
It’s bound to fail and just a bad idea . Still lag behind getting out the first dose never mind a 2nd. Poor planning all around at every level.Let’s trust the people to do the right thing. Isn’t that right Ms. Perischelli?And Biden has talked about opening up vaccinations to anyone who wants one. My only concern is then not having enough vaccines for 2nd shots for people who got their first one. They're banking on keeping a smaller inventory (10% held back for 2nd shots vs. the current 50%), assuming additional vaccines will be available. It's a little risky, but maybe worth it - not sure, to be honest...
https://www.cnn.com/2021/01/08/politics/biden-vaccine-strategy/index.html
Colleges
- American Athletic
- Atlantic Coast
- Big 12
- Big East
- Big Ten
- Colonial
- Conference USA
- Independents (FBS)
- Junior College
- Mountain West
- Northeast
- Pac-12
- Patriot League
- Pioneer League
- Southeastern
- Sun Belt
- Army
- Charlotte
- East Carolina
- Florida Atlantic
- Memphis
- Navy
- North Texas
- Rice
- South Florida
- Temple
- Tulane
- Tulsa
- UAB
- UTSA
- Boston College
- California
- Clemson
- Duke
- Florida State
- Georgia Tech
- Louisville
- Miami (FL)
- North Carolina
- North Carolina State
- Pittsburgh
- Southern Methodist
- Stanford
- Syracuse
- Virginia
- Virginia Tech
- Wake Forest
- Arizona
- Arizona State
- Baylor
- Brigham Young
- Cincinnati
- Colorado
- Houston
- Iowa State
- Kansas
- Kansas State
- Oklahoma State
- TCU
- Texas Tech
- UCF
- Utah
- West Virginia
- Illinois
- Indiana
- Iowa
- Maryland
- Michigan
- Michigan State
- Minnesota
- Nebraska
- Northwestern
- Ohio State
- Oregon
- Penn State
- Purdue
- Rutgers
- UCLA
- USC
- Washington
- Wisconsin
High Schools
- Illinois HS Sports
- Indiana HS Sports
- Iowa HS Sports
- Kansas HS Sports
- Michigan HS Sports
- Minnesota HS Sports
- Missouri HS Sports
- Nebraska HS Sports
- Oklahoma HS Sports
- Texas HS Hoops
- Texas HS Sports
- Wisconsin HS Sports
- Cincinnati HS Sports
- Delaware
- Maryland HS Sports
- New Jersey HS Hoops
- New Jersey HS Sports
- NYC HS Hoops
- Ohio HS Sports
- Pennsylvania HS Sports
- Virginia HS Sports
- West Virginia HS Sports
ADVERTISEMENT
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
OT: COVID Science - Pfizer/Moderna vaccines >90% effective; Regeneron antibody cocktail looks very promising in phase II/III trial and more
- Thread starter RU848789
- Start date
- Status
- Not open for further replies.
You still think contract tracing will be possible after vaccinating several million. Good luck with that idea.I think until we have data on vaccinated people getting asymptomatic infections and then infecting others (through contact tracing, presumably), we simply won't know, but would have to assume they could be carriers.

I don’t know if you’ve answered this in these threads and results of JNJ still have to come out but assume they will at least be satisfactory...if you had a choice of vaccine PFE, Moderna, JNJ, AZ which would you choose?Absolutely, assuming we see somewhat similar protection as seen for the Moderna and Pfizer mRNA vaccines. Out of the 40 severe COVID cases during the combined Pfizer/Moderna clinical trials, all but one were in the placebo group, so the vaccines not only have a 95% reduction in the chances of getting symptomatic COVID, they also clearly lessen the severity of infections for those who do become infected.
Specifically, Moderna had 185 symptomatic cases in the placebo group, while only having 11 symptomatic cases in the vaccinated group, who received two doses for an efficacy of 94.1%. And Moderna's vaccine had 100% efficacy against severe disease, as there were zero severe COVID-19 cases among those vaccinated, but 30 severe cases in the placebo group, including one death from the disease.
Pfizer's data were similar with 170 symptomatic cases in the placebo group, while only having 8 symptomatic cases in the vaccinated group, who received two doses, for an efficacy of 95.0%. And Pfizer's vaccine had a very high efficacy against severe disease, as there was only one severe COVID-19 case among those vaccinated, but 10 severe cases in the placebo group (no deaths).
https://www.sciencemag.org/news/202...ernas-vaccine-trial-developed-severe-covid-19
If the gov feels the inventory is normalizing and predictable, then they should absolutely administer the vaccines that are currently reserved. Would be crazy not to.
It sounds like this is exactly what will be occurring. The doses won't be held back, with the hopefully correct assumption manufacturing will meet demand for the second doses. Just saw the news on CNBC.
 www.cnbc.com
www.cnbc.com
Separate issue, but I saw that NYC just announced that Citi Field will be a 24/7, 7 days a week vaccine location.
