
Have you been allowed to do even emergency cases? I was actually wondering about this the other day because I've had root canals that were so painful that if I had to wait a couple months I might have jumped off the Driscoll Bridge.I have also been telling my girls June 1 but at least give us some guidance so we have an idea fo what to do with our patients because even when we open and many others things will not be normal until we get a vaccine
Colleges
- American Athletic
- Atlantic Coast
- Big 12
- Big East
- Big Ten
- Colonial
- Conference USA
- Independents (FBS)
- Junior College
- Mountain West
- Northeast
- Pac-12
- Patriot League
- Pioneer League
- Southeastern
- Sun Belt
- Army
- Charlotte
- East Carolina
- Florida Atlantic
- Memphis
- Navy
- North Texas
- Rice
- South Florida
- Temple
- Tulane
- Tulsa
- UAB
- UTSA
- Boston College
- California
- Clemson
- Duke
- Florida State
- Georgia Tech
- Louisville
- Miami (FL)
- North Carolina
- North Carolina State
- Pittsburgh
- Southern Methodist
- Stanford
- Syracuse
- Virginia
- Virginia Tech
- Wake Forest
- Arizona
- Arizona State
- Baylor
- Brigham Young
- Cincinnati
- Colorado
- Houston
- Iowa State
- Kansas
- Kansas State
- Oklahoma State
- TCU
- Texas Tech
- UCF
- Utah
- West Virginia
- Illinois
- Indiana
- Iowa
- Maryland
- Michigan
- Michigan State
- Minnesota
- Nebraska
- Northwestern
- Ohio State
- Oregon
- Penn State
- Purdue
- Rutgers
- UCLA
- USC
- Washington
- Wisconsin
High Schools
- Illinois HS Sports
- Indiana HS Sports
- Iowa HS Sports
- Kansas HS Sports
- Michigan HS Sports
- Minnesota HS Sports
- Missouri HS Sports
- Nebraska HS Sports
- Oklahoma HS Sports
- Texas HS Hoops
- Texas HS Sports
- Wisconsin HS Sports
- Cincinnati HS Sports
- Delaware
- Maryland HS Sports
- New Jersey HS Hoops
- New Jersey HS Sports
- NYC HS Hoops
- Ohio HS Sports
- Pennsylvania HS Sports
- Virginia HS Sports
- West Virginia HS Sports
ADVERTISEMENT
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
COVID-19 Pandemic: Transmissions, Deaths, Treatments, Vaccines, Interventions and More...
- Thread starter RU848789
- Start date
- Status
- Not open for further replies.
Tell your friend he is good to go.Does this mean that if I commit a crime, get caught, and go to jail, that I will be more likely to be asymptomatic then the general public?
Asking for a friend.
so since I can;t find any n95 masks what is the next best thing to get? should I get one of those reusable facemasks with filters i see on facebook? are they better than disposable surgical masks?
https://www.aphp.fr/contenu/tociliz...outcomes-patients-moderate-or-severe-covid-19
Encouraging beginnings. This is how the doctors of the Public Assistance-Hospitals of Paris judge the first results of the study currently being conducted with tocilizumab. This drug, usually used in rheumatology, "significantly improves the prognosis of patients with moderate or severe Covid pneumonia , " said the APHP in a statement released Monday, April 27.
Sounds promising, although it's open-label and not large (~65 patients each in the tocilizumab arm and and the standard of care arm) and they don't provide any data.
On the other hand Regeneron/Sanofi's RA drug, sarilumab, like tocilizumab, another monoclonal antibody blocking the receptor for the interleukin-6 cytokine, failed to show efficacy in "severe" COVID patients in a separate, larger, blinded, placebo-controlled trial with ~229 patients in each arm. They're continuing with the "critical" patient arms.
https://www.nytimes.com/2020/04/27/health/coronavirus-drug-sarilumab.html
But, with doctors around the world dosing ill patients with the arthritis drugs, Regeneron and Sanofi decided it was urgent to get reliable data.
