
Ahhh, gotcha - that makes it a bit easier. Gotta go watch one...No, you don't have to use all the numbers. You just have to use any of the numbers (once only) and the four math functions to make the total number. There is also a word scramble part to teh game (kind of like Boggle), and then there is just a lot of banter and obscenities. There is another show called Countdown, and it is a serious game show. This one is for fun. We never miss it.
Colleges
- American Athletic
- Atlantic Coast
- Big 12
- Big East
- Big Ten
- Colonial
- Conference USA
- Independents (FBS)
- Junior College
- Mountain West
- Northeast
- Pac-12
- Patriot League
- Pioneer League
- Southeastern
- Sun Belt
- Army
- Charlotte
- East Carolina
- Florida Atlantic
- Memphis
- Navy
- North Texas
- Rice
- South Florida
- Temple
- Tulane
- Tulsa
- UAB
- UTSA
- Boston College
- California
- Clemson
- Duke
- Florida State
- Georgia Tech
- Louisville
- Miami (FL)
- North Carolina
- North Carolina State
- Pittsburgh
- Southern Methodist
- Stanford
- Syracuse
- Virginia
- Virginia Tech
- Wake Forest
- Arizona
- Arizona State
- Baylor
- Brigham Young
- Cincinnati
- Colorado
- Houston
- Iowa State
- Kansas
- Kansas State
- Oklahoma State
- TCU
- Texas Tech
- UCF
- Utah
- West Virginia
- Illinois
- Indiana
- Iowa
- Maryland
- Michigan
- Michigan State
- Minnesota
- Nebraska
- Northwestern
- Ohio State
- Oregon
- Penn State
- Purdue
- Rutgers
- UCLA
- USC
- Washington
- Wisconsin
High Schools
- Illinois HS Sports
- Indiana HS Sports
- Iowa HS Sports
- Kansas HS Sports
- Michigan HS Sports
- Minnesota HS Sports
- Missouri HS Sports
- Nebraska HS Sports
- Oklahoma HS Sports
- Texas HS Hoops
- Texas HS Sports
- Wisconsin HS Sports
- Cincinnati HS Sports
- Delaware
- Maryland HS Sports
- New Jersey HS Hoops
- New Jersey HS Sports
- NYC HS Hoops
- Ohio HS Sports
- Pennsylvania HS Sports
- Virginia HS Sports
- West Virginia HS Sports
ADVERTISEMENT
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
COVID-19 Pandemic: Transmissions, Deaths, Treatments, Vaccines, Interventions and More...
- Thread starter RU848789
- Start date
- Status
- Not open for further replies.
May have missed this one, but good news out of Hong Kong, as a randomized, controlled, open label study comparing a triplet antiviral cocktail of lopinavir–ritonavir, and ribavirin with interferon beta-1b, showed that this combo was safe and superior to lopinavir–ritonavir alone in shortening virus shedding, alleviating symptoms, and facilitating discharge of patients with mild to moderate COVID-19. These are the kinds of patients who benefitted from remdesivir in its recent trial.
Great to have more options, but we still need drugs to treat more serious cases. Nobody died in the study, so it's not clear to me if these were simply people who would have recovered anyway (or if even the lopinavir-ritonavir "control" would have prevented people from progressing to serious illness). I didn't see that discussed in the paper, but might have missed it.
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)31042-4/fulltext
Great to have more options, but we still need drugs to treat more serious cases. Nobody died in the study, so it's not clear to me if these were simply people who would have recovered anyway (or if even the lopinavir-ritonavir "control" would have prevented people from progressing to serious illness). I didn't see that discussed in the paper, but might have missed it.
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)31042-4/fulltext

Again, you are throwing away data that can be useful in making critical decisions in a real time crisis. If you have 11% of those tested being positive when you are narrowly focused on those who are sick and then shift to a much wider regimen, and get 7%, then you have data to chew on. If you know how the wider testing was established, you can make a reasonable estimate of whether you are witnessing a decrease or increase in total numbers.Sure, if you can estimate how many of the latest 7% would have been likely to test positive under the previous approach. But you do not have that info so your judgement on 11 v 7 is flawed. To what degree? I do not have access to the two protocols to make an intelligent estimate of how many of the 7% would likely have been tested. If it is say 1/3 then, the comparison is 11% to 2% which would mean something very different than 11 v 7.
The key here is that decisions need to be made and the comparison of these data isn't appropriately to perfect data, but rather to no data. A type one error in this situation is unfortunate, but a type two error could kill.
Not that this is unexpected but just shows how difficult it will be for some places to get back to a “normal” and this is in SK who has such specificity in tracking, tracing etc...
From CNN:
All bars in Seoul have been ordered to close until further notice after a spike in coronavirus cases linked to nightclubs in the South Korean capital.
At a briefing Saturday, Seoul Mayor Park Won-soon said that clubs and bars would all need to shut, effective immediately.
A spike in cases: The order follows a surge in cases connected with nightclubs in Itaewon, a popular nightlife district in Seoul.
On Thursday, a 29-year-old man from the city of Yongin -- on the outskirts of Seoul -- tested positive for the virus. The person visited several clubs in Itaewon on the night of May 1 and the early hours of May 2, according to the Korea Centers for Disease Control and Prevention (KCDC).
Since then, 40 others believed to be connected to the case have tested positive. Of those, 27 are from Seoul.
Tracking partygoers: South Korea has not introduced a nationwide lockdown, but has brought in additional measures to control the coronavirus outbreak. At nightclubs, for instance, people must provide their full name and phone number before entry.
According to Park, 1,946 names were listed on the registry books of the three clubs the 29-year-old visited. Only 647 of those people have been identified.
More cases possible: Kwon Joon-wook, deputy director of the KCDC, also said there may have been more than one source of infection behind the nightclub outbreak. Some of the people who have been confirmed positive visited clubs on different nights from the 29-year-old.
“We’ve put in much efforts and made a lot of sacrifices," Park added Saturday. "Are we just to let this all go to waste because of few people’s carelessness?”
A setback in South Korea: Before the nightclub-related spike, new coronavirus cases had been trending down in the country. On Tuesday, South Korea reported its lowest number of new cases for more than two months.
According to Johns Hopkins University, South Korea has reported more than 10,800 coronavirus cases and 256 deaths. The vast majority of South Korea's cases have recovered, the KCDC said earlier this week.
From CNN:
All bars in Seoul have been ordered to close until further notice after a spike in coronavirus cases linked to nightclubs in the South Korean capital.
At a briefing Saturday, Seoul Mayor Park Won-soon said that clubs and bars would all need to shut, effective immediately.
A spike in cases: The order follows a surge in cases connected with nightclubs in Itaewon, a popular nightlife district in Seoul.
On Thursday, a 29-year-old man from the city of Yongin -- on the outskirts of Seoul -- tested positive for the virus. The person visited several clubs in Itaewon on the night of May 1 and the early hours of May 2, according to the Korea Centers for Disease Control and Prevention (KCDC).
Since then, 40 others believed to be connected to the case have tested positive. Of those, 27 are from Seoul.
Tracking partygoers: South Korea has not introduced a nationwide lockdown, but has brought in additional measures to control the coronavirus outbreak. At nightclubs, for instance, people must provide their full name and phone number before entry.
According to Park, 1,946 names were listed on the registry books of the three clubs the 29-year-old visited. Only 647 of those people have been identified.
More cases possible: Kwon Joon-wook, deputy director of the KCDC, also said there may have been more than one source of infection behind the nightclub outbreak. Some of the people who have been confirmed positive visited clubs on different nights from the 29-year-old.
“We’ve put in much efforts and made a lot of sacrifices," Park added Saturday. "Are we just to let this all go to waste because of few people’s carelessness?”
A setback in South Korea: Before the nightclub-related spike, new coronavirus cases had been trending down in the country. On Tuesday, South Korea reported its lowest number of new cases for more than two months.
According to Johns Hopkins University, South Korea has reported more than 10,800 coronavirus cases and 256 deaths. The vast majority of South Korea's cases have recovered, the KCDC said earlier this week.
I don't know what to say after reading this...
My brother in-law's kid (18) works part time in the kitchen of a nursing facility up in north Jersey.
My sister in-law is a nurse.
A few weeks ago, she was diagnosed with the Covid. Actually got really sick, but never sick enough to be hospitalized.
On the Friday evening we did a family Zoom happy hour. The B-I-L is downstairs, she's in bed with their 16 year-old daughter sitting in the bed next to her. She sounds like death. Somebody asks "where's Michael?" "Oh, he's at work."
After the call, everyone was on the phone, texting back and forth, utterly incredulous. My other B-I-L finds out the name of the nursing home the kid works at and calls them to say that they have a food service employee who is working while his mother is in bed with the Covid. Their response? "Oh, yes. We know."
There's nothing to be done. No laws have been broken.
Oh, I'm sure it is a lost cause, in general. However, I know at least one school is still committed to it and our little one adores cursive.Sadly, the student that the Scholastic journalism piece is based on shows that writing in cursive does not produce writing that is superior to printing. It got ever so slightly higher scores on syntax, but not on composition. And the groups weren't randomized to begin with, so interpretation is a bit sketchy. Not a bad study, just doesn't have results anywhere near the hype in the Scholastic piece. I see this time and again in publications like Scholastic, and it drives me nuts as teachers and parents never read the original research, and Scholastic only tends to like articles that are sexy (well, education sexy).
I think cursive is helpful, but in all honesty, I think it is a lost cause, like spelling and using although instead of while where appropriate.
:)
No need to apologize, as someone with a loved one in an LTC I understand. The facility in the town next to me has a poor reputation and I guess it has been earned as they have 170+ cases and 56 deaths. So sad ...I am obviously insanely bothered by this on multiple levels.
The facility to at least “be fair” is in Delaware and not here in NJ.
But what is going on here? I know after losing my mom in one of these facilities over a long period of time recently how poorly they can be run and how overworked the employees are. Also I hate to say it but how unskilled and underpaid some of the people can be who take care of your loved ones on a daily basis are. I’m not saying people don’t work hard or care because for me that’s all they did was bust their ass but they could only do so much.
These facilities weren’t equipped to deal with our loved seniors in normal times much less now.