CDC expands Covid vaccination guidelines to everyone 65 and older
The states' focus on vaccinating health-care workers and nursing homes has created a bottleneck, the official said.
Separate issue, but I saw that NYC just announced that Citi Field will be a 24/7, 7 days a week vaccine location.

The Future of the Coronavirus? An Annoying Childhood Infection (Published 2021)
Once immunity is widespread in adults, the virus rampaging across the world will come to resemble the common cold, scientists predict.
This is what I have been talking about as far as optimizing injections. Moderna and Pfizer appear to be producing 60 million doses a month. Sequenced that’s 60 million administered with 30 million full inoculations a month. If and when JJ comes on line how many will they produce per month? Theirs will be a 1 dose so could see a bug ramping there.It sounds like this is exactly what will be occurring. The doses won't be held back, with the hopefully correct assumption manufacturing will meet demand for the second doses. Just saw the news on CNBC.
CDC expands Covid vaccination guidelines to everyone 65 and older
The states' focus on vaccinating health-care workers and nursing homes has created a bottleneck, the official said.
Separate issue, but I saw that NYC just announced that Citi Field will be a 24/7, 7 days a week vaccine location.
Why not call up national guard to help admin doses quickly at locations throughout? Just an idea.
It sounds like this is exactly what will be occurring. The doses won't be held back, with the hopefully correct assumption manufacturing will meet demand for the second doses. Just saw the news on CNBC.
CDC expands Covid vaccination guidelines to everyone 65 and older
The states' focus on vaccinating health-care workers and nursing homes has created a bottleneck, the official said.
Separate issue, but I saw that NYC just announced that Citi Field will be a 24/7, 7 days a week vaccine location.
Can you mix and match vaccines. Don’t believe so.This is what I have been talking about as far as optimizing injections. Moderna and Pfizer appear to be producing 60 million doses a month. Sequenced that’s 60 million administered with 30 million full inoculations a month. If and when JJ comes on line how many will they produce per month? Theirs will be a 1 dose so could see a bug ramping there.
Why not call up national guard to help admin doses quickly at locations throughout? Just an idea.
I guess no baseball this year.It sounds like this is exactly what will be occurring. The doses won't be held back, with the hopefully correct assumption manufacturing will meet demand for the second doses. Just saw the news on CNBC.
CDC expands Covid vaccination guidelines to everyone 65 and older
The states' focus on vaccinating health-care workers and nursing homes has created a bottleneck, the official said.
Separate issue, but I saw that NYC just announced that Citi Field will be a 24/7, 7 days a week vaccine location.
I don’t know if you’ve answered this in these threads and results of JNJ still have to come out but assume they will at least be satisfactory...if you had a choice of vaccine PFE, Moderna, JNJ, AZ which would you choose?
I consider the two mRNA vaccines as being essentially identical, so I'd take one of those, since they have higher demonstrated efficacy than the Astra-Zeneca vaccine, which also still has a number of oddities and questions surrounding it, as have been discussed before (post below, including Derek Lowe's take), plus they're the only two approved so far in the US. And we have no idea, yet, on what the J&J results will be. If it's close to the ~95% effectiveness of the mRNA vaccines I might pick that one, as it's a single shot.
Lots of vaccine questions and Derek Lowe came out with a very good blog entry on the vaccine landscape for the major players; it's so good, the entire entry is below. I agree with him that while the Pfizer/BioNTech and Moderna mRNA vaccines are off to a slow vaccination start, hopefully the CDC is right that we'll see vaccination numbers rise quickly. We do this every year for the flu and it shouldn't be that much harder for these vaccines, even with cryo conditions required for the Pfizer vaccine - this is a distribution issue, not a supply issue.
With regard to other vaccines, the most concerning issue is that many experts are now starting to believe that that UK variant may well be more infectious than previous strains and that is likely part of the reason why the UK gave an earlier approval to the Astra-Zeneca/Oxford vaccine in the UK, especially for a potential single shot, where, with a more transmissible variant, one shot of a pretty good vaccine for twice as many people is better than two shots of a better vaccine for half as many people. Hopefully, we don't have to make a decision like that here if we can get the mRNA vaccination rates up and if we don't get high rates of the UK variant. Lots of questions still on how they ran their trial, which Lowe details below.
The other thing people need to keep in mind is that the J&J vaccine has a lot of similarities to the AZ vaccine, as both are adenovirus vector vaccines, with the AZ one using a chimp adenovirus to carry the genetic info on it for the spike protein to prime people's immune systems to make antibodies to SARS-CoV-2, while the J&J one uses a fairly rare human adenovirus vector - that means it's possible that the issues with dosing seen for AZ might apply here, although we'll see pretty soon what their first phase III trial using a single dose shows. If it shows even modest efficacy (like ~70%) and good safety from a single shot, we're likely to see it still used a lot.