Their clinical trial randomly assigned 457 hospitalized Covid-19 patients to receive either 400 milligrams or 200 milligrams of sarilumab, or a placebo. The patients fell into two groups — “severe,” meaning they required oxygen but did not need a ventilator or so-called high flow oxygen, and “critical,” those who needed a ventilator, high flow oxygen or were in intensive care.
Although the drug reduced c-reactive protein, which rises in severe inflammation, it did not help the severely ill patients, the companies reported on Monday. Many of those patients recovered on their own. Eighty percent were discharged from the hospital, whether or not they were given the drug. Ten percent remained hospitalized, and ten percent died.
The results for the critically ill patients are not conclusive but there is a hint that such patients may be helped, so the study will continue with only critically ill patients. More than 600 have been enrolled. Results are expected in early June.
KN95 which is China's equivalent if you can get them from a reputable place.so since I can;t find any n95 masks what is the next best thing to get? should I get one of those reusable facemasks with filters i see on facebook? are they better than disposable surgical masks?

Haven't watched much of his pressers, and given the recent death toll stats, hard to argue with his measures thus far, but I think you are right that it is important for morale that he set's timelines.Agree. I appreciated his early reaction and response and supported these measures, until today. Other states and NYC have dates and thresholds, and all we have is this guy asking God for help, and posting Instagram photos of dead residents. It's getting weird with him quite frankly.
I tend to think there is a plan, but he does need to communicate it.
KN95 which is China's equivalent if you can get them from a reputable place.
I just got a box of them from my next door neighbor.
Same here:ThumbsUp:ThumbsUp:ThumbsUp for my son who is in an essential job that can now only get surgical masks.I just got a box of them from my next door neighbor.
Last edited:
I just got a box of them from my next door neighbor.
I got some of these also in March. They’re not too bad. Although I have a big melon so they do a number on tugging at my ears.
Is this not the guy, that says if you commit a crime ( rape, murder, robbery, and illegal entry to the country) come to N.J.I agree, Murphy is clueless and has NJ in the worst shape than any state in the country.
we will give you sanctuary. But had nothing for the veterans, and other people of my generation, rotting in nasty, abusive,
so called nursing homes. We have to stop voting for people just because of their party affiliations.
I would recommend a large paper clip (very large) to connect both loops behind your head.I got some of these also in March. They’re not too bad. Although I have a big melon so they do a number on tugging at my ears.
Perfectwhat about the n95 masks for sanding and fiberglass work?
what about the n95 masks for sanding and fiberglass work?
N95 = N95.
I see you and raise you one N95N95 = N95.
N95=N95=N95
Also, FFP2 and P2 masks removes 94% of 0.3 micron particles.what about the n95 masks for sanding and fiberglass work?
I would recommend a large paper clip (very large) to connect both loops behind your head.
Thanks! I’ll give this a try tomorrow at work.
You endorsed shop towels too didn’t you?Also, FFP2 and P2 masks removes 94% of 0.3 micron particles.
Yes we are allowed to do "true emergencies" which of course include root canals!! but I am literally seeing 4-6 patients a week in my office versus probably around 100 and had to layoff the entire staff!!Have you been allowed to do even emergency cases? I was actually wondering about this the other day because I've had root canals that were so painful that if I had to wait a couple months I might have jumped off the Driscoll Bridge.
Question for the guys who know their stuff just read an article about a healthy 46 year old physician who was very sick from Covid and he was given Actemra which is a drug used to treat Rheumatoid Arthritis says he was better in a couple of days after that
Question for the guys who know their stuff just read an article about a healthy 46 year old physician who was very sick from Covid and he was given Actemra which is a drug used to treat Rheumatoid Arthritis says he was better in a couple of days after that
An article was posted in the last page. It’s also called Tocilizumab. Apparently a trial went well and detailed results will be outlined in a journal the next few days. A lot of hype around that and Leronlimab.