But it’s truly disturbing me on the first person level to see a friend with a daughter she needs to be there for, fall ill herself because they had no protection for employees to speak of. And they want her to come to work next week. And she wants to because she has to work. So I’m sorry for the rant but it just is disturbing to see the failure on every level here. Now in mid-May.
You do realize you making me feel even worse now, right? I just pray the reason my Aunt's facility has had better success is the fact they don't or won't do the same.My brother in-law's kid (18) works part time in the kitchen of a nursing facility up in north Jersey.
My sister in-law is a nurse.
A few weeks ago, she was diagnosed with the Covid. Actually got really sick, but never sick enough to be hospitalized.
On the Friday evening we did a family Zoom happy hour. The B-I-L is downstairs, she's in bed with their 16 year-old daughter sitting in the bed next to her. She sounds like death. Somebody asks "where's Michael?" "Oh, he's at work."
After the call, everyone was on the phone, texting back and forth, utterly incredulous. My other B-I-L finds out the name of the nursing home the kid works at and calls them to say that they have a food service employee who is working while his mother is in bed with the Covid. Their response? "Oh, yes. We know."
There's nothing to be done. No laws have been broken.
There is a study showing that writing in cursive improves literacy skills? You got a link for that? I'd love to have that in my hip pocket for discussions with my faculty. Have to say I'm a bit skeptical on that one.
Many years ago when I was an elementary principal, our curriculum director, who was a brilliant educator, presented the idea idea that we consider teaching cursive from the get go and do away with teaching block lettering. She pointed to the fact that pre school children use scribble writing before learning “how to write,” as they imagine they are writing. Scribble writing is very similar physically to cursive. She also pointed to studies in Russia. Apparently Russia teaches only cursive, and there was no effect on children’s acquisition of literacy skills.
We considered this as a way of saving instructional time and instead use that time to teach/practice keyboarding skills. The developmental stage that cursive was introduced coincided pretty closely with when it was developmentally appropriate for students to learn keyboarding.
For several reasons we never adopted this approach
Is that not what I said in each post in our back and forth? Making a judgement with no understanding of the wider scope is pointless (that is where you and I sit) but to those with the knowledge of the depth of the wider scope, those numbers can be compared after adjusting. My point in each of the posts has been you and I do not have that information so we cannot make a proper judgement. That has no bearing on the people making the decisions as they should have people on their team with the information to make the adjustments/corrections for comparison. I would hope they are doing that and is the reason they are going to start to re-open.If you know how the wider testing was established, you can make a reasonable estimate of whether you are witnessing a decrease or increase in total numbers.
You keep taking what I responded to YOU as meaning the numbers are useless for everyone, even those who have the data on the wider scope. I am suggesting the 11 and 7 are useless to you and I to make a judgement on whether cases are slowing down because we do not have the information. My initial response was to your judgement of the 11 v 7 and re-opening and I am suggesting you have no idea on how to compare those two numbers to make a valid judgement. About all you can do is guess as to whether cases are slowing down or not. Same goes for me. I would hope the govt is not blindly guessing too.
https://www.medrxiv.org/content/10.1101/2020.05.02.20080036v1.full.pdf
Retrospective study on whether zinc made a significant difference when added to HCQ/AZ.
The main finding of this study is that after adjusting for the timing of zinc therapy, we found that the addition of zinc sulfate to hydroxychloroquine and azithromycin was found to associate with a decrease in mortality or transition to hospice among patients who did not require ICU level of care, but this association was not significant in patients who were treated in the ICU.
Retrospective study on whether zinc made a significant difference when added to HCQ/AZ.
The main finding of this study is that after adjusting for the timing of zinc therapy, we found that the addition of zinc sulfate to hydroxychloroquine and azithromycin was found to associate with a decrease in mortality or transition to hospice among patients who did not require ICU level of care, but this association was not significant in patients who were treated in the ICU.
https://www.evms.edu/media/evms_pub...cine/EVMS_Critical_Care_COVID-19_Protocol.pdf
Updated treatment protocol from EVMS.
Note they have suggestions for prophylaxsis and early symptomatic treatments. Note they qualifiers and this is not intended as medical advice from me.
While there is very limited data (and none specific for COVID-19), the following “cocktail” may have a role in the prevention/mitigation of COVID-19 disease. While there is no high-level evidence that this cocktail is effective; it is cheap, safe and widely available.
• Vitamin C 500 mg BID and Quercetin 250-500 mg BID
• Zinc 75-100 mg/day (acetate, gluconate or picolinate). Zinc lozenges are preferred. After 1 month, reduce the dose to 30-50 mg/day.
• Melatonin (slow release): Begin with 0.3mg and increase as tolerated to 2 mg at night
• Vitamin D3 1000-4000 u/day
Updated treatment protocol from EVMS.
Note they have suggestions for prophylaxsis and early symptomatic treatments. Note they qualifiers and this is not intended as medical advice from me.
While there is very limited data (and none specific for COVID-19), the following “cocktail” may have a role in the prevention/mitigation of COVID-19 disease. While there is no high-level evidence that this cocktail is effective; it is cheap, safe and widely available.
• Vitamin C 500 mg BID and Quercetin 250-500 mg BID
• Zinc 75-100 mg/day (acetate, gluconate or picolinate). Zinc lozenges are preferred. After 1 month, reduce the dose to 30-50 mg/day.
• Melatonin (slow release): Begin with 0.3mg and increase as tolerated to 2 mg at night
• Vitamin D3 1000-4000 u/day
Not that this is unexpected but just shows how difficult it will be for some places to get back to a “normal” and this is in SK who has such specificity in tracking, tracing etc...
From CNN:
All bars in Seoul have been ordered to close until further notice after a spike in coronavirus cases linked to nightclubs in the South Korean capital.
At a briefing Saturday, Seoul Mayor Park Won-soon said that clubs and bars would all need to shut, effective immediately.
A spike in cases: The order follows a surge in cases connected with nightclubs in Itaewon, a popular nightlife district in Seoul.
On Thursday, a 29-year-old man from the city of Yongin -- on the outskirts of Seoul -- tested positive for the virus. The person visited several clubs in Itaewon on the night of May 1 and the early hours of May 2, according to the Korea Centers for Disease Control and Prevention (KCDC).
Since then, 40 others believed to be connected to the case have tested positive. Of those, 27 are from Seoul.
Tracking partygoers: South Korea has not introduced a nationwide lockdown, but has brought in additional measures to control the coronavirus outbreak. At nightclubs, for instance, people must provide their full name and phone number before entry.
According to Park, 1,946 names were listed on the registry books of the three clubs the 29-year-old visited. Only 647 of those people have been identified.
More cases possible: Kwon Joon-wook, deputy director of the KCDC, also said there may have been more than one source of infection behind the nightclub outbreak. Some of the people who have been confirmed positive visited clubs on different nights from the 29-year-old.
“We’ve put in much efforts and made a lot of sacrifices," Park added Saturday. "Are we just to let this all go to waste because of few people’s carelessness?”
A setback in South Korea: Before the nightclub-related spike, new coronavirus cases had been trending down in the country. On Tuesday, South Korea reported its lowest number of new cases for more than two months.
According to Johns Hopkins University, South Korea has reported more than 10,800 coronavirus cases and 256 deaths. The vast majority of South Korea's cases have recovered, the KCDC said earlier this week.
They've had a couple of flare-ups and been able to handle them, so far, with very rapid testing/tracing of anyone involved and/or in contact with anyone infected (including asymptomatic contacts) - let's see how they do on this one. What they did in response to a Seoul office building outbreak is truly impressive, but an infected person visiting multiple nightclubs will likely be more challenging.
https://wwwnc.cdc.gov/eid/article/26/8/20-1274_article
https://www.evms.edu/media/evms_pub...cine/EVMS_Critical_Care_COVID-19_Protocol.pdf
Updated treatment protocol from EVMS.
Note they have suggestions for prophylaxsis and early symptomatic treatments. Note they qualifiers and this is not intended as medical advice from me.
While there is very limited data (and none specific for COVID-19), the following “cocktail” may have a role in the prevention/mitigation of COVID-19 disease. While there is no high-level evidence that this cocktail is effective; it is cheap, safe and widely available.
• Vitamin C 500 mg BID and Quercetin 250-500 mg BID
• Zinc 75-100 mg/day (acetate, gluconate or picolinate). Zinc lozenges are preferred. After 1 month, reduce the dose to 30-50 mg/day.
• Melatonin (slow release): Begin with 0.3mg and increase as tolerated to 2 mg at night
• Vitamin D3 1000-4000 u/day
I've been following their treatment protocols for a while (posted an earlier version a few weeks back). It's certainly interesting and I wonder about a couple of things:
1) How similar is this to what is being done elsewhere, and
2) They are claiming very good results but I haven't seen any published data to back that up. Would be really nice to see some numbers.
This is a pretty strong claim they throw in without anything to back it up:
"Our long-standing and more recent experiences show consistently successful treatment if traditional therapeutic principles of early and aggressive intervention is achieved, before the onset of advanced organ failure."
Just wanted to add to what I witnessed this past week as it relates to long term care facilities. And this is just one place where I had the misfortune of my mother being at for a while unfortunately.
So I have a friend who works there as a nurse. She had zero experience, former school teacher and just got her certification for nursing there, whatever that is. They had zero PPE there until recently. We mailed her homemade cloth masks. As sure as shit she got sick the other day. They finally set her up to get tested after. Of course she is positive. This was Wednesday.
Nursing home wants her to use PTO this week to cover her absence.
They also want her to return to work next week. Next week! No follow up test, just if you can taste and smell again. But if not you won’t get paid.
So what is she going to do? She has a daughter Go back to work as a per diem nurse who’s facility gives zero shits about it’s employees.
So that’s just one person’s account at a long term care facility. No wonder it spreads like wildfire.
Zero PPE is just so irresponsible, I can't fathom it. As for her return to work, she should check with the state recommendations from the Department of Health on guidelines for return. At our facility, the general rule is seven days from diagnosis or three days after your last recorded symptom...minimum. You mentioned per diem, so I am assuming that is her employment status. As a per diem, she does not accrue sick time and must rely on her PTO for that one week...one of the unfortunate consequences of a per diem nurse. One trades increase in salary, flexibility of schedule for no benefits (sick time, holiday time) or guaranteed work. I wish her the best, but she should check with the state DOH for some guidance. The taste/smell preclusion for return to work is an odd and new one. I have friends who havent had taste/smell return for a month and a half.