He also covers the vaccines from Russia and the three from China, with lots of skepticism on these, although they are being deployed in some countries, as well as the Novavax recombinant protein vaccine, which is an exciting entry and which just started phase III trials.
https://blogs.sciencemag.org/pipeline/archives/2020/12/30/vaccine-roundup-late-december
Vaccine Roundup, Late December
By Derek Lowe 30 December, 2020
There’s been a lot of news, so it’s time to survey the vaccine landscape. For this post, I’m only going to cover the big players that are either deep into human trials or have actually been rolling out vaccines to the general population – another post to come will go further down the list. But that still leaves us with plenty to talk about. The situation is. . .well, I’m going with “chaotic”, overused though it is.
I don’t have separate categories for the Pfizer/BioNTech and Moderna vaccines this time, since they’re already under EUA here in the US and people are being vaccinated as we speak. That rollout is worth a longer discussion, but it’s as much politics as it is medicine. Vice President Pence’s statement earlier this month of having 20 million people vaccinated by the end of the year is totally out of reach, though, and I believe that he has now altered that to having 20 million doses shipped (and I’m not even sure about that). The CDC says that vaccinated numbers should start rising steeply, and I certainly hope that’s the case.
Oxford/AstraZeneca: As the world knows, this adenovirus vector vaccine has been a messy one. I think that both partners need to take responsibility for some real mistakes in the trial execution and further mistakes in their announcements since the data became available. But I haven’t seen any sign of that (although I would be even happier than usual to be corrected on that point).
Last night, the UK authorities approved this vaccine for distribution there. Of special interest is the intent to give as many people as possible a first shot, without holding back supplies for the second round. I think that this is simultaneously the correct decision for them to make and also very bad news. It appears that the coronavirus variant first reported there is indeed more contagious: Trevor Bedford is convinced, and we have early data that would seem to only make sense if the R for this form is indeed higher. One mechanism for that may be higher viral load developing in patients more quickly, making them presumably more infectious (via shedding more viral particles). That said, it also appears (so far) that the course of disease with this variant is not actually worse than the other strains, but it’s not any better, either. And with higher transmission, that’s bad enough. (Note that the WHO believes that the South Africa variant is spreading quickly as well).
That situation in the UK appears to be one of the biggest factors driving the approval and rollout, and I see their point: this vaccine is indeed better than nothing, one shot for more people is likely to be better than two-shots-for-some, and it looks like they’re going to need all the help they can get. But “better than nothing” is a rough place to be. So what do we know about the efficacy of a single shot of the Oxford/AZ vaccine, and about the effect of waiting for a second one?
All I can say is that attempts to answer those questions land you immediately in a confusing mess. It’s a mess made worse by AstraZeneca, whose CEO has made statements about the vaccine’s efficacy that are not (so far) backed up by actual numbers. If you’d like me to name a major drug company that’s going to come out of this pandemic looking worse, it’s them. Anyway, as you’ll recall, initially there was a hint that a lower first dose followed by a standard second dose might be more protective overall (although I don’t think the evidence for that is very strong at all, considering the statistical spread in the data). But now there’s a report that increased efficacy might be driven by an even longer wait between the two doses. I don’t find that evidence very compelling, either (we’re getting into some pretty small subgroups by this point, and that is always a dangerous area to draw conclusions from). And if you’re going to leave people walking around with a half dose at first, or a full dose but with a longer wait for the second one, it makes the question above even more crucial: how protective is one dose?
We do not know. We don’t know for this vaccine, nor for the Pfizer/BioNTech one, nor for Moderna’s. No studies have been designed to find that out, so all we can do is guess based on what we’ve seen with the interval between doses in the two-dose studies. That’s been encouraging with the two mRNA vaccines, but remember: we don’t know how they are over a longer period, because no one was left without a second dose for that long. It’s certainly possible that without the second booster that the protection seen after one shot starts to wane. We do not know. And we know even less about the Oxford/AZ vaccine’s behavior under these conditions. Giving as many people in the UK as possible a single dose of that vaccine with a longer wait until the booster is a gamble, and you wouldn’t want to do it that way if the alternatives weren’t even worse. It’s the right move, unfortunately, and it’s a damned shame it’s come to this.
The US trial of this vaccine was paused for weeks, of course, while adverse events were investigated. It’s basically fully enrolled now, and the data will include many more elderly patients than have been investigated to date. I would assume that our current terrible infection rates will allow this trial to move along rather quickly, but I have no estimate of when we might see it report.
J&J: data on the one-dose clinical trial of this adenovirus vector candidate should be coming very soon indeed. It’s going to be of great interest, given the results from the Oxford/AZ effort, and given the deliberate one-dose protocol. The company has a two-dose trial underway as well, but we won’t be seeing data on that one until later.
