united-states.html
And Cuomo and others started talking about hospital capacity/ventilators/PPE in mid-March, well before either of these models came out and I started posting about his pressers around 3/10 and doing daily updates for awhile starting on 3/19. Cuomo did share that they were using a host of different models, but didn't share what they were until a week about 2 weeks later (2nd link below). And the models were usually worst case models if shutdowns and social distancing were ineffective, since they had to plan for the worst case and hope for the best, which is what you do in a highly uncertain, potentially catastrophic scenario.
Also, in case you've forgotten, hospitals in this area did run out of supplies/ventilators at times (we've had docs in this thread and all over the media in NYC saying so) and were barely able to keep up so if the outbreak had been just a bit worse, the outcomes would've likely been far worse. Fortunately, we didn't reach those horrible levels due to fairly effective shutdowns/social distancing - but the graphs (2nd link) show we were likely on the way to reaching those levels.
Actually, IMO, the amazing thing is that even though the cases and deaths significantly exceeded models/expectations for NYC Metro, leading to the hospital systems struggling and buckling at times, the systems never really failed completely anywhere, which is a testament to how well NY/NJ planned ahead for and responded to the onslaught of patients and patient needs. The outbreak here was more than twice as bad as those in Italy/Spain on a cases/deaths per capita basis, yet Italy's health care system completely failed (especially in Northern Italy) and ours did not. I'd call that a very underappreciated success story. @LETSGORU91 @RUfubar - assuming you guys would agree.
https://rutgers.forums.rivals.com/t...social-distancing.191275/page-24#post-4458943
https://rutgers.forums.rivals.com/t...social-distancing.191275/page-61#post-4497445
Thought this was cool: a Canadian team has developed a novel way to possibly treat seriously ill patients: using dialysis to esentially "chemically reprogram" (no details on what exactly that means) overactive white blood cells in patients with hyperimmune responses, associated with the "cytokine storm" inflammation in the lungs and acute respiratory distress/death. They plan to start a small 40-person controlled clinical trial on this shortly.
https://www.eurekalert.org/pub_releases/2020-05/lhri-ctf050620.php
https://www.eurekalert.org/pub_releases/2020-05/lhri-ctf050620.php
The decision by the government in NY to force nursing homes to accept covid infected is one that really takes the cake. Those are the people where quarantine really matters. After Italy's early issues and their old age it is amazing such a thing could happen. The government should have prohibited such people from nursing homes and instead they did the exact opposite.
I'm not sure where you got this from. Would love to see the source material.
My understanding is that any nursing home with a COVID patient simply calls the NYSDOH and the State immediately relocates that person from the nursing home to a hospital.
NYS has been at the forefront of the nursing home issue. They have a daily tally of nursing homes illnesses and deaths and have worked tirelessly to get PPE into these nursing homes.
The problem is that nursing homes operate on razor thin profit margins and PPE goes to hospitals first. It also doesn't help that nursing home employees make very little in comparison to their hospital counterparts.
A cure may not happen....there is no cure for AIDS another SARs disease. there certainly will not be a cure in the next few months. Trials take a year plusIMO, they'll ban it until there's a cure (could be in the next few months with plasma/antibodies) or a vaccine, if no cure is found (most say at least 12 months, I say by the end of the year). They can live without tourism - it'll hurt, but they've made the decision that the economic impact is worth not having 0.2-0.5% of their population die. Or at least most of them feel that way. I'll try paging @SkilletHead2 one more time to see his perspective on this from the actual country, since it's possible I have some of this wrong.
With NJs R-naught effectively frozen at .9 for the last three weeks, cases, hospitalizations, intubations all steadily down for 2 weeks, deaths not dropping as quickly but to be expected on a lag, and back to back days of under 2k new daily cases (first time since 4th week of March)
can someone explain why it is reasonable for Murphy to still not have given any signal on a target date or at least the thresholds he wants to see before starting the phased reopen?
can someone explain why it is reasonable for Murphy to still not have given any signal on a target date or at least the thresholds he wants to see before starting the phased reopen?
