Probably the best analysis of the situation I've read, medically, epidemiologically, and socially by Tomas Pueyo. Scary as shit, but with serious data analysis (and great graphics for visualization) behind it.
Link not working. Go to medium.com/topic/coronavirus, then click on "Coronavirus, Why We Must Act Now" for the article/data.
He basically says we're in the exponential growth phase and are about to be hammered with actual cases, since the true numbers of people walking around with the coronavirus right now are 10-30X what we've measured so far (a bit over 2000) and the only way to stem the tide once a country has reached this kind of growth rate (especially without testing insight) is lockdown.
And while he's not a medical professional/epidemiologist, he's got an MBA from Stanford and two MS's in eng'g from top European schools and is one of the best data visualization experts out there and numerous other epidemiologists are sending the same message - it's just that he's doing it in a more convincing, data-rich, easy to understand way (see the Times link below for a similar article). So while there are a few weak points in the scientific discussion (he doesn't discuss age and probably overstates some of his mortality rates), the parts about exponential growth and the need for containment (testing. tracking contacts, quarantining infected people, etc.) and mitigation/social distancing are spot on if we want to prevent a bunch of Wuhans/Italys.
https://www.nytimes.com/2020/03/13/science/coronavirus-math-mitigation-distancing.html
We're making strides but we're not in true lockdown yet. In a week, when we have 10,000 cases and hundreds dead, we'll end up in lockdown, but unfortunately it will likely be a lockdown with an overwhelmed health care system, making the mortality rates much higher than they need to be. So why not do it now if you haven't already (and are able to do so) to try to "flatten the curve" so we at least don't overwhelm our medical facilities and health care system?
Below is his intro and in the link are all the graphics and explanations. Hard to read it without saying, damn this guy really knows his science and his data. A few bulleted highlights from the detailed sections:
- Wuhan went exponential and out of control with over a thousand "actual" (but unknown cases when they had only confirmed about 100. We've all heard how bad it got there with their lockdown
- The rest of China learned from Wuhan and every other outbreak was contained with lockdowns that were effective before the exponential growth phase was reached and the lockdown, high testing rate, and largely unaffected medical system made for a much lower mortality rate.
- Hong Kong, Taiwan, Singapore, Japan also never hit the exponential growth phase, as all of them were hit by SARS in 2003, and all of them learned from it. They learned how viral and lethal it could be, so they knew to take it seriously. That’s why all of their graphs, despite starting to grow much earlier, still don’t look like exponentials.
- South Korea is an outlier in many respects. The outbreak was under control until Patient 31, who was a super-spreader who passed it to thousands of other people in Daegu. Because the virus spreads before people show symptoms, by the time the authorities realized the issue, the virus was out there. They’re now paying the consequences of that one instance, but their testing and containment efforts have paid off, as Italy and Iran have caught up to and well surpassed SK, which is now showing a significant decline in new cases.
- Washington State is the US’s Wuhan. The number of cases there is growing exponentially and the virus had been spreading undetected for weeks. If only the CDC had allowed Dr. Chu to test those reserve flu samples in early Feb, instead of Feb 25th, when she found the virus had been spreading for weeks, undetected (when she ran the tests and shared them with the public without permission)
- With the number of cases we see today in countries like the US, Spain, France, Iran, Germany, Japan, Netherlands, Denmark, Sweden or Switzerland, Wuhan was already in lockdown.
- There are several stages to control an epidemic, starting with anticipation and ending with eradication. But it’s too late for most options today. With this level of cases, the two only options politicians have in front of them are containment and mitigation.
- Containment is sure all the cases are identified, controlled, and isolated. It’s what Singapore, Hong Kong, Japan or Taiwan are doing so well: They very quickly limit people coming in, identify the sick, immediately isolate them, use heavy protective gear to protect their health workers, track all their contacts, quarantine them… This works extremely well when you’re prepared and you do it early on, and don’t need to grind your economy to a halt to make it happen.
- Researchers estimate that the Wuhan travel ban only delayed the spread in China by 3-5 days.