CanSino: this adenovirus vector vaccine (Ad5) is said to be submitting data to Mexico shortly, presumably for regulatory approval. Trials have been underway there, as well as in Pakistan, Chile, and other countries. No efficacy or safety data have been reported publicly, however.
Gamaleya Research Institute: this two-adenovirus-vector two-dose vaccine has made some news as well. Earlier this month, a press release from the GRI said that the vaccine was 91% effective, based on a trial with over 17,000 vaccinated patients and over 5600 controls. The release also says that a full paper is in the works, to be published in a leading journal, and I very much look forward to that. It appears that the vaccine is now being shipped to Belarus, Argentina and Hungary, but Reuters reports that the Argentina shipment is for only the first dose, which is the easier of the two different adenovirus vectors to manufacture. Nothing on the other countries as yet, but the Hungarian shipment was quite small (6,000 doses), which tells you that it’s more in press-release territory anyway. It’s unclear what’s going on – Reuters had a source saying that the Argentine shipment was excess production from the manufacture of the first shot, and that they’re still catching up on the second. I have seen no reliable figures on the protection offered by just that first shot – the director of the GRI has said, though, that immunity from the first shot lasts only 3 to 4 months.
Meanwhile, the earlier reported collaboration between GRI and AstraZeneca seems to be real – a clinical trial has been registered. I’m quite curious to see how this is going to go, and whether it will produce results in time to make any sort of impact.
Sinovac: Word has just come in the last couple of days from a trial in Turkey of this inactivated virus vaccine. Turkish officials said that it was 91% effective, but we have no numbers to back that up yet. What we do know is that this was based on a rather small trial (752 people vaccinated, 570 in the control group), so the confidence interval on that number is surely going to be large. Sinovac, for its part, seems to have said nothing yet. I’m glad to see that this vaccine seems to be working, but you would really want to see a lot more data on both efficacy and safety.
SinoPharm/Beijing Institute: this inactivated-virus vaccine candidate has just reported data in The Lancet from its Phase 1/2 trials (safety and immunogenicity). And they have now announced that interim analysis of Phase 3 data show 79% efficacy, but with no actual numbers yet. Note that this is the same one that UAE officials announced an 86% efficacy for, but (as far as I can see) SinoPharm has still made no comment on that. Everyone would very much like to have a more complete look at the data, but there is no word on when that will be forthcoming. We don’t know how many people were in these trials, the inclusion or diagnostic criteria used, nor do we have any safety data at all. So this could be encouraging, but I myself would rather stay home and wait for something with more numbers behind it, rather than take a vaccine on this basis. More on this as more data appear.
Novavax: this should be the next trial we hear about after J&J reports, and a lot of people are waiting to see how this recombinant-protein candidate works out. These will be results from a trial in the UK – a US Phase 3 just launched this week. This one has much less rigorous storage requirements and is generally easier to manufacture, and it could be a big contributor if things work out.
There will be baseball this year. Even if we "only" have 75-100MM vaccinated by April, that, combined with a pretty high number of infected/recovered/immune people by then (30%?), that's a much better place than we were in this past year where we had baseball and other sports. The bigger question is fans. I'm hoping we'll have more data on low transmission rates from vaccinated people by then, which would make it very likely vaccinated (and probably recovered/immune) fans could attend.I guess no baseball this year.
Not in the Bronx with that poorly assembled team.I guess no baseball this year.
My wife , son and I went to two Somerset patriot games last season. They had a series of exhibition games against the NJ Blasters. It was fun. The Patriots won the series and got the Joe Torre trophy, the best pitcher got the Sparky Lyle trophy and the series MVP got the Willie Randolph trophy .They only allowed 500 people in per game and they did sell out each game. The Sussex Miners and NJ Jackels also did something similar . I don't know if fans were allowed. My feeling is baseball will be played . Too much money to lose again if they don't. They will figure it out.There will be baseball this year. Even if we "only" have 75-100MM vaccinated by April, that, combined with a pretty high number of infected/recovered/immune people by then (30%?), that's a much better place than we were in this past year where we had baseball and other sports. The bigger question is fans. I'm hoping we'll have more data on low transmission rates from vaccinated people by then, which would make it very likely vaccinated (and probably recovered/immune) fans could attend.
I hope you are right. I dont see a 100 million before April. Most of these "mega-centers" we are seeing now can only vaccinate 2,500 max a day. NJ only has current plans of just 6 of them. That is not nearly enough. Its been a horrible start.There will be baseball this year. Even if we "only" have 75-100MM vaccinated by April, that, combined with a pretty high number of infected/recovered/immune people by then (30%?), that's a much better place than we were in this past year where we had baseball and other sports. The bigger question is fans. I'm hoping we'll have more data on low transmission rates from vaccinated people by then, which would make it very likely vaccinated (and probably recovered/immune) fans could attend.