My brother in-law's kid (18) works part time in the kitchen of a nursing facility up in north Jersey.
My sister in-law is a nurse.
A few weeks ago, she was diagnosed with the Covid. Actually got really sick, but never sick enough to be hospitalized.
On the Friday evening we did a family Zoom happy hour. The B-I-L is downstairs, she's in bed with their 16 year-old daughter sitting in the bed next to her. She sounds like death. Somebody asks "where's Michael?" "Oh, he's at work."
After the call, everyone was on the phone, texting back and forth, utterly incredulous. My other B-I-L finds out the name of the nursing home the kid works at and calls them to say that they have a food service employee who is working while his mother is in bed with the Covid. Their response? "Oh, yes. We know."
There's nothing to be done. No laws have been broken.
Having a sick member in the household should not prevent him from working. Otherwise there would be no healthcare workers available as we pretty much all have all been exposed, multiple, multiple times. I have an ER buddy who tells me he takes a "Covid Shower" on a daily basis. Your nephew and the facility should be mindful and screening for symptoms though. The importance of your SIL self-quarantining until she is symptom free (typically 3 days) is the biggest help. The fact her daughter was sitting on the bed with her makes your niece at risk for contracting the virus.
You do realize you making me feel even worse now, right? I just pray the reason my Aunt's facility has had better success is the fact they don't or won't do the same.
My wife's aunt, who lived in Pittsburgh, was diagnosed with Alzheimer's about five years ago. It moved pretty quickly at the onset. Four years ago we moved her out of her ancestral home and into a memory care unit in East Brunswick.
She died on March 14th, following no discernible illness. We had to fly her, somewhat circuitously, out to Western PA, then my wife and I drove out there to bury her. That was the weekend everything shut down; we were on the PATP coming home on the Sunday when NJ went into lockdown.
I've become convinced that she was an early Covid victim. Alzheimer's patients are prone to stroke, which has been found to be an irregular manifestation of C-19. They didn't test her, because it was too early in the epidemic. But ya gotta wonder.
Having a sick member in the household should not prevent him from working. Otherwise there would be no healthcare workers available as we pretty much all have all been exposed, multiple, multiple times. I have an ER buddy who tells me he takes a "Covid Shower" on a daily basis. Your nephew and the facility should be mindful and screening for symptoms though. The importance of your SIL self-quarantining until she is symptom free (typically 3 days) is the biggest help. The fact her daughter was sitting on the bed with her makes your niece at risk for contracting the virus.
And, by extension, her brother. That was our concern. My sister-in-law wasn't really quarantining; she was continually exposing the entire family.
When Tyler went back to school in the spring of his 4th grade year, they were learning long division. So, at home, I taught him long division in under an hour, just doing it on paper. He gets into school, they spend 2 weeks learning how to estimate results when dividing? Really?New math was essentially an effort to focus less on calculation and accuracy as the goals of math instruction and to focus more on understanding the underlying concepts and ideas that make up mathematics. Hence, less time memorizing multiplication tables and more time looking at patterns and sets of numbers that underlie multiplication. More time on estimating what results look reasonable and less time on correcting errors in calculation. And with the advent of calculators, even less time on calculation. Kids more likely to work in groups and problem solve and novel approaches to things like long division. In New Zealand, we don't even teach kids division by fractions (because who ever actually does that stuff?).
The underlying problem of new math is that in the real world it's important to get the answer right, and if you have to stop half way through a problem to work out what 6 times 8 is, the cognitive load throws you off the problem. Thus, new math, and it's descendants, were well-intentioned and had some good ideas, but common sense gave way to ideological purity and it pretty much went haywire.
@rutgersguy1 saw it too...May have missed this one, but good news out of Hong Kong, as a randomized, controlled, open label study comparing a triplet antiviral cocktail of lopinavir–ritonavir, and ribavirin with interferon beta-1b, showed that this combo was safe and superior to lopinavir–ritonavir alone in shortening virus shedding, alleviating symptoms, and facilitating discharge of patients with mild to moderate COVID-19. These are the kinds of patients who benefitted from remdesivir in its recent trial.
Great to have more options, but we still need drugs to treat more serious cases. Nobody died in the study, so it's not clear to me if these were simply people who would have recovered anyway (or if even the lopinavir-ritonavir "control" would have prevented people from progressing to serious illness). I didn't see that discussed in the paper, but might have missed it.
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)31042-4/fulltext
Study out of Hong Kong that a triple antiviral cocktail and MS drug help patients recover more quickly. Patients with mild/moderate symptoms and given withing 7 days of testing positive.
From the article:
Dr. Kwok-Yung Yuen at Hong Kong University and colleagues tested the HIV drug combination of ritonavir and lopanivir along with the general antiviral drug ribavirin and a multiple sclerosis drug called beta interferon.
Patients in the study all had mild to moderate symptoms and were treated within seven days of testing positive. Some doctors think treating patients earlier in the course of the infection might be better.
Yuen's team gave some patients only the HIV drug combination, often sold under the brand name Kaletra. Other were randomly assigned to get the lopinavir-ritonavir combination plus the antiviral drug ribavirin and injections of beta interferon.
The patients who got the cocktail tested negative for coronavirus after seven days on average. Those who just got the HIV drugs were positive on average for 12 days, the team reported in the Lancet medical journal.
The patients given the cocktail also felt better quicker -- within four days.
"Early triple antiviral therapy was safe and superior to lopinavir-ritonavir alone in alleviating symptoms and shortening the duration of viral shedding and hospital stay in patients with mild to moderate COVID-19," the researchers wrote.
There were few side effects, they added.
https://www.cnn.com/2020/05/08/health/coronavirus-triple-therapy-hong-kong-health/index.html
Just wanted to add to what I witnessed this past week as it relates to long term care facilities. And this is just one place where I had the misfortune of my mother being at for a while unfortunately.
So I have a friend who works there as a nurse. She had zero experience, former school teacher and just got her certification for nursing there, whatever that is. They had zero PPE there until recently. We mailed her homemade cloth masks. As sure as shit she got sick the other day. They finally set her up to get tested after. Of course she is positive. This was Wednesday.
Nursing home wants her to use PTO this week to cover her absence.
They also want her to return to work next week. Next week! No follow up test, just if you can taste and smell again. But if not you won’t get paid.
So what is she going to do? She has a daughter Go back to work as a per diem nurse who’s facility gives zero shits about it’s employees.
So that’s just one person’s account at a long term care facility. No wonder it spreads like wildfire.
Most nursing homes are more real estate ventures than medical facilities.
You have to be very careful in choosing these facilities for your loved ones. Places that provide a continuum of care or have legal agreements with hospitals are essential.
First FDA Emergency Use Authorization for an antigen test, which detects the virus via detection of a viral protein (an "antigen" or foreign body) vs. an analysis of the viral RNA as in the PCR test. These tests are fantastic for speed/simplicity, but still have even higher false negative rates than current PCR-nucleic acid tests, which can have as high as 20% false negatives, due to lack of sensitivity, early in an infection (but false negatives are much lower when symptomatic due to greater viral loads). So a negative test should not mean someone should feel they're virus free, whereas a positive result is almost never wrong.
Need the sensitivity to be at least as good as PCR tests before widely deploying these IMO - and once they are (and we ought to be able to get there), they'll be far faster and far more available and should be doable at home. But to be used in close to real time for events and such the false negative rate has to be close to zero - not sure how long it will take to get there. First link is to the new test story and second one is to a ore in-depth discussion of antigen testing for the virus.
https://www.cnbc.com/2020/05/09/fda...tigen-test-to-rapidly-detect-coronavirus.html
https://www.npr.org/sections/health...on-coronavirus-test-raises-hopes-and-concerns
Need the sensitivity to be at least as good as PCR tests before widely deploying these IMO - and once they are (and we ought to be able to get there), they'll be far faster and far more available and should be doable at home. But to be used in close to real time for events and such the false negative rate has to be close to zero - not sure how long it will take to get there. First link is to the new test story and second one is to a ore in-depth discussion of antigen testing for the virus.
https://www.cnbc.com/2020/05/09/fda...tigen-test-to-rapidly-detect-coronavirus.html
https://www.npr.org/sections/health...on-coronavirus-test-raises-hopes-and-concerns
When Tyler went back to school in the spring of his 4th grade year, they were learning long division. So, at home, I taught him long division in under an hour, just doing it on paper. He gets into school, they spend 2 weeks learning how to estimate results when dividing? Really?
The problem is since elementary schools have mostly done away with homogeneous grouping, all students are expected to learn at the same pace. Your son is likely bright and a fast learner in math, I can guarantee you that out of 25 kids in the class not all would have learned long division in an hour, especially with one teacher for all 25. I understand the reasons why grouping practices were changed but there’s definitely negative consequences including dumbing down the curriculum pace to the middle and making faster learners dislike school. There are reasonable alternatives that make sense and allows for students to learn at their pace with others of similar abilities and avoid the concerns of homogeneous grouping.
It's not just the elderly and it's not just about the health care system - to me, it's much more about preventing 1MM or more additional US deaths over the next 6-18 months, assuming we open things up and allow the US to move towards herd immunity, which is what some seem to want.
There are 83MM people in the US aged 45-64 and the total death rate for these people from COVID in NYC is 1540 per 1MM, which translates to 127K deaths of people in the US between 45 and 64, assuming the NYC death rates are similar for what the US's will be, which should eventually be the case, even if it's not now, as there should be no reason NYC people would be more likely to die from the virus than anyone else, unless there's some demographic or health care system reason, which could be factors, but are likely minor ones. But NYC only has about 20-25% infected so far (20% as of 4/30, but the first two results were closer to 25%, so since more people have been infected since the antibody study, let's take the 25% number infected right now in NYC. So one needs to multiply that 25% infected by 2.4X to get the total number of deaths for 60% being infected or very close to herd immunity. That would up the number to 305K dead between 45-64.