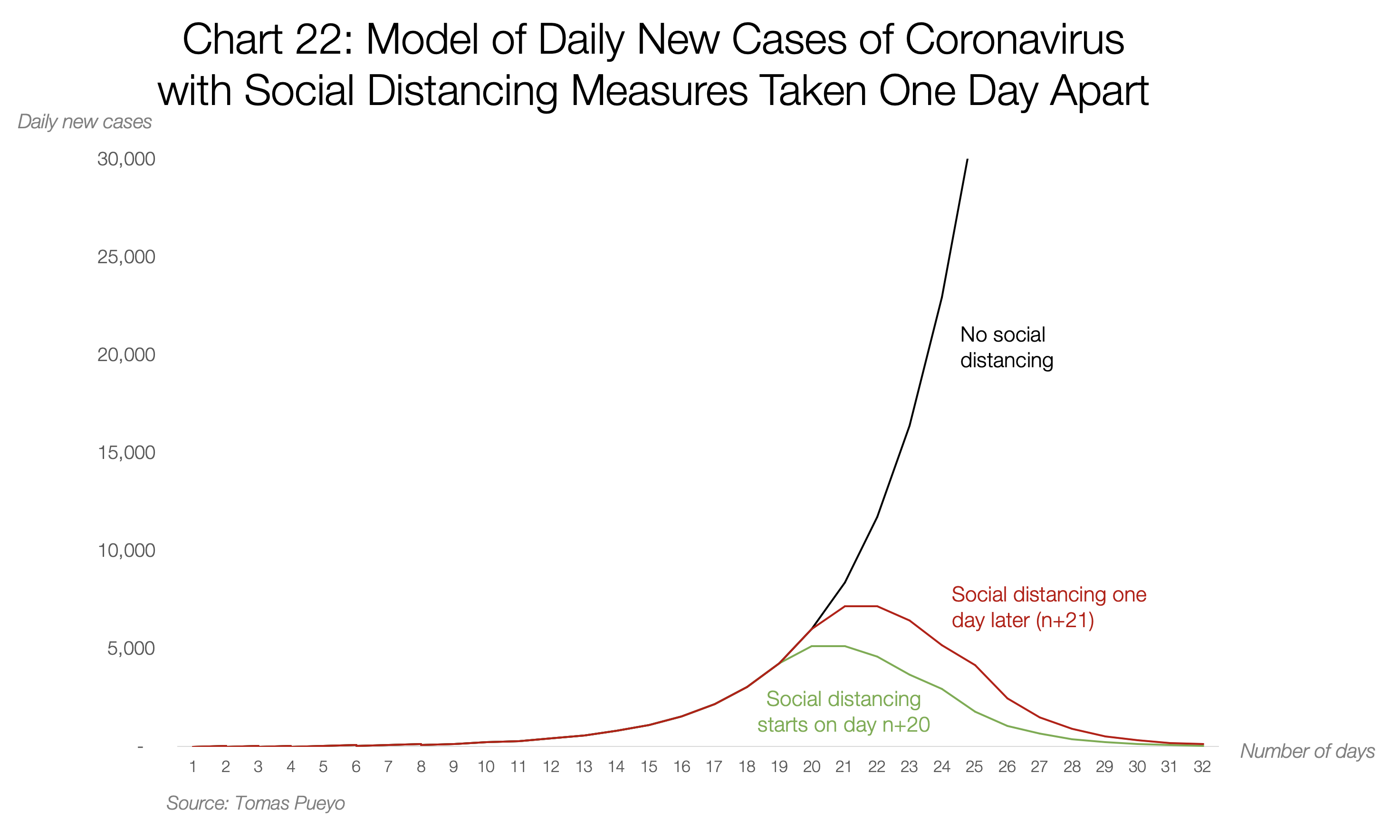
- Mitigation requires heavy social distancing. People need to stop hanging out to drop the transmission rate (R), from the R=~2–3 that the virus follows without measures, to below 1, so that it eventually dies out. These measures require closing companies, shops, mass transit, schools, enforcing lockdowns… The worse your situation, the worse the social distancing. The earlier you impose heavy measures, the less time you need to keep them, the easier it is to identify brewing cases, and the fewer people get infected. This is what Wuhan had to do. This is what Italy was forced to accept. Because when the virus is rampant, the only measure is to lock down all the infected areas to stop spreading it at once. With thousands of official cases — and tens of thousands of true ones — this is what countries like Iran, France, Spain, Germany, Switzerland or the US need to do. But they’re not doing it.
Coronavirus: Why You Must Act Now
Politicians, Community Leaders and Business Leaders: What Should You Do and When?

Tomas Pueyo
Updated on 3/13/2020. Now reflects an update on containment vs. mitigation strategies. 17 translations at the bottom. Send me more existing translations in private notes at the bottom. This article has received 21million views in the last 48h.
With everything that’s happening about the Coronavirus, it might be very hard to make a decision of what to do today. Should you wait for more information? Do something today? What?
Here’s what I’m going to cover in this article, with lots of charts, data and models with plenty of sources:
- How many cases of coronavirus will there be in your area?
- What will happen when these cases materialize?
- What should you do?
- When?
When you’re done reading the article, this is what you’ll take away:
The coronavirus is coming to you.
It’s coming at an exponential speed: gradually, and then suddenly.
It’s a matter of days. Maybe a week or two.
When it does, your healthcare system will be overwhelmed.
Your fellow citizens will be treated in the hallways.
Exhausted healthcare workers will break down. Some will die.
They will have to decide which patient gets the oxygen and which one dies.
The only way to prevent this is social distancing today. Not tomorrow. Today.