Didn't see this posted here: Tyson Foods said yesterday in a NY Times letter to the editor that the supply chain for meats is breaking down, due to plant closures from coronavirus infections. Not good, although I'm guessing there's a little posturing in there to get some Federal help...
https://www.cnbc.com/2020/04/27/tys...ing-as-coronavirus-forces-plant-closures.html
https://www.cnbc.com/2020/04/27/tys...ing-as-coronavirus-forces-plant-closures.html
Didn't see this posted here: Tyson Foods said yesterday in a NY Times letter to the editor that the supply chain for meats is breaking down, due to plant closures from coronavirus infections. Not good, although I'm guessing there's a little posturing in there to get some Federal help...
https://www.cnbc.com/2020/04/27/tys...ing-as-coronavirus-forces-plant-closures.html
Less meat isn’t necessarily a bad thing imo.
A two layer mask from them is decent. If you need or want an N95 equivalent then only a few things will meet your needs like a KN95 or a FFP2/P2.You endorsed shop towels too didn’t you?
Didn't see this posted here: Tyson Foods said yesterday in a NY Times letter to the editor that the supply chain for meats is breaking down, due to plant closures from coronavirus infections. Not good, although I'm guessing there's a little posturing in there to get some Federal help...
https://www.cnbc.com/2020/04/27/tys...ing-as-coronavirus-forces-plant-closures.html
If you'd ever been to a Tyson plant, you'd know that coronavirus wouldn't be the worst thing to happen to you.
Less meat isn’t necessarily a bad thing imo.
You seen a produce aisle lately? Not much to take the place of that meat.
Well I understand that a N95 is the best but looking for other alternatives besides that. I have a couple unused N95s from some time ago from housework but looking at other alternatives beyond that as I think I'm gonna need the use of a mask for a year or 2 and not sure how much mileage I'll get from the 2 N95s. I'll use them over and over and let them sit in the sun and let time do its thing but eventually they may wear out. Also have one of those painter respirator type masks but not sure how comfortable I'll feel wearing that out and about.A two layer mask from them is decent. If you need or want an N95 equivalent then only a few things will meet your needs like a KN95 or a FFP2/P2.
So getting a N95 is very hard now as they're going to hospitals and such as it should be and same for K95s. If you did happen to find some I'd still wonder about the reputable nature of the source and if you're getting something real or just some counterfeit stuff and how would you know. Any reputable retailer like a Target/Walmart/HD/Amazon etc...won't be selling them to the general public for awhile I think. So I've been thinking of the cloths masks I've bought and putting folded up shop towels in the filter slits. Not ideal but I think an okay solution outside of a N95 and a solution that can take me through the next year or 2 as well and enough for the family too.
Along with the testing, I think the masks will once again become an issue going forward. If we want people to get back to work, then I think we need sufficient masks for those situations where social distancing isn’t possible.
How do we have people going on trains, busses, elevators, etc. without masks.
How do we have people going on trains, busses, elevators, etc. without masks.
I have also been telling my girls June 1 but at least give us some guidance so we have an idea fo what to do with our patients because even when we open and many others things will not be normal until we get a vaccine
Excuse me, but if this were World War II you guys would be complaining if FDR didn't give an ending date for the war. We're up against an elusive enemy, and we have to see what the trends are before we know that it's safe to start re-opening. There is no way to set dates at this point.
Some promising stuff out of the Jenner Institute at Oxford.
“In the worldwide race for a vaccine to stop the coronavirus, the laboratory sprinting fastest is at Oxford University.
Most other teams have had to start with small clinical trials of a few hundred participants to demonstrate safety. But scientists at the university’s Jenner Institute had a head start on a vaccine, having proved in previous trials that similar inoculations — including one last year against an earlier coronavirus — were harmless to humans.
That has enabled them to leap ahead and schedule tests of their new coronavirus vaccine involving more than 6,000 people by the end of next month, hoping to show not only that it is safe, but also that it works.
The Oxford scientists now say that with an emergency approval from regulators, the first few million doses of their vaccine could be available by September — at least several months ahead of any of the other announced efforts — if it proves to be effective.
Now, they have received promising news suggesting that it might.