There are 30MM people in the US 65-74 and the NYC death rates for them is 5020 per 1MM, which translates to 150K deaths of people in the US between 65 and 74, assuming the NYC death rates are similar for what the US's will be. But NYC only has about 25% infected so far, so one needs to multiply that number by 2.4X to get the total number of deaths for 60% being infected or very close to herd immunity. That would up the number to 360K dead between 65-74.
There are 19MM people in the US over 75 and the NYC death rates for them is 12,620 per 1MM, which translates to 240K deaths of people in the US for people 75 and over, assuming the NYC death rates are similar for what the US's will be. But NYC only has about 25% infected so far, so one needs to multiply that number by 2.4X to get the total number of deaths for 60% being infected or very close to herd immunity. That would up the number to 576K dead between 45-64.
And finally, there are 109MM people in the US 19-44 and the NYC death rates for them is 168 per 1MM, which translates to "only" 18K deaths of people in the US between 19 and 44, assuming the NYC death rates are similar for what the US's will be. But NYC only has about 25% infected so far, so one needs to multiply that number by 2.4X to get the total number of deaths for 60% being infected or very close to herd immunity. That would up the number to 43K dead between 19-44. In a typical flu season, about 3400 people from 18-49 (didn't have 19-44) die from the flu and that number would obviously be less (3000?) for 18-44.
That's about 1.28MM total US dead, which is a fair amount greater than the 950K total dead the Wharton model had last week, if we stopped all interventions/social distancing and went to herd immunity over the next 6 to maybe 18 months (because the rate of spread will be much slower in low population density areas). The calcs above assume no interventions and no treatment/cure/vaccine and 60% of the US becoming infected at herd immunity and dying at rates we see in NYC now. The calcs also assume the NYC ~25% infected number, from antibody testing is correct. There could obviously be errors in all of those assumptions, but even if the deaths were simply just the 950K deaths in the Wharton model that's still an insane level of deaths over the next 18 months or so.
Also, here's a reality check on the numbers above. NYC right now, has 19,700 deaths in 25% of its population of 8.5MM (2.12MM infected) so the infection fatality number right now is 0.93%. If that overall 0.93% number held for the 60% of 330MM that would eventually become infected, that would be 1.84MM US deaths. Even if we went with NY State numbers of 26K deaths in 15% of the population with antibodies out of 20MM, that's an IFR of 0.86%, which would translate to 1.70MM US deaths. We better hope there are a lot more people with antibodies in NYC/NY or that there is something unusual about NYC/NY death rates or that we have a real treatment (plasma/engineered antibodies?) soon or that transmission rates end up being slower than expected in less densely populated areas with less interventions, giving more time for a cure/vaccine. Also, keep in mind that true infection rates in the rest of the US are likely only around 3-5%, given the much slower outbreaks in much less densely populated areas - this is where a Federal antibody testing program would be nice.
These kinds of potential deaths are why we need to get transmission rates down to much lower levels, such that death rates will stay at low levels, especially until we have a treatment/cure/vaccine. And the only way to do that is aggressive testing, tracing, and isolating to quickly detect and snuff out flare-ups, along with wearing masks in public and at least moderate social distancing to prevent the flare-ups in the first place and minimize them when they occur. This is the direction the NE Region (NY, NJ, CT, RI, MA, PA, DE) are heading as well as CA, WA, and OR, which combined are about 1/3 of the US population (106MM) but not the direction much of the rest of the country is headed.

US Population By Age (2018)

Sometimes I wonder if I'm missing something really important, but nothing obvious comes to mind. Hey @SkilletHead2 - being a numbers/math guy, who hasn't been immersed in this, as far as I can tell - can you check me here? Thanks.
This JHU "academic comment" reinforces what I was saying in this post. We're nowhere near herd immunity yet (they think that's near 70%), especially in the US at large with maybe 2-4% actually infected (vs. ~15% in NY and maybe 20-25% in NYC), so trying to "move towards herd immunity" is a really bad idea that, without any cure/vaccine will slowly lead to >500K US deaths and possibly many more than that (like the 950K in the Wharton model or even more as I outlined is possible above).
Whether it's 500K or a million, does that really matter? Do we want to even go anywhere near there? I certainly don't and we've seen other countries figure out how to greatly slow transmissions/deaths, but we don't seem to wan to go that route except in some states (especially in the NE that have been hit hardest so far).
https://coronavirus.jhu.edu/from-ou...ty-against-covid-19-a-dangerous-misconception
We have listened with concern to voices erroneously suggesting that herd immunity may “soon slow the spread”1 of COVID-19. For example, Rush Limbaugh2 recently claimed that “herd immunity has occurred in California.” As infectious disease epidemiologists, we wish to state clearly that herd immunity against COVID-19 will not be achieved at a population level in 2020, barring a public health catastrophe.
Although more than 2.5 million confirmed cases of COVID-19 have been reported worldwide, studies suggest that (as of early April 2020) no more than 2-4%3–5 of any country’s population has been infected with SARS-CoV-2 (the coronavirus that causes COVID-19). Even in hotspots like New York City that have been hit hardest by the pandemic, initial studies suggest that perhaps 15-21%6,7 of people have been exposed so far. In getting to that level of exposure, more than 17,500 of the 8.4 million people in New York City (about 1 in every 500 New Yorkers) have died, with the overall death rate in the city suggesting deaths may be undercounted and mortality may be even higher.8
Some have entertained the idea of “controlled voluntary infection,”9 akin to the “chickenpox parties” of the 1980s. However, COVID-19 is 100 times more lethal than the chickenpox. For example, on the Diamond Princess cruise ship, the mortality rate among those infected with SARS-CoV-2 was 1%. Someone who goes to a “coronavirus party” to get infected would not only be substantially increasing their own chance of dying in the next month, they would also be putting their families and friends at risk. COVID-19 is now the leading cause of death in the United States, killing almost 2,000 Americans every day.8 Chickenpox never killed more than 150 Americans in a year.9
To reach herd immunity for COVID-19, likely 70% or more of the population would need to be immune. Without a vaccine, over 200 million Americans would have to get infected before we reach this threshold. Put another way, even if the current pace of the COVID-19 pandemic continues in the United States – with over 25,000 confirmed cases a day – it will be well into 2021 before we reach herd immunity. If current daily death rates continue, over half a million Americans would be dead from COVID-19 by that time.
I keep hearing about spikes in SK, and then I look at worldometer and see 12 new cases.Not that this is unexpected but just shows how difficult it will be for some places to get back to a “normal” and this is in SK who has such specificity in tracking, tracing etc...
From CNN:
All bars in Seoul have been ordered to close until further notice after a spike in coronavirus cases linked to nightclubs in the South Korean capital.
At a briefing Saturday, Seoul Mayor Park Won-soon said that clubs and bars would all need to shut, effective immediately.
A spike in cases: The order follows a surge in cases connected with nightclubs in Itaewon, a popular nightlife district in Seoul.
On Thursday, a 29-year-old man from the city of Yongin -- on the outskirts of Seoul -- tested positive for the virus. The person visited several clubs in Itaewon on the night of May 1 and the early hours of May 2, according to the Korea Centers for Disease Control and Prevention (KCDC).
Since then, 40 others believed to be connected to the case have tested positive. Of those, 27 are from Seoul.
Tracking partygoers: South Korea has not introduced a nationwide lockdown, but has brought in additional measures to control the coronavirus outbreak. At nightclubs, for instance, people must provide their full name and phone number before entry.
According to Park, 1,946 names were listed on the registry books of the three clubs the 29-year-old visited. Only 647 of those people have been identified.
More cases possible: Kwon Joon-wook, deputy director of the KCDC, also said there may have been more than one source of infection behind the nightclub outbreak. Some of the people who have been confirmed positive visited clubs on different nights from the 29-year-old.
“We’ve put in much efforts and made a lot of sacrifices," Park added Saturday. "Are we just to let this all go to waste because of few people’s carelessness?”
A setback in South Korea: Before the nightclub-related spike, new coronavirus cases had been trending down in the country. On Tuesday, South Korea reported its lowest number of new cases for more than two months.
According to Johns Hopkins University, South Korea has reported more than 10,800 coronavirus cases and 256 deaths. The vast majority of South Korea's cases have recovered, the KCDC said earlier this week.
Shows how vigilant they are to shut things down even with such low #'s.
I took typing at night 11th or 12th grade, never used it, typed a couple things while getting my Chem E degree, but really lost any capability using it. Anyway, fast forward to after my Comp Sci degree and working at my first job, where I'm doing the whole hunt and peck method to program. At some point during my first year I realized this would go much better if I knew how to type, so I pulled out the old course book I had, retaught myself all the positioning, then on one particular day switched over and forced myself to use it, absolutely refusing to hunt and peck anymore. Best decision I ever made, 'cause now I can fly on the keyboard as I write code. No one in my office can do that. When people come over to my desk asking for something adhoc concerning a client, usually around their data, they know I can write the SQL queries on the fly and give them an answer almost immediately instead of going back to their desk and waiting.I should qualify that by saying my "printing" half looks like cursive, as it's really sloppy and letters run into each other in my own kind of shorthand, including many abbreviations I use.
Took typing in 11th grade and have said for years it was the most valuable course I took in HS also! Teacher said I'd make a fine secretary someday.
And what about the residents who are highly likely to be exposed? That's borderline criminal. Someone on the CE Board just had a similar situation, they got the state involved and the doctors were put in their place. I wonder if something similar could be done in Delaware for this place.Nursing home wants her to use PTO this week to cover her absence.
They also want her to return to work next week. Next week! No follow up test, just if you can taste and smell again. But if not you won’t get paid.
So what is she going to do? She has a daughter Go back to work as a per diem nurse who’s facility gives zero shits about it’s employees.