Somebody has to pay the bill.With NJs R-naught effectively frozen at .9 for the last three weeks, cases, hospitalizations, intubations all steadily down for 2 weeks, deaths not dropping as quickly but to be expected on a lag, and back to back days of under 2k new daily cases (first time since 4th week of March)
can someone explain why it is reasonable for Murphy to still not have given any signal on a target date or at least the thresholds he wants to see before starting the phased reopen?
A cure may not happen....there is no cure for AIDS another SARs disease
I've been saying cure/treatment and left the treatment part out this time. Plasma-antibodies and engineered antibodies are initially thought of as treatments to prevent serious sickness/deaths for those with COVID, but it's also likely that antibody treatments will provide viral immunity for months or even a year or more without additional treatments, so it could easily become a "functional cure" until a vaccine is available as a true preventative (or herd immunity is reached). I don't think most people care if it's a life-saving treatment or a complete cure right now, as long as there's something to keep people healthy/alive until there's a vaccine.
To me, this is different from the current antiviral cocktails that are now used to treat AIDS patients, which are essentially required for the rest of one's life to stay healthy, so yeah there's no "cure" (complete elimination of the virus) for AIDS. However, there is for Hep C, with the various antivirals that are out now and which eliminate the virus completely after 8-12 weeks of treatment, which is a functional cure to me.
In addition, two weeks ago 2050/5063 deaths were from LTCs. Since that time we are now at 4556/8801 which means over the last few weeks almost 70% (2506 out of 3738) of deaths have been in LTC residents. Our lockdown has minimal impact on LTC facilities. So we have had 1232 deaths outside of LTCs. I would love to see the demographics on that number to see if the majority of them are older than 65 or have obvious co-morbidities.With NJs R-naught effectively frozen at .9 for the last three weeks, cases, hospitalizations, intubations all steadily down for 2 weeks, deaths not dropping as quickly but to be expected on a lag, and back to back days of under 2k new daily cases (first time since 4th week of March)
can someone explain why it is reasonable for Murphy to still not have given any signal on a target date or at least the thresholds he wants to see before starting the phased reopen?
Last edited:
I'm not sure where you got this from. Would love to see the source material.
My understanding is that any nursing home with a COVID patient simply calls the NYSDOH and the State immediately relocates that person from the nursing home to a hospital.
NYS has been at the forefront of the nursing home issue. They have a daily tally of nursing homes illnesses and deaths and have worked tirelessly to get PPE into these nursing homes.
The problem is that nursing homes operate on razor thin profit margins and PPE goes to hospitals first. It also doesn't help that nursing home employees make very little in comparison to their hospital counterparts.
Well, it's been covered by many news outlets. I don't have first hand knowledge other than that.
Here's one:
https://www.nbcnews.com/news/us-new...home-forced-take-recovering-patients-n1191811
Honestly, it is hard to imagine a more dangerous policy. Can you imagine the uproar if the divisive president had done this?
Last edited:
You have a lot of this wrong. The IHME/U of Washington model didn't even exist until 3/27, well after almost all shutdown orders were issued by the states and the first version of it predicted 92K dead by June 1st, which will likely be pretty close to what it is. Where they "missed" was not realizing the "tail" of the death curve would likely be prolonged and slow, plus they assumed social distancing would continue until all outbreaks were under control (they assumed we had common sense) - the combination is why the latest model went to 134K deaths by August.
http://www.healthdata.org/covid/updates
The US/White House didn't even issue a projection until 3/31 with their 100-240K projections (where IHME was consulted, but obviously not assumed to be correct).
https://www.nytimes.com/2020/03/31/us/politics/coronavirus-death-toll-united-states.html
And Cuomo and others started talking about hospital capacity/ventilators/PPE in mid-March, well before either of these models came out and I started posting about his pressers around 3/10 and doing daily updates for awhile starting on 3/19. Cuomo did share that they were using a host of different models, but didn't share what they were until a week about 2 weeks later (2nd link below). And the models were usually worst case models if shutdowns and social distancing were ineffective, since they had to plan for the worst case and hope for the best, which is what you do in a highly uncertain, potentially catastrophic scenario.
Also, in case you've forgotten, hospitals in this area did run out of supplies/ventilators at times (we've had docs in this thread and all over the media in NYC saying so) and were barely able to keep up so if the outbreak had been just a bit worse, the outcomes would've likely been far worse. Fortunately, we didn't reach those horrible levels due to fairly effective shutdowns/social distancing - but the graphs (2nd link) show we were likely on the way to reaching those levels.