Scientists at the National Institutes of Health’s Rocky Mountain Laboratory in Montana last month inoculated six rhesus macaque monkeys with single doses of the Oxford vaccine. The animals were then exposed to heavy quantities of the virus that is causing the pandemic — exposure that had consistently sickened other monkeys in the lab. But more than 28 days later all six were healthy, said Vincent Munster, the researcher who conducted the test.
“The rhesus macaque is pretty much the closest thing we have to humans,” Dr. Munster said, noting that scientists were still analyzing the result. He said he expected to share it with other scientists next week and then submit it to a peer-reviewed journal.”
#s: Do you think the US pharmaceuticals only jump in with this drug if they can only get worldwide exclusivity?
https://www.nytimes.com/2020/04/27/...action=click&module=Spotlight&pgtype=Homepage
“In the worldwide race for a vaccine to stop the coronavirus, the laboratory sprinting fastest is at Oxford University.
Most other teams have had to start with small clinical trials of a few hundred participants to demonstrate safety. But scientists at the university’s Jenner Institute had a head start on a vaccine, having proved in previous trials that similar inoculations — including one last year against an earlier coronavirus — were harmless to humans.
That has enabled them to leap ahead and schedule tests of their new coronavirus vaccine involving more than 6,000 people by the end of next month, hoping to show not only that it is safe, but also that it works.
The Oxford scientists now say that with an emergency approval from regulators, the first few million doses of their vaccine could be available by September — at least several months ahead of any of the other announced efforts — if it proves to be effective.
Now, they have received promising news suggesting that it might.
Scientists at the National Institutes of Health’s Rocky Mountain Laboratory in Montana last month inoculated six rhesus macaque monkeys with single doses of the Oxford vaccine. The animals were then exposed to heavy quantities of the virus that is causing the pandemic — exposure that had consistently sickened other monkeys in the lab. But more than 28 days later all six were healthy, said Vincent Munster, the researcher who conducted the test.
“The rhesus macaque is pretty much the closest thing we have to humans,” Dr. Munster said, noting that scientists were still analyzing the result. He said he expected to share it with other scientists next week and then submit it to a peer-reviewed journal.”
#s: Do you think the US pharmaceuticals only jump in with this drug if they can only get worldwide exclusivity?
https://www.nytimes.com/2020/04/27/...action=click&module=Spotlight&pgtype=Homepage
Some promising stuff out of the Jenner Institute at Oxford.
“In the worldwide race for a vaccine to stop the coronavirus, the laboratory sprinting fastest is at Oxford University.
Most other teams have had to start with small clinical trials of a few hundred participants to demonstrate safety. But scientists at the university’s Jenner Institute had a head start on a vaccine, having proved in previous trials that similar inoculations — including one last year against an earlier coronavirus — were harmless to humans.
That has enabled them to leap ahead and schedule tests of their new coronavirus vaccine involving more than 6,000 people by the end of next month, hoping to show not only that it is safe, but also that it works.
The Oxford scientists now say that with an emergency approval from regulators, the first few million doses of their vaccine could be available by September — at least several months ahead of any of the other announced efforts — if it proves to be effective.
Now, they have received promising news suggesting that it might.
Scientists at the National Institutes of Health’s Rocky Mountain Laboratory in Montana last month inoculated six rhesus macaque monkeys with single doses of the Oxford vaccine. The animals were then exposed to heavy quantities of the virus that is causing the pandemic — exposure that had consistently sickened other monkeys in the lab. But more than 28 days later all six were healthy, said Vincent Munster, the researcher who conducted the test.
“The rhesus macaque is pretty much the closest thing we have to humans,” Dr. Munster said, noting that scientists were still analyzing the result. He said he expected to share it with other scientists next week and then submit it to a peer-reviewed journal.”
#s: Do you think the US pharmaceuticals only jump in with this drug if they can only get worldwide exclusivity?
https://www.nytimes.com/2020/04/27/...action=click&module=Spotlight&pgtype=Homepage
Wow, pay a few hundred humans to infect themselves with the virus and lets get it over with already.