Reservations for the beach? Interesting to see how that will play out in Spain.
https://www.cnn.com/travel/article/spanish-beach-reservations/index.html
https://www.cnn.com/travel/article/spanish-beach-reservations/index.html
this is a must read
‘Finally, a virus got me.’ Scientist who fought Ebola and HIV reflects on facing death from COVID-19 | Science | AAAS
https://www.sciencemag.org/news/202...-ebola-and-hiv-reflects-facing-death-covid-19
full version:
‘Finally, a virus got me.’ Scientist who fought Ebola and HIV reflects on facing death from COVID-19 | Science | AAAS
https://www.sciencemag.org/news/202...-ebola-and-hiv-reflects-facing-death-covid-19
full version:
Believe or not, Spank, a lot of schools don't teach long division at all anymore. Which is a shame because long division contains two of the most practical elements of doing math: generating initial estimates prior to doing the actual work, and checking your answer to see if it is reasonable. Kids with good math ability pick these two ideas up easily and expand on them as they grow. I'm sure Tyler is that kind of kid. But most kids are not. They really struggle with this concept and need a lot of help on it. But, if you can get them to have a decent appreciation of these ideas, it is super helpful throughout the rest of math and in life. And so, schools teach it. They often don't teach it well, but they try. You have to understand that most elementary school teachers are scared stiff of math.When Tyler went back to school in the spring of his 4th grade year, they were learning long division. So, at home, I taught him long division in under an hour, just doing it on paper. He gets into school, they spend 2 weeks learning how to estimate results when dividing? Really?
One of my former students, who is from Belarus, has two amazingly bright and talented boys. She's an educational psychologist, like me (trained by me). We were talking about lockdown the other day. She has taken her boys through two years of their local (very high SES) school curriculum. She thinks that the lockdown is going to cause some kids to soar (who aren't being held back by their classmates) while others will have become much much better at World of Warcraft or Frozen 2. I think she's right. Of course, her son, at age 11, played the violin at Carnegie Hall and speaks four languages (the mom speaks six).
(And btw, on that other issue we are discussing concerning the Middle East, I hope you know I'm just ragging on you, but we really should come up with some real rules, and I'm all for making them rigorous and adhering to them. In which case, you could argue my posts and yours should go.)
I’m glad you’re around. :Beers:Believe or not, Spank, a lot of schools don't teach long division at all anymore. Which is a shame because long division contains two of the most practical elements of doing math: generating initial estimates prior to doing the actual work, and checking your answer to see if it is reasonable. Kids with good math ability pick these two ideas up easily and expand on them as they grow. I'm sure Tyler is that kind of kid. But most kids are not. They really struggle with this concept and need a lot of help on it. But, if you can get them to have a decent appreciation of these ideas, it is super helpful throughout the rest of math and in life. And so, schools teach it. They often don't teach it well, but they try. You have to understand that most elementary school teachers are scared stiff of math.
One of my former students, who is from Belarus, has two amazingly bright and talented boys. She's an educational psychologist, like me (trained by me). We were talking about lockdown the other day. She has taken her boys through two years of their local (very high SES) school curriculum. She thinks that the lockdown is going to cause some kids to soar (who aren't being held back by their classmates) while others will have become much much better at World of Warcraft or Frozen 2. I think she's right. Of course, her son, at age 11, played the violin at Carnegie Hall and speaks four languages (the mom speaks six).
(And btw, on that other issue we are discussing concerning the Middle East, I hope you know I'm just ragging on you, but we really should come up with some real rules, and I'm all for making them rigorous and adhering to them. In which case, you could argue my posts and yours should go.)
For the most part, I agree. But in reality, the %'s aren't really the issue; it's the actual number of cases. But that is a bit clouded as well, since we know that some people can get this, get over it, and perhaps never know they had it. Which is why the broader testing is helpful. But even for us, with limited knowledge of the specifics, we can say that if you expand the testing greatly, you should expect the % to drop. Nothing wrong with that.Is that not what I said in each post in our back and forth? Making a judgement with no understanding of the wider scope is pointless (that is where you and I sit) but to those with the knowledge of the depth of the wider scope, those numbers can be compared after adjusting. My point in each of the posts has been you and I do not have that information so we cannot make a proper judgement. That has no bearing on the people making the decisions as they should have people on their team with the information to make the adjustments/corrections for comparison. I would hope they are doing that and is the reason they are going to start to re-open.
You keep taking what I responded to YOU as meaning the numbers are useless for everyone, even those who have the data on the wider scope. I am suggesting the 11 and 7 are useless to you and I to make a judgement on whether cases are slowing down because we do not have the information. My initial response was to your judgement of the 11 v 7 and re-opening and I am suggesting you have no idea on how to compare those two numbers to make a valid judgement. About all you can do is guess as to whether cases are slowing down or not. Same goes for me. I would hope the govt is not blindly guessing too.
This JHU "academic comment" reinforces what I was saying in this post. We're nowhere near herd immunity yet (they think that's near 70%), especially in the US at large with maybe 2-4% actually infected (vs. ~15% in NY and maybe 20-25% in NYC), so trying to "move towards herd immunity" is a really bad idea that, without any cure/vaccine will slowly lead to >500K US deaths and possibly many more than that (like the 950K in the Wharton model or even more as I outlined is possible above).
Whether it's 500K or a million, does that really matter? Do we want to even go anywhere near there? I certainly don't and we've seen other countries figure out how to greatly slow transmissions/deaths, but we don't seem to wan to go that route except in some states (especially in the NE that have been hit hardest so far).
https://coronavirus.jhu.edu/from-ou...ty-against-covid-19-a-dangerous-misconception
We have listened with concern to voices erroneously suggesting that herd immunity may “soon slow the spread”1 of COVID-19. For example, Rush Limbaugh2 recently claimed that “herd immunity has occurred in California.” As infectious disease epidemiologists, we wish to state clearly that herd immunity against COVID-19 will not be achieved at a population level in 2020, barring a public health catastrophe.
Although more than 2.5 million confirmed cases of COVID-19 have been reported worldwide, studies suggest that (as of early April 2020) no more than 2-4%3–5 of any country’s population has been infected with SARS-CoV-2 (the coronavirus that causes COVID-19). Even in hotspots like New York City that have been hit hardest by the pandemic, initial studies suggest that perhaps 15-21%6,7 of people have been exposed so far. In getting to that level of exposure, more than 17,500 of the 8.4 million people in New York City (about 1 in every 500 New Yorkers) have died, with the overall death rate in the city suggesting deaths may be undercounted and mortality may be even higher.8
Some have entertained the idea of “controlled voluntary infection,”9 akin to the “chickenpox parties” of the 1980s. However, COVID-19 is 100 times more lethal than the chickenpox. For example, on the Diamond Princess cruise ship, the mortality rate among those infected with SARS-CoV-2 was 1%. Someone who goes to a “coronavirus party” to get infected would not only be substantially increasing their own chance of dying in the next month, they would also be putting their families and friends at risk. COVID-19 is now the leading cause of death in the United States, killing almost 2,000 Americans every day.8 Chickenpox never killed more than 150 Americans in a year.9
To reach herd immunity for COVID-19, likely 70% or more of the population would need to be immune. Without a vaccine, over 200 million Americans would have to get infected before we reach this threshold. Put another way, even if the current pace of the COVID-19 pandemic continues in the United States – with over 25,000 confirmed cases a day – it will be well into 2021 before we reach herd immunity. If current daily death rates continue, over half a million Americans would be dead from COVID-19 by that time.
Summary:
I'm officially confused now, as the epidemiologists are now all over the map on future transmissions and deaths, with regard to how far do we have to go to reach herd immunity, which has a huge impact on total infections, hospitalizations and, obviously deaths, with models now ranging from herd immunity (where the outbreak fizzles/stops on its own) being anywhere from 10-20% to 40% to 60-70%, when most were saying 50-80% for quite awhile. Some previous posts discussing the details below are linked below from the Wharton Model, IHME and my own thoughts, plus the JHU comment is above, (partly to put them in one place for my own sanity, lol).
This plus some other variables would probably put the range of US deaths anywhere from 150K to >1MM. These are the ranges of deaths (and infections) we'd reach very slowly (18 months?) with aggressive interventions in densely populated areas or in very sparsely populated areas without interventions or much more quickly (6 months?) in densely populated areas without interventions. All of these models/calcs assume no cure/vaccine (i.e., generally current deaths per infection, which could obviously greatly reduce deaths.
While it would be fantastic to have herd immunity be at a much lower infection level, hugely cutting potential deaths, this kind of disagreement and uncertainty make decision-making on a path forward even harder than it has been. Personally, I'd be inclined to still want to follow the South Korea plan, like the NE US/West Coast are, i.e., aggressive testing, tracing, and isolating with continued mask-wearing and social distancing in order to contain flare-ups while we phase in reopening our economy and life, just in case the assumptions/models suggesting much lower herd immunity levels are possible are wrong - at least until we have a bona fide treatment/functional cure (by late summer with antibodies?) or vaccine.
Details:
- We have the Wharton estimates from about a week ago of 950K eventually (over the next 12-18 months) dead in the US if we open back up and significantly relax social distancing (details/links in the 3rd post below); they also have scenarios with anywhere from 116K-950K total US deaths depending on how much we loosen controls and open things up and how effective our social distancing is. This was the article that also compared health impacts and economic impacts, including unemployment levels for the various model runs/assumptions.