CVS has 20000 stores and who knows how many Walgreens. I agree poor planning at the top. Give it to the states and let 50 of them figure it out.I hope you are right. I dont see a 100 million before April. Most of these "mega-centers" we are seeing now can only vaccinate 2,500 max a day. NJ only has current plans of just 6 of them. That is not nearly enough. Its been a horrible start.
Not all of those stores have the deep freezers. We seen many examples of wasted vaccines because of that.CVS has 20000 stores and who knows how many Walgreens. I agree poor planning at the top. Give it to the states and let 50 of them figure it out.
It has been given to the states! That is where the plans failed, at the state level.
wait only a year....hahaha.....$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$

 www.forbes.com
www.forbes.com
Moderna Says Its Covid-19 Vaccine Provides One Year’s Immunity
The U.S. has ordered 200 million doses of the Moderna vaccine, enough to immunize 100 million people.
www.forbes.com
US to require all arriving passengers to get COVID-19 test
The CDC order is to take effect in about two weeks, on Jan. 26. It requires air passengers to get a COVID-19 test within three days before their flight departs to the U.S., and to provide written proof of the test result to the airline. Travelers can also provide documentation that they had the infection in the past and recovered.
Airlines are ordered to stop passengers from boarding if they don’t have proof of a negative test or a prior infection.

 www.pix11.com
www.pix11.com
The CDC order is to take effect in about two weeks, on Jan. 26. It requires air passengers to get a COVID-19 test within three days before their flight departs to the U.S., and to provide written proof of the test result to the airline. Travelers can also provide documentation that they had the infection in the past and recovered.
Airlines are ordered to stop passengers from boarding if they don’t have proof of a negative test or a prior infection.
US to require all arriving passengers to get COVID-19 test
Anyone flying to the U.S. will soon need to show proof of a negative test for COVID-19, health officials announced Tuesday. The Centers for Disease Control and Prevention requirement expands on a s…
www.pix11.com
Which is stupid. Getting a test means at that moment you have it or not. It doesn't actually mean you don't have it as we see false negatives and within 3 days anyone can get it.US to require all arriving passengers to get COVID-19 test
The CDC order is to take effect in about two weeks, on Jan. 26. It requires air passengers to get a COVID-19 test within three days before their flight departs to the U.S., and to provide written proof of the test result to the airline. Travelers can also provide documentation that they had the infection in the past and recovered.
Airlines are ordered to stop passengers from boarding if they don’t have proof of a negative test or a prior infection.
US to require all arriving passengers to get COVID-19 test
Anyone flying to the U.S. will soon need to show proof of a negative test for COVID-19, health officials announced Tuesday. The Centers for Disease Control and Prevention requirement expands on a s…
It depends on the vaccination rate and the length of immunity. Some think those won't be high/long enough and there will always be some small pockets of infections, especially if some countries have really low vaccination rates, plus animals can be reservoirs for viruses to allow reintroduction at a later date. If immunity only lasts a year or so (like other betacoronaviruses which cause the common cold), then people might require annual vaccinations, which might lead to lower compliance and more risk the virus sticks around.
However, more recent data (2nd link) are indicating that immunity levels may last for several years - if that's the case and we can get 60-70% or more vaccinated, there's a good chance the virus will disappear, like SARS/MERS did - people with SARS/MERS still have relevant immunity markers 10+ years later (doesn't "prove" immunity, since those outbreaks died out).
We also don't know, yet, what percentage of vaccinated people might still get infected and whether they'll be infectious - we just know the levels of people with symptoms/COVID were low (~5% or so), but don't know how many might have been asymptomatic, but possibly infectious. So, the jury is still out on many questions which need to be answered to know if SARS-CoV-2 becomes endemic or not. Let's hope not.
https://science.sciencemag.org/content/370/6516/527
https://rutgers.forums.rivals.com/t...ase-ii-iii-trial-and-more.203426/post-4782651
Have a long post on the variants in the main COVID thread last night. I would argue that whether or not this virus becomes endemic is an open question. If enough people get vaccinated before the virus mutates enough, via antigenic drift, to "escape" the vaccine, then transmission rates could go to zero and the virus could be stamped out (this would need to happen worldwide, though), like SARS/MERS were. Length of immunity/effectiveness of the vaccines (and infection/immunity) is also key here.
I don't think anyone knows, though, how quickly we can get transmission rates to be very low, and when/if the virus will mutate enough to render the current vaccines ineffective. It's doubtful that happens in the next year, though, which will hopefully give us enough time to get transmission rates to very low levels. Also, at least with the mRNA vaccines, they're easy to "retool" to provide efficacy against a virus mutated enough to escape the current vaccines (would take a month or two), which might allow us to keep ahead of new variants. Much of this was discussed in the post below, with the ScienceMag article being a very good one on this.