Actually, IMO, the amazing thing is that even though the cases and deaths significantly exceeded models/expectations for NYC Metro, leading to the hospital systems struggling and buckling at times, the systems never really failed completely anywhere, which is a testament to how well NY/NJ planned ahead for and responded to the onslaught of patients and patient needs. The outbreak here was more than twice as bad as those in Italy/Spain on a cases/deaths per capita basis, yet Italy's health care system completely failed (especially in Northern Italy) and ours did not. I'd call that a very underappreciated success story. @LETSGORU91 @RUfubar - assuming you guys would agree.
https://rutgers.forums.rivals.com/t...social-distancing.191275/page-24#post-4458943
https://rutgers.forums.rivals.com/t...social-distancing.191275/page-61#post-4497445
Whether it was released or not, it was said to be the model that government was relying on in March. If it wasn't, then maybe part of the problem with the whole response is that the governments, especially at state levels, said "we have models that show X" and then didn't release them. What model ever showed 30,000 ventilators were needed in NY? I know it was the Washington model that stated that hospital capacity would be exceeded in about every state. Outside of some areas in NY/NJ, that never came close to happening.
In NY/NJ, we learned that the hospital system was way better than Italy, just like many predicted despite the apples to oranges incorrect comparisons thrown out that they had more beds than we did.
Those #'s are stunning.In addition, two weeks ago 2050/5063 deaths were from LTCs. Since that time we are now at 4556/8801 which means over the last few weeks almost 70% (2506 out of 3738) of deaths have been in LTC residents. Our lockdown has minimal impact on LTC facilities. So we have had 1232 deaths outside of LTCs. I would love to see the demographics on that number to see if the majority of them are older than 65 or have obvious com-morbidities.
In NJ and NY, whenever a patient was diagnosed with corona, they were just sent back to their LTC facility. The virus is slowing down because it has already ripped through most local facilities.
Alright but there is NO cure. For the record they have no idea if it's gone permanently you are making assumptionsI've been saying cure/treatment and left the treatment part out this time. Plasma-antibodies and engineered antibodies are initially thought of as treatments to prevent serious sickness/deaths for those with COVID, but it's also likely that antibody treatments will provide viral immunity for months or even a year or more without additional treatments, so it could easily become a "functional cure" until a vaccine is available as a true preventative (or herd immunity is reached). I don't think most people care if it's a life-saving treatment or a complete cure right now, as long as there's something to keep people healthy/alive until there's a vaccine.
To me, this is different from the current antiviral cocktails that are now used to treat AIDS patients, which are essentially required for the rest of one's life to stay healthy, so yeah there's no "cure" (complete elimination of the virus) for AIDS. However, there is for Hep C, with the various antalrightivirals that are out now and which eliminate the virus completely after 8-12 weeks of treatment, which is a functional cure to me.
Don't look now, but Florida's numbers are rising, both cases and deaths.Florida #'s looking good as well:
https://experience.arcgis.com/experience/96dd742462124fa0b38ddedb9b25e429
I
Uh, deaths are way down over the last 4 days.Don't look now, but Florida's numbers are rising, both cases and deaths.
I
Just a thought but maybe he wants to see what happens in other states that open up.With NJs R-naught effectively frozen at .9 for the last three weeks, cases, hospitalizations, intubations all steadily down for 2 weeks, deaths not dropping as quickly but to be expected on a lag, and back to back days of under 2k new daily cases (first time since 4th week of March)
can someone explain why it is reasonable for Murphy to still not have given any signal on a target date or at least the thresholds he wants to see before starting the phased reopen?
No, that page has just not put the last couple days in their graph. Intentional?Uh, deaths are way down over the last 4 days.
61 was the last reported death total by Florida(not sure if that is counted for yesterday or today). Back to back 60 death days.
Who said there was a cure?Alright but there is NO cure. For the record they have no idea if it's gone permanently you are making assumptions
- Status
- Not open for further replies.
Similar threads
- Replies
- 0
- Views
- 206
- Replies
- 14
- Views
- 630
- Replies
- 33
- Views
- 941
- Replies
- 17
- Views
- 894
ADVERTISEMENT
ADVERTISEMENT