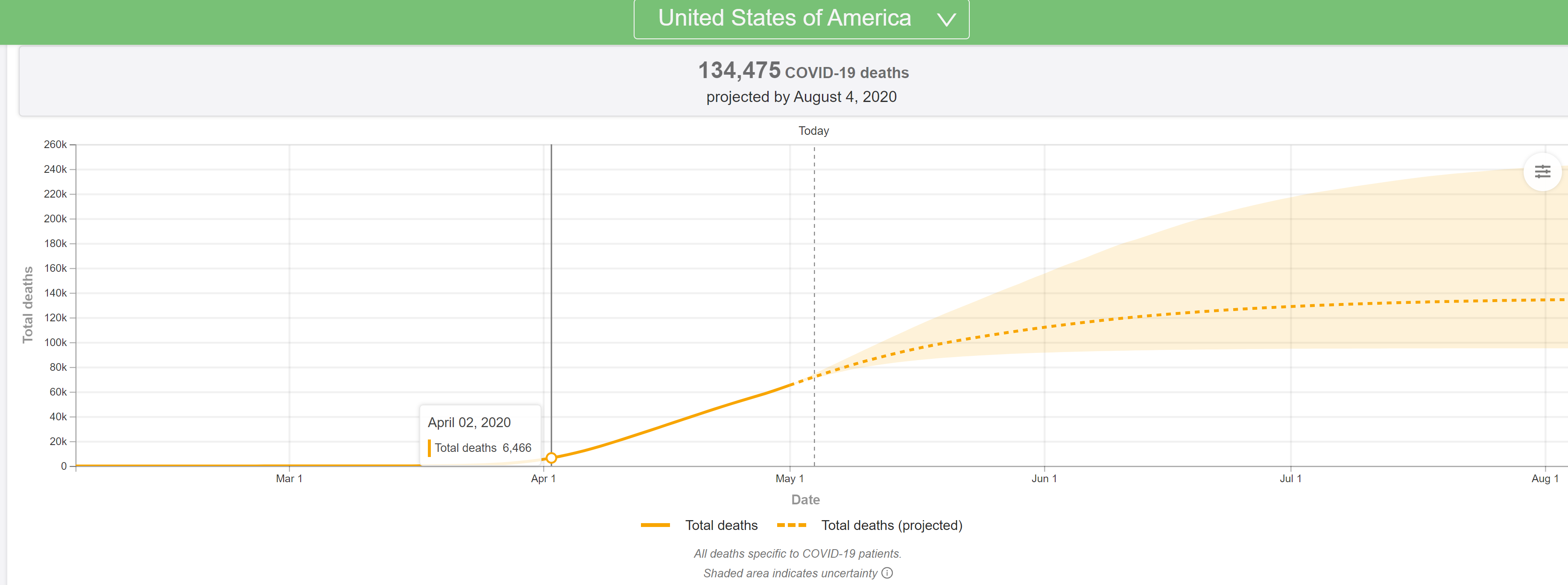
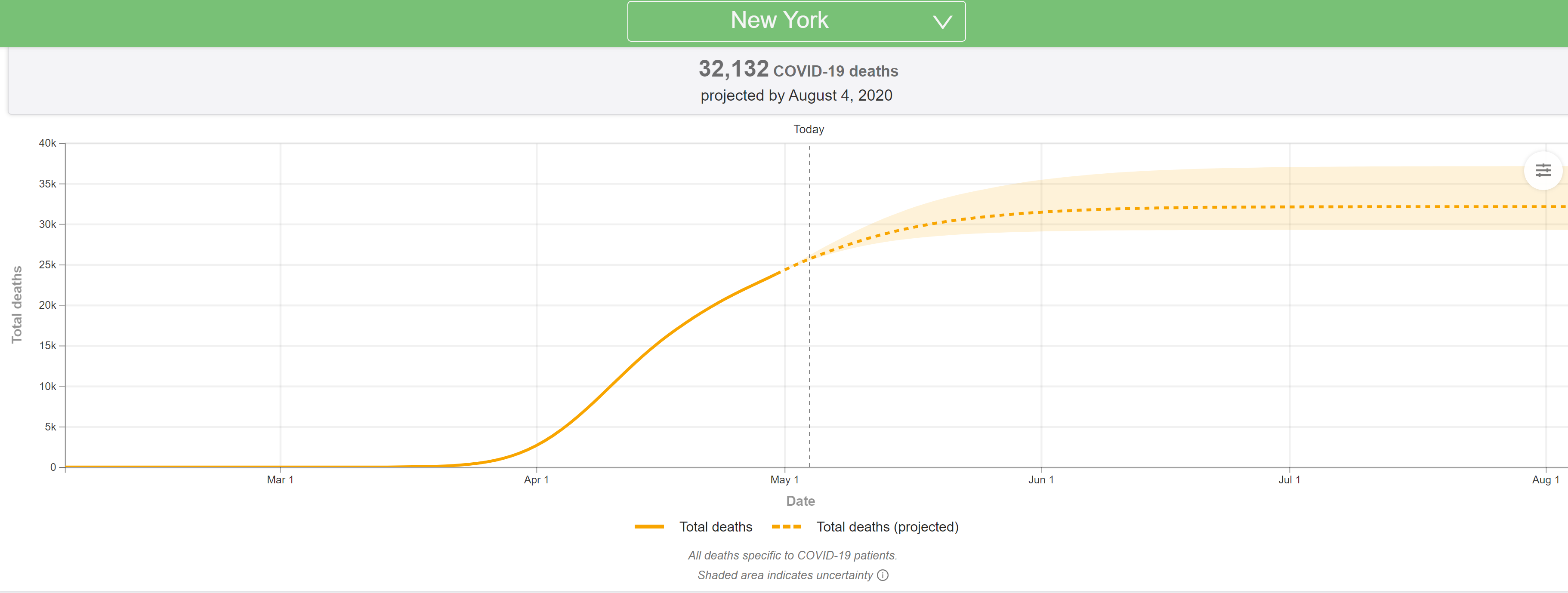
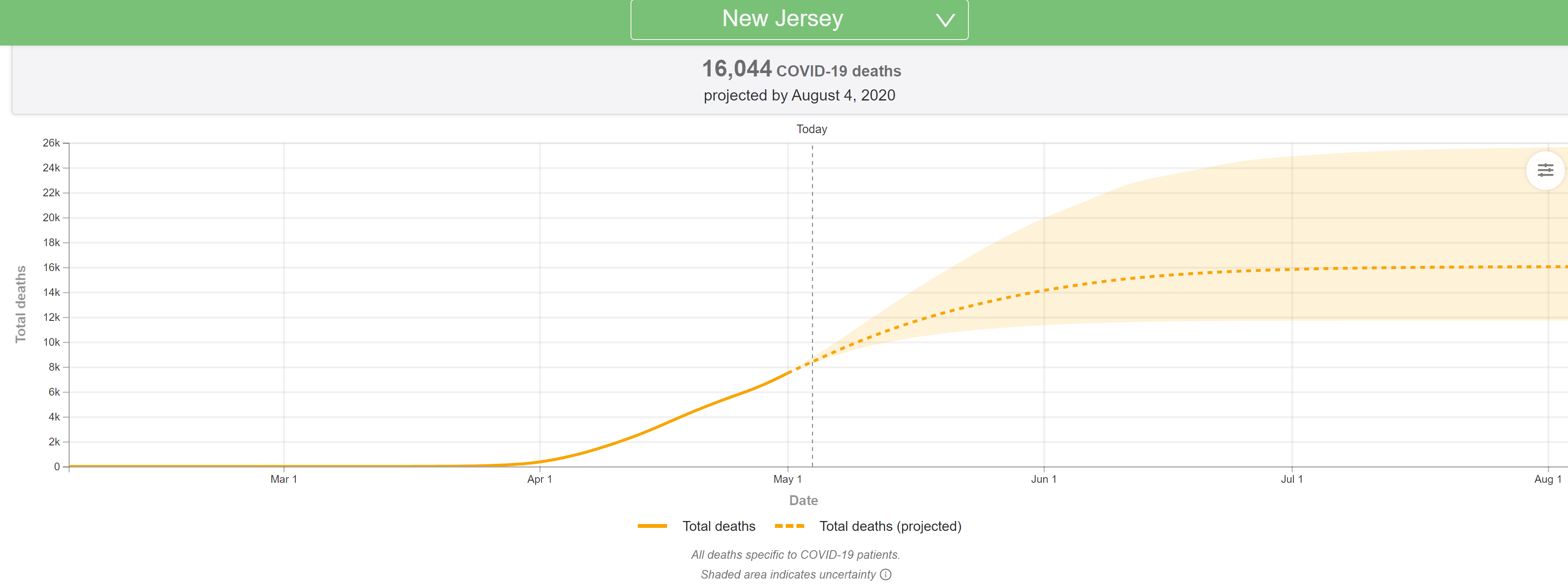
- We also have the latest IHME/U of Washington model, which was significantly revised on 5/4 to reflect much slower declines in deaths in hotspot locations and to reflect predicted increases in deaths in areas opening up and reducing social distancing, with their prediction of US deaths from this "first wave" going from 72K by the end of May to 134K by the end of July. They have not predicted overall US deaths for the entire pandemic; details/links in the 2nd post below.
- The post above (including links) from Johns Hopkins predicts we'll see >500K US deaths over the next 18 months as we steadily reach ~70% infected (herd immunity). This "academic comment" came out today, possibly in response to the two preprints discussed below, each of which argues that herd immunity levels could be far below 70% (10-40% even). This and the Wharton model were in general agreement with what I've been thinking (~1MM deaths in the US being very possible, overall), as per the first post below.
- We now have a preprint of a paper from Britton et al (Swedish) predicting that the actual herd immunity level where the outbreak fizzles/stops could be as low as 43% of the population infected, instead of the "classical" herd immunity number of 60-70% of the population infected. They're assuming the population is not "homogeneously mixed" and if the very social superspreaders all get it early (which they think should happen), then transmission rates will slow down and fizzle out at a much lower herd immunity level of about 43%.
- https://arxiv.org/pdf/2005.03085.pdf
- "Standard," epidemiology models say that if the R0 is 2.2, herd immunity is achieved at 54% of the population infected, while if the R0 is 5.7 (as some have postulated), herd immunity would require 82% of the population being infected. Huge difference, obviously.
- https://wwwnc.cdc.gov/eid/article/26/7/20-0282_article
- For an area like NYC with 20-25% infected, as per antibody testing, this would mean there isn't nearly as far to go to reach herd immunity; for most of the rest of the US and the world, outside of the worst hotspots, estimates are more like 2-5% infected so far.
- A big problem I have with this paper is that right in the beginning they cite the Swedish estimate that 26% of Stockholm would be infected by 5/1, but we now know that Stockholm only has 11% infected (at most), as per antibody testing of blood donors and the paper saying 26% would be infected was retracted. https://www.forbes.com/sites/davidn...ontroversial-coronavirus-report/#2b1b7c484349
- In the big picture if herd immunity is really around 43% vs. 60-70%, that would likely reduce overall deaths by at least 1/3 to maybe 1/2, depending on the percentage already infected.
- We also now have a preprint of another paper from Gomes et al from a few days ago (tweeted about by Dr. Scott Gottleib, former FDA Commissioner), proposing that herd immunity could also be significantly reduced, but by the mechanism of "variable susceptability" of infection, proposing that there is a range of susceptibility to getting the virus.
- https://www.medrxiv.org/content/10.1101/2020.04.27.20081893v1.full.pdf
- In this paper, they speculate that the herd immunity endpoint could be reduced from the standard 60-70% of the population infected to a wide range of numbers, even as low as 10%. Given that NYC is already at or above 20%, obviously their low end of the range looks flawed, which makes me wonder about the applicability of their methodology.