Been talking a lot about the future of SARS-CoV-2 lately, especially with regard to whether variants will emerge which vaccines or previous COVID infections won't provide immunity to (not yet and hopefully not for awhile), as well as whether the virus will eventually "disappear" like SARS/MERS (previous similar coronaviruses) or become endemic, but probably mostly harmless, like a host of existing coronaviruses that cause the common cold.
Well today a paper came out from Lavine, et al, on the topic of endemicity, entitled, "Immunological characteristics govern the transition of COVID-19 to endemicity," which is getting a lot of attention among scientists and even the mainstream press. Basically, they're predicting that COVID will eventually become endemic and likely no more virulent than the common cold, but they talk a lot about the path to get there being far less deadly if this endpoint is reached via vaccination rather than transmission. An excerpt from their abstract is below.
https://science.sciencemag.org/content/early/2021/01/11/science.abe6522
We are currently faced with the question of how the CoV-2 severity may change in the years ahead. Our analysis of immunological and epidemiological data on endemic human coronaviruses (HCoVs) shows that infection-blocking immunity wanes rapidly, but disease-reducing immunity is long-lived. Our model, incorporating these components of immunity, recapitulates both the current severity of CoV-2 and the benign nature of HCoVs, suggesting that once the endemic phase is reached and primary exposure is in childhood, CoV-2 may be no more virulent than the common cold.
Since the paper is certainly pretty dense and complex, it might also be worth reading the article in today's Times by science writer Apoorva Mandavalli, who is truly excellent. She talks more about how we get there in the article, as per the excerpt below. As i've said countless times, if we rely on transmission to get us to "herd immunity" and are only 20-30% of the way there now with 380K deaths, getting to 70-80% infected, where transmissions woud likely end on their own would likely mean another 500K+ deaths and millions of serious illnesses - that's why vaccinating as fast as we can is so important in the US and worldwide.
https://www.nytimes.com/2021/01/12/health/coronavirus-immunity-future.html
In other words, the coronavirus will become “endemic,” a pathogen that circulates at low levels and only rarely causes serious illness.
“The timing of how long it takes to get to this sort of endemic state depends on how quickly the disease is spreading, and how quickly vaccination is rolled out,” said Jennie Lavine, a postdoctoral fellow at Emory University in Atlanta, who led the study.
“So really, the name of the game is getting everyone exposed for the first time to the vaccine as quickly as possible.”
Excellent and important new paper from La Jolla Institute of Immunology by Shane Crotty's group, which has been the subject of a few posts by me and @UMRU and others over the last several months. Essentially, they followed over 180 recovered infected patients for 5-8 months, performing the most comprehensive assessment of ongoing immunological marker levels in patients, by profiling antibodies, B-cells, and T-cells in their immune systems over time.
They found durable responses for the vast majority of people and have postulated that immunity in these people could very well last for years and it's expected that immunity from vaccines would likely be similar - see the excerpt below from the Times article (the paper is in the 2nd link), especially the part in bold. This work builds on the work done by many others around the world in recent months (some of which is in the 3rd/4th links from old posts of mine).
https://www.nytimes.com/2020/11/17/health/coronavirus-immunity.html/??
https://www.biorxiv.org/content/10.1101/2020.11.15.383323v1.full.pdf
https://rutgers.forums.rivals.com/threads/florida-halts-football-program-covid.202128/post-4726680
https://rutgers.forums.rivals.com/t...es-interventions-and-more.198855/post-4650144
How long might immunity to the coronavirus last? Years, maybe even decades, according to a new study — the most hopeful answer yet to a question that has shadowed plans for widespread vaccination.
Eight months after infection, most people who have recovered still have enough immune cells to fend off the virus and prevent illness, the new data show. A slow rate of decline in the short term suggests, happily, that these cells may persist in the body for a very, very long time to come.
The research, published online, has not been peer-reviewed nor published in a scientific journal. But it is the most comprehensive and long-ranging study of immune memory to the coronavirus to date.
“That amount of memory would likely prevent the vast majority of people from getting hospitalized disease, severe disease, for many years,” said Shane Crotty, a virologist at the La Jolla Institute of Immunology who co-led the new study.