That means keeping as many people home as possible, starting now.
As a politician, community leader or business leader, you have the power and the responsibility to prevent this.
You might have fears today: What if I overreact? Will people laugh at me? Will they be angry at me? Will I look stupid? Won’t it be better to wait for others to take steps first? Will I hurt the economy too much?
But in 2–4 weeks, when the entire world is in lockdown, when the few precious days of social distancing you will have enabled will have saved lives, people won’t criticize you anymore: They will thank you for making the right decision.
Ok, let’s do this.
Share the Word
This is probably the one time in the last decade that sharing an article might save lives. They need to understand this to avert a catastrophe. The moment to act is now.
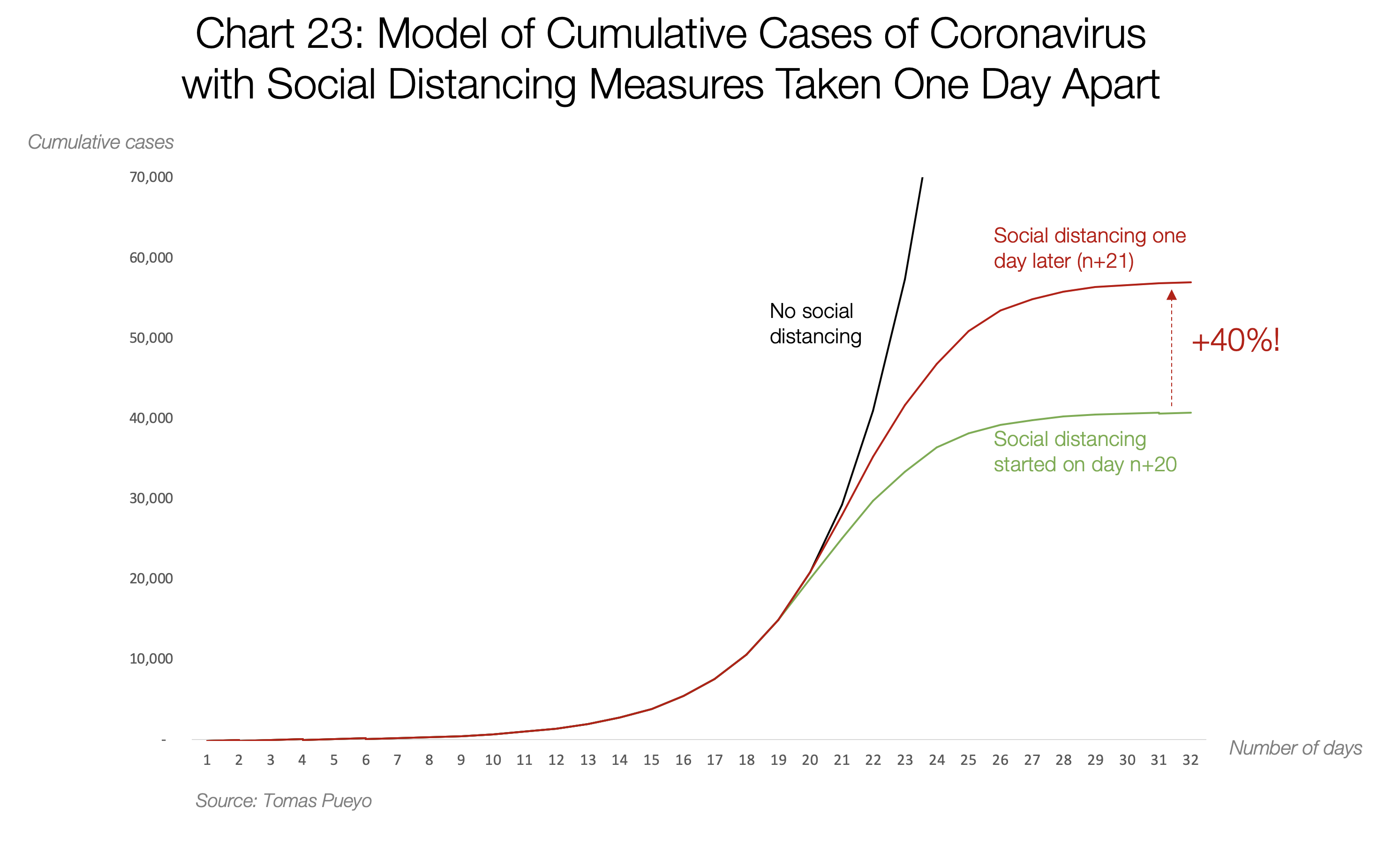
Below are a few graphics from the link, showing how big of a difference even one day's worth of social distancing can make down the road in daily new cases and eventual cumulative total cases. The article has a ton of other graphics illustrating what happened in many countries and what is expected to happen in selected countries, based on epidemiological models, incorporating what actually happened in countries that handled things similarly.