- Here is an excerpt: Individuals that are frailer, and therefore more susceptible or more exposed, have higher probabilities of being infected, depleting the susceptible subpopulation of those who are at higher risk of infection, and thus intensifying the deceleration in occurrence of new cases. Eventually, susceptible numbers become low enough to prevent epidemic growth or, in other words, herd immunity is attained. Although estimates vary, it is currently believed that herd immunity to SARS-CoV-2 requires 60-70% of the population to be immune. Here we show that variation in susceptibility or exposure to infection can reduce these estimates. Achieving accurate estimates of heterogeneity for SARS-CoV-2 is therefore of paramount importance in controlling the COVID-19 pandemic.
- Clearly, though, if herd immunity were something more possible, like 30-40%, total deaths in hotspot places like NYC/NENJ and parts of Europe might end up not being more than double what they are now, in the worst case and maybe less than that.
- https://www.medrxiv.org/content/10.1101/2020.04.27.20081893v1.full.pdf
It's not just the elderly and it's not just about the health care system - to me, it's much more about preventing 1MM or more additional US deaths over the next 6-18 months, assuming we open things up and allow the US to move towards herd immunity, which is what some seem to want.
There are 83MM people in the US aged 45-64 and the total death rate for these people from COVID in NYC is 1540 per 1MM, which translates to 127K deaths of people in the US between 45 and 64, assuming the NYC death rates are similar for what the US's will be, which should eventually be the case, even if it's not now, as there should be no reason NYC people would be more likely to die from the virus than anyone else, unless there's some demographic or health care system reason, which could be factors, but are likely minor ones. But NYC only has about 20-25% infected so far (20% as of 4/30, but the first two results were closer to 25%, so since more people have been infected since the antibody study, let's take the 25% number infected right now in NYC. So one needs to multiply that 25% infected by 2.4X to get the total number of deaths for 60% being infected or very close to herd immunity. That would up the number to 305K dead between 45-64.
There are 30MM people in the US 65-74 and the NYC death rates for them is 5020 per 1MM, which translates to 150K deaths of people in the US between 65 and 74, assuming the NYC death rates are similar for what the US's will be. But NYC only has about 25% infected so far, so one needs to multiply that number by 2.4X to get the total number of deaths for 60% being infected or very close to herd immunity. That would up the number to 360K dead between 65-74.
There are 19MM people in the US over 75 and the NYC death rates for them is 12,620 per 1MM, which translates to 240K deaths of people in the US for people 75 and over, assuming the NYC death rates are similar for what the US's will be. But NYC only has about 25% infected so far, so one needs to multiply that number by 2.4X to get the total number of deaths for 60% being infected or very close to herd immunity. That would up the number to 576K dead between 45-64.
And finally, there are 109MM people in the US 19-44 and the NYC death rates for them is 168 per 1MM, which translates to "only" 18K deaths of people in the US between 19 and 44, assuming the NYC death rates are similar for what the US's will be. But NYC only has about 25% infected so far, so one needs to multiply that number by 2.4X to get the total number of deaths for 60% being infected or very close to herd immunity. That would up the number to 43K dead between 19-44. In a typical flu season, about 3400 people from 18-49 (didn't have 19-44) die from the flu and that number would obviously be less (3000?) for 18-44.
That's about 1.28MM total US dead, which is a fair amount greater than the 950K total dead the Wharton model had last week, if we stopped all interventions/social distancing and went to herd immunity over the next 6 to maybe 18 months (because the rate of spread will be much slower in low population density areas). The calcs above assume no interventions and no treatment/cure/vaccine and 60% of the US becoming infected at herd immunity and dying at rates we see in NYC now. The calcs also assume the NYC ~25% infected number, from antibody testing is correct. There could obviously be errors in all of those assumptions, but even if the deaths were simply just the 950K deaths in the Wharton model that's still an insane level of deaths over the next 18 months or so.
Also, here's a reality check on the numbers above. NYC right now, has 19,700 deaths in 25% of its population of 8.5MM (2.12MM infected) so the infection fatality number right now is 0.93%. If that overall 0.93% number held for the 60% of 330MM that would eventually become infected, that would be 1.84MM US deaths. Even if we went with NY State numbers of 26K deaths in 15% of the population with antibodies out of 20MM, that's an IFR of 0.86%, which would translate to 1.70MM US deaths. We better hope there are a lot more people with antibodies in NYC/NY or that there is something unusual about NYC/NY death rates or that we have a real treatment (plasma/engineered antibodies?) soon or that transmission rates end up being slower than expected in less densely populated areas with less interventions, giving more time for a cure/vaccine. Also, keep in mind that true infection rates in the rest of the US are likely only around 3-5%, given the much slower outbreaks in much less densely populated areas - this is where a Federal antibody testing program would be nice.
These kinds of potential deaths are why we need to get transmission rates down to much lower levels, such that death rates will stay at low levels, especially until we have a treatment/cure/vaccine. And the only way to do that is aggressive testing, tracing, and isolating to quickly detect and snuff out flare-ups, along with wearing masks in public and at least moderate social distancing to prevent the flare-ups in the first place and minimize them when they occur. This is the direction the NE Region (NY, NJ, CT, RI, MA, PA, DE) are heading as well as CA, WA, and OR, which combined are about 1/3 of the US population (106MM) but not the direction much of the rest of the country is headed.
US Population By Age (2018)
Sometimes I wonder if I'm missing something really important, but nothing obvious comes to mind. Hey @SkilletHead2 - being a numbers/math guy, who hasn't been immersed in this, as far as I can tell - can you check me here? Thanks.
The latest (5/4) projections are out from the U of Washington/IHME and they're very bad, with the US deaths predicted to jump from the 72K in the 4/27 model to 134K through the end of July in the 5/4 model run. NY deaths are modeled to increase from 24K in the 4/27 model to 32K in the 5/4 model (more distancing modeled, hence the smaller increase vs. the US) and NJ deaths are modeled to increase from 7,2K in the 4/27 mode to 16K in the 5/4 model (not clear why NJ wasn't treated like NY).
They've completely overhauled the model and are now factoring in an increase in deaths due to expected significant increases in transmissions related to significant relaxation of stay at home policies and social distancing efforts, as well as slower than expected declines in deaths everywhere, once peaks are reached and passed. Haven't had time to go through it all, as there's a ton of new info, but did include the updated US/NY/NJ graphics. Will update this post with more later...
In addition, the Times obtained an internal CDC report from internal modeling, which is also predicting roughly a doubling of deaths from the current 68K (that would be 136K) by mid-summer, but the Administration is pushing back on that saying the report hasn't been fully vetted yet. However, President Trump on Sunday said deaths could reach 100K, so it certainly seems like forecasts are getting worse, even if not final yet. In that CDC report, it shows deaths per day increasing from the current ~2000/day to over 3000 per day by June.
https://covid19.healthdata.org/united-states-of-america
https://www.nytimes.com/2020/05/04/us/coronavirus-live-updates.html#link-32993cff
https://int.nyt.com/data/documenthe...f7319f4a55fd0ce5dc9/optimized/full.pdf#page=1
As I have been saying for the past week or so and which the Wharton model clearly confirmed on Friday, if restrictive policies are relaxed and social distancing lessened significantly, as looks to be happening, without an infrastructure to test massively and rapidly to detect outbreaks and to trace contacts and isolate positives and contacts, like South Korea and Taiwan have done (which we don't appear to be ready/willing to implement), deaths will get far worse than most have been projecting (including me). If one assumes a 60% infection endpoint (near herd immunity) and a very conservative 0.2% infection fatality rate (NY is at 0.7% now), then about ~400K US deaths would occur in the next 6-12 months if we open it all back up, but if we use an IFR of 0.5% (plausible), the estimate would be 1000K US deaths, which is pretty damn close to Wharton's 950K estimate in their model with limited controls/distancing.
https://rutgers.forums.rivals.com/t...social-distancing.191275/page-94#post-4539724
The only other hope we have to not hit the modeled numbers of deaths in the next 2 months is if we have a bona fide cure (or close to it) in place in the next month or so. We all better hope convalescent plasma is as good as the anecdotal reports are indicating, since that can help now, whereas even the engineered antibodies, which could be available by late summer, will be too late to prevent many of these deaths, and a vaccine is at least several more months beyond late summer.
Excellent new simulator from Penn's Wharton School of Business was just released. Shows the tradeoffs between public health and the economy. One can select three different levels of "reopening" from current baseline to partial reopening to full reopening and two different levels of social distancing from the current baseline aggressive distancing to partial distancing. The differences in modeled additional deaths are huge by the end of June and the economic impacts (especially jobs lost) of the current state are huge too, as expected.
Here are a few highlights from three scenarios, analyzed by US News in the 2nd link and summarized below. I have no idea how accurate the economics part is, but the modeled deaths are significantly greater than the IHME (U of Washington) model, which is only showing 73K dead through the end of June if we continue with the current state, while Scenario 1 below, shows 117K US deaths by the end of June if we continue with our current state. IHME has consistently been underpredicting deaths the past few weeks, so perhaps this new model is more realistic.
- Scenario 1: If we continue with the current state of significant work/school policy restrictions (which is already unrealistic, as many states are partly reopening as of 5/1) and continue with aggressive individual social distancing, the death toll would still rise to 117K by 6/30.
- In Scenario 1, however, U.S. gross domestic product would end June down 11.6% over the year, and roughly 18.6 million more jobs would be lost between May 1 and June 30.
- Scenario 2: Under an arguably more realistic "partial open scenario," in which States immediately lift emergency declarations, stay-at-home orders, and school closures, but maintaining some restrictions (like the prohibition of in-house dining at bars and restaurants), while residents continue practicing aggressive individual social distancing, we'd see an additional 45,000 deaths (vs. the first scenario above) by the end of June, meaning the U.S. total at that point would reach 162,000.
- In Scenario 2, roughly 4.4 million jobs would be saved. The U.S. would still see a loss of 14 million positions between May 1 and June 30 vs. the 18.6MM jobs lost in the first scenario
- Scenario 3: Under a less realistic scenario in which all state economies/schools/businesses, etc. fully reopen without any restrictions on May 1, an additional 233,000 deaths (vs. scenario 1) would be recorded by the end of June, even if individuals continued practicing aggressive individual social distancing, leading to a total of roughly 350,000 deaths (close to the number of Americans who died during World War II).