And another really good paper came out today in the prestigious journal Cell, this time from Crotty and Settes (Crotty did the great paper a few months ago on profiling immune responses in infected/recovered patients, posted above), providing a great overview of the literature, to date, on the adaptive immune system and its role in COVID infections and vaccines. If you ever wanted to know anything about the human immune system and how it fights viral infections, it's probably either in here or in the bibliography. The summary is below. I assume @UMRU is all over this one. 😄
https://www.sciencedirect.com/science/article/abs/pii/S0092867421000076
Summary: While there is much more to be learned about adaptive immune responses to SARS-CoV-2 and their relationships to disease severity, immune memory, protection, and vaccines, an extraordinary amount has been accomplished during 2020. Studies of antigen-specific CD4+ T cells, CD8+ T cells, and antibodies together in larger cohorts of acute patients, representing a range of disease severity, are needed to further understand mechanisms of protective adaptive immune responses to COVID-19. Big unknowns remain about variable kinetics of viral loads and duration of infection and the connections between those parameters and adaptive immunity and immune memory. Understanding heterogenous disease manifestations of COVID-19 remains a major knowledge gap, and exploring relationships between those phenomena and adaptive immunity is a priority. Additionally, duration of immune memory, and protective immunity, to SARS-CoV-2 after COVID-19 and in response to COVID-19 vaccines will be a high priority for years to come.
Last edited:
It's not perfect, but it probably cuts out at least half the infectious people who might otherwise be traveling - it's 100x better than screening for temperature.Which is stupid. Getting a test means at that moment you have it or not. It doesn't actually mean you don't have it as we see false negatives and within 3 days anyone can get it.
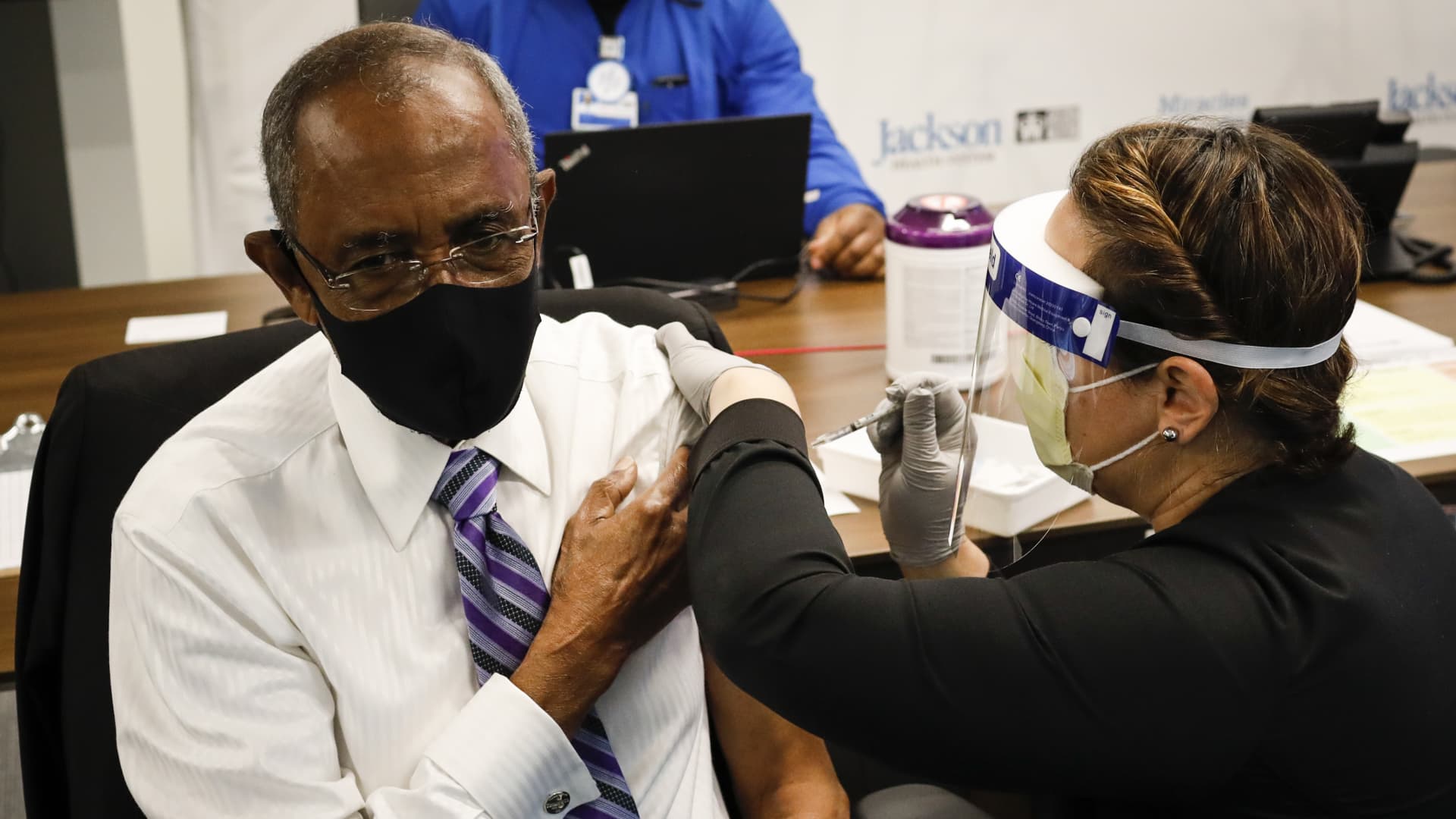
Got my second pfizer vaccine dose today, just a little soreness at injection site.
Shocker...NOT

 www.cnn.com
www.cnn.com
Chinese Covid-19 vaccine far less effective than initially claimed in Brazil, sparking concerns | CNN
A leading Chinese Covid-19 vaccine developed by Sinovac Biotech was just 50.38% effective in late-stage trials in Brazil, significantly lower than earlier results showed, according to a statement published by the government of Sao Paulo Tuesday.
Yep, think that’s from the same paper numbers posted about.
I laugh at this BS.
That's because an immunized person can still potentially...
Nobody knows this as fact. So they rather you catch the virus first than get vaccinated.
Can you provide a source for this? I am a 1B (+75) and was told by my town's Health Department yesterday they are still vaccinating the 1A health care workers
See this article and make sure you register on the site (link included in article)

N.J. to expand COVID vaccine eligibility to people 65 and older, Murphy says
Gov. Phil Murphy said the state will comply with the CDC's new guidelines for coronavirus vaccinations and expand eligibility within days.
Sorry Armin., I referenced the wrong post. Do you have a source for this post? I am not being critical, I am only trying to get reliable information about vaccine availability to 1B people. I was told by my town Health Department yesterday that they are still doing !A category and had no idea when 1B would begin.NJ opening up to 65+ today
Sorry Armin., I referenced the wrong post. Do you have a source for this post? I am not being critical, I am only trying to get reliable information about vaccine availability to 1B people. I was told by my town Health Department yesterday that they are still doing !A category and had no idea when 1B would begin.
No worries! See my reply above.
Murphy will be having his Wednesday press conference soon, so more info will be coming out this afternoon as well.
If you’re interested, they live stream the video conference on the nj.com Facebook page.
Last edited:
Some real life anecdotal information. Spoke to a group who owns 100 senior housing assisted living/ memory care facilities in the US with 12000 residents.
Partnered with CVS to conduct clinics. 35% of the way through senior population and expect to be finished with second dose by mid March. Have seen 95 to 100 percent acceptance.
Healthcare workers acceptance 50% as the majority are in child bearing years. 80% workforce is female and that concern is the biggest expressed by those not getting vaccinated. Lack of data. Younger men have also expressed this concern.
they cannot mandate it as they would have a problem with finding qualified people to work in these facilities. If they had 90% acceptance they could likely make it mandatory.
Partnered with CVS to conduct clinics. 35% of the way through senior population and expect to be finished with second dose by mid March. Have seen 95 to 100 percent acceptance.
Healthcare workers acceptance 50% as the majority are in child bearing years. 80% workforce is female and that concern is the biggest expressed by those not getting vaccinated. Lack of data. Younger men have also expressed this concern.
they cannot mandate it as they would have a problem with finding qualified people to work in these facilities. If they had 90% acceptance they could likely make it mandatory.
JNJ efficacy coming next week for sure. Slaoui is guessing 80%. At this point things are likely unblinded and he’s definitely catching some whispers. I’m guessing it will be 70-80% for at least the 18-65 cohort. Older than that this vaccine may struggle a bit based on some of the results outlined in the nejm paper that was released today.
Do we know how many doses they can produce and how quickly?JNJ efficacy coming next week for sure. Slaoui is guessing 80%. At this point things are likely unblinded and he’s definitely catching some whispers. I’m guessing it will be 70-80% for at least the 18-65 cohort. Older than that this vaccine may struggle a bit based on some of the results outlined in the nejm paper that was released today.
Disregard question. Found this. Looks like they are behind but could get to 60 million by February.
Redirect Notice
www.google.com
Disregard question. Found this. Looks like they are behind but could get to 60 million by February.
Redirect Notice
www.google.com
I'm sort of hoping that by the time I'm cleared to get one (40 yo, no medical issues) I'll be getting the JJ one dose vax.
Disregard question. Found this. Looks like they are behind but could get to 60 million by February.
Redirect Notice
www.google.com
Don’t think Feb, 60mil by April and they are trying to pull that in so they hit that mark sometime in March. At least that’s what the article says. Yesterday they were saying they’ll only be in the single digit millions for Feb, but trying to get into double digits,
Yup mistype. April. Was hoping they would have been able to ramp quicker than that.Don’t think Feb, 60mil by April and they are trying to pull that in so they hit that mark sometime in March. At least that’s what the article says. Yesterday they were saying they’ll only be in the single digit millions for Feb, but trying to get into double digits,
- Status
- Not open for further replies.
Similar threads
ADVERTISEMENT
ADVERTISEMENT