- In Scenario 3, about 500,000 jobs would be lost between May 1 and June 30, and the size of the U.S. economy would be down roughly 10% over the year.
- For all three scenarios above, if we greatly reduce individual social distancing, the number of deaths goes up substantially more, as per the the last 3 rows in the Wharton table below
- For the most aggressive case, the model predicts 950K US deaths if we stopped all interventions/social distancing. This scenario is much closer to what my thinking is, as per my post above, i.e., at least ~400K US deaths in the next 12 months if we open it all back up - remember, my scenario above used an infection fatality rate of 0.2% (very conservative), whereas if that is 0.5% (plausible), my estimate would've been 1000K US deaths, which is pretty damn close to their 950K estimate.

I think we can all agree that all of these scenarios suck. As I've said countless times, my preference would be to follow South Korea and invest in massive testing/tracing/isolating to greatly reduce deaths (well below even Scenario 1, if we did it well) and allow at least partial reopening. These aren't even options being considered in this country right now though (only by a few governors).
https://budgetmodel.wharton.upenn.edu/issues/2020/5/1/coronavirus-reopening-simulator
https://www.usnews.com/news/economy...-000-deaths-by-july-but-save-millions-of-jobs
I wonder how much of "modernization" of material is just textbook companies needing to sell new titles. If you do not "modernize" subjects.. the same old textbooks will do a long service.When Tyler went back to school in the spring of his 4th grade year, they were learning long division. So, at home, I taught him long division in under an hour, just doing it on paper. He gets into school, they spend 2 weeks learning how to estimate results when dividing? Really?
But if that had happened, Harry wouldn't have gotten the copy of the text belonging to the Half-Blood Prince.I wonder how much of "modernization" of material is just textbook companies needing to sell new titles. If you do not "modernize" subjects.. the same old textbooks will do a long service.
THAT.. was the one thing that broke the illusion of reality for me.But if that had happened, Harry wouldn't have gotten the copy of the text belonging to the Half-Blood Prince.
In case this pandemic isn't depressing enough, a paper today in Nature (a top journal) discusses various coronaviruses in pangolins, one of the most heavily trafficked mammals in Asia/China and one suspected to possibly be the intermediate host between bats and humans for SARS-CoV-2 (the current coronavirus). They've found viruses that are almost identical to CV2 in the critical receptor binding domain of the spike protein, which is the part of the virus which attaches to host cells. These wet markets really need to be shut down.
https://www.nature.com/articles/s41586-020-2313-x_reference.pdf
In particular, the receptor-binding domain within the S protein of the Pangolin-CoV is virtually identical to that of SARS-CoV-2, with one noncritical amino acid diference. Results of comparative genomic analysis suggest that SARS-CoV-2 might have originated from the recombination of a Pangolin-CoV-like virus with a Bat-CoV-RaTG13-like virus. The Pangolin-CoV was detected in 17 of 25 Malayan pangolins analyzed. Infected pangolins showed clinical signs and histological changes, and circulating antibodies against Pangolin-CoV reacted with the S protein of SARS-CoV-2. The isolation of a coronavirus that is highly related to SARS-CoV-2 in pangolins suggests that they have the potential to act as the intermediate host of SARS-CoV-2. The newly identifed coronavirus in the most-trafcked mammal could represent a future threat to public health if wildlife trade is not efectively controlled.
https://www.nature.com/articles/s41586-020-2313-x_reference.pdf
In particular, the receptor-binding domain within the S protein of the Pangolin-CoV is virtually identical to that of SARS-CoV-2, with one noncritical amino acid diference. Results of comparative genomic analysis suggest that SARS-CoV-2 might have originated from the recombination of a Pangolin-CoV-like virus with a Bat-CoV-RaTG13-like virus. The Pangolin-CoV was detected in 17 of 25 Malayan pangolins analyzed. Infected pangolins showed clinical signs and histological changes, and circulating antibodies against Pangolin-CoV reacted with the S protein of SARS-CoV-2. The isolation of a coronavirus that is highly related to SARS-CoV-2 in pangolins suggests that they have the potential to act as the intermediate host of SARS-CoV-2. The newly identifed coronavirus in the most-trafcked mammal could represent a future threat to public health if wildlife trade is not efectively controlled.
This is disappointing...we had a domestic manufacturer capable of making an additional 1.7MM N95 masks per week and they were never used by the Administration until April. And here's the worst part: "In the end, the government did not take Bowen up on his offer. Even today, production lines that could be making more than 7 million masks a month sit dormant."
It was Jan. 22, a day after the first case of covid-19 was detected in the United States, and orders were pouring into Michael Bowen’s company outside Fort Worth, some from as far away as Hong Kong.
Bowen’s medical supply company, Prestige Ameritech, could ramp up production to make an additional 1.7 million N95 masks a week. He viewed the shrinking domestic production of medical masks as a national security issue, though, and he wanted to give the federal government first dibs.
“We still have four like-new N95 manufacturing lines,” Bowen wrote that day in an email to top administrators in the Department of Health and Human Services. “Reactivating these machines would be very difficult and very expensive but could be achieved in a dire situation.”
But communications over several days with senior agency officials — including Robert Kadlec, the assistant secretary for preparedness and emergency response — left Bowen with the clear impression that there was little immediate interest in his offer.
https://www.washingtonpost.com/inve...y.html?utm_source=reddit.com#comments-wrapper
It was Jan. 22, a day after the first case of covid-19 was detected in the United States, and orders were pouring into Michael Bowen’s company outside Fort Worth, some from as far away as Hong Kong.
Bowen’s medical supply company, Prestige Ameritech, could ramp up production to make an additional 1.7 million N95 masks a week. He viewed the shrinking domestic production of medical masks as a national security issue, though, and he wanted to give the federal government first dibs.
“We still have four like-new N95 manufacturing lines,” Bowen wrote that day in an email to top administrators in the Department of Health and Human Services. “Reactivating these machines would be very difficult and very expensive but could be achieved in a dire situation.”
But communications over several days with senior agency officials — including Robert Kadlec, the assistant secretary for preparedness and emergency response — left Bowen with the clear impression that there was little immediate interest in his offer.
https://www.washingtonpost.com/inve...y.html?utm_source=reddit.com#comments-wrapper
This is disappointing...we had a domestic manufacturer capable of making an additional 1.7MM N95 masks per week and they were never used by the Administration until April. And here's the worst part: "In the end, the government did not take Bowen up on his offer. Even today, production lines that could be making more than 7 million masks a month sit dormant."
It was Jan. 22, a day after the first case of covid-19 was detected in the United States, and orders were pouring into Michael Bowen’s company outside Fort Worth, some from as far away as Hong Kong.
Bowen’s medical supply company, Prestige Ameritech, could ramp up production to make an additional 1.7 million N95 masks a week. He viewed the shrinking domestic production of medical masks as a national security issue, though, and he wanted to give the federal government first dibs.
“We still have four like-new N95 manufacturing lines,” Bowen wrote that day in an email to top administrators in the Department of Health and Human Services. “Reactivating these machines would be very difficult and very expensive but could be achieved in a dire situation.”
But communications over several days with senior agency officials — including Robert Kadlec, the assistant secretary for preparedness and emergency response — left Bowen with the clear impression that there was little immediate interest in his offer.
https://www.washingtonpost.com/inve...y.html?utm_source=reddit.com#comments-wrapper
Why should they make 1.7 mil masks/week when Fauci doesn't think they are warranted to prevent transmission? Such illogical thinking I want to put my fist through the wall.
Don't know if this was posted or not already but just saw on the news this morning and found a related article that frontline workers in NY(healthcare, transit, first responders) tested for antibodies at about the same rate or less than the general population. Might think they might have a higher infection rate but looks to be about the same....proper protection and hygiene work.
From the article:
Cuomo said 27,000 healthcare workers across 25 downstate facilities were tested for antibodies.
In New York City, 20% of the general public had antibodies, compared to about 12% of healthcare workers.
In Westchester, near the state’s first coronavirus outbreak, nearly 14% of the general public had antibodies, while just about 7% of healthcare workers had them.
Nearby Long Island tested at roughly the same rate: 11.4% of the general public tested for antibodies while healthcare workers were at 11.1%.
Cuomo said the results suggest that healthcare workers must have protective equipment, like masks, gloves and gowns—and that along with hand sanitizer, proves effective against preventing the virus’ spread.
“We were afraid of what was going to happen” to healthcare workers, Cuomo said, adding that the numbers show healthcare workers are following the protective equipment protocols and therefore getting infected at lower rates.
“Those masks work,” Cuomo said. “If they’re working for front line workers, they’re going to work for people in their day to day lives.”
https://www.forbes.com/sites/lisett...9-compared-to-public-cuomo-says/#48f1d3be6619
From the article:
Cuomo said 27,000 healthcare workers across 25 downstate facilities were tested for antibodies.
In New York City, 20% of the general public had antibodies, compared to about 12% of healthcare workers.
In Westchester, near the state’s first coronavirus outbreak, nearly 14% of the general public had antibodies, while just about 7% of healthcare workers had them.
Nearby Long Island tested at roughly the same rate: 11.4% of the general public tested for antibodies while healthcare workers were at 11.1%.
Cuomo said the results suggest that healthcare workers must have protective equipment, like masks, gloves and gowns—and that along with hand sanitizer, proves effective against preventing the virus’ spread.
“We were afraid of what was going to happen” to healthcare workers, Cuomo said, adding that the numbers show healthcare workers are following the protective equipment protocols and therefore getting infected at lower rates.
“Those masks work,” Cuomo said. “If they’re working for front line workers, they’re going to work for people in their day to day lives.”
https://www.forbes.com/sites/lisett...9-compared-to-public-cuomo-says/#48f1d3be6619
In the future instead of slapping a baby when they are born the nurses will just slap on a face mask.
- Status
- Not open for further replies.
Similar threads
- Replies
- 93
- Views
- 3K
- Replies
- 8
- Views
- 1K
- Replies
- 7
- Views
- 724
- Replies
- 0
- Views
- 1K
ADVERTISEMENT
ADVERTISEMENT