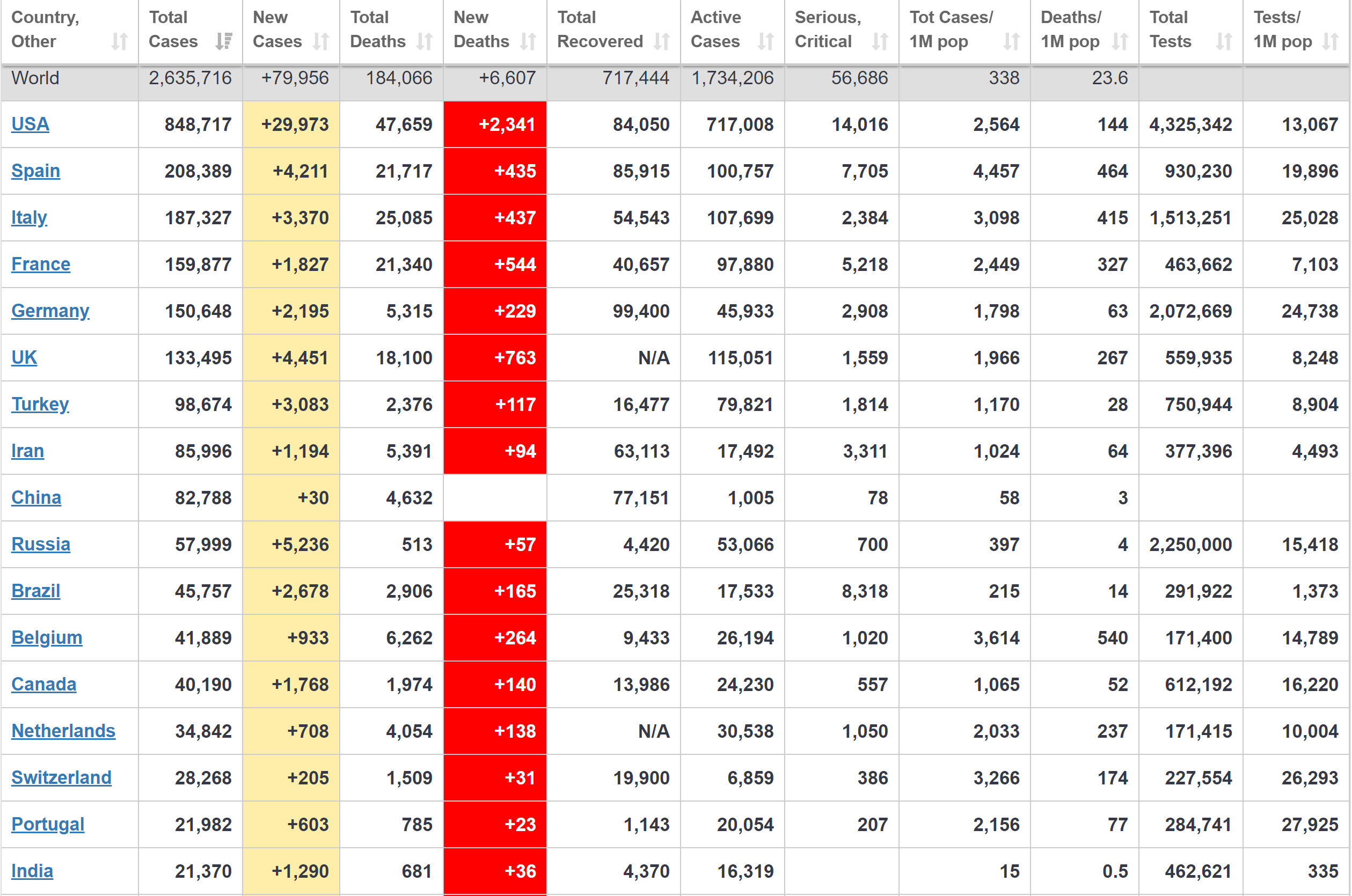
Summary/commentary for some key World/US data through 4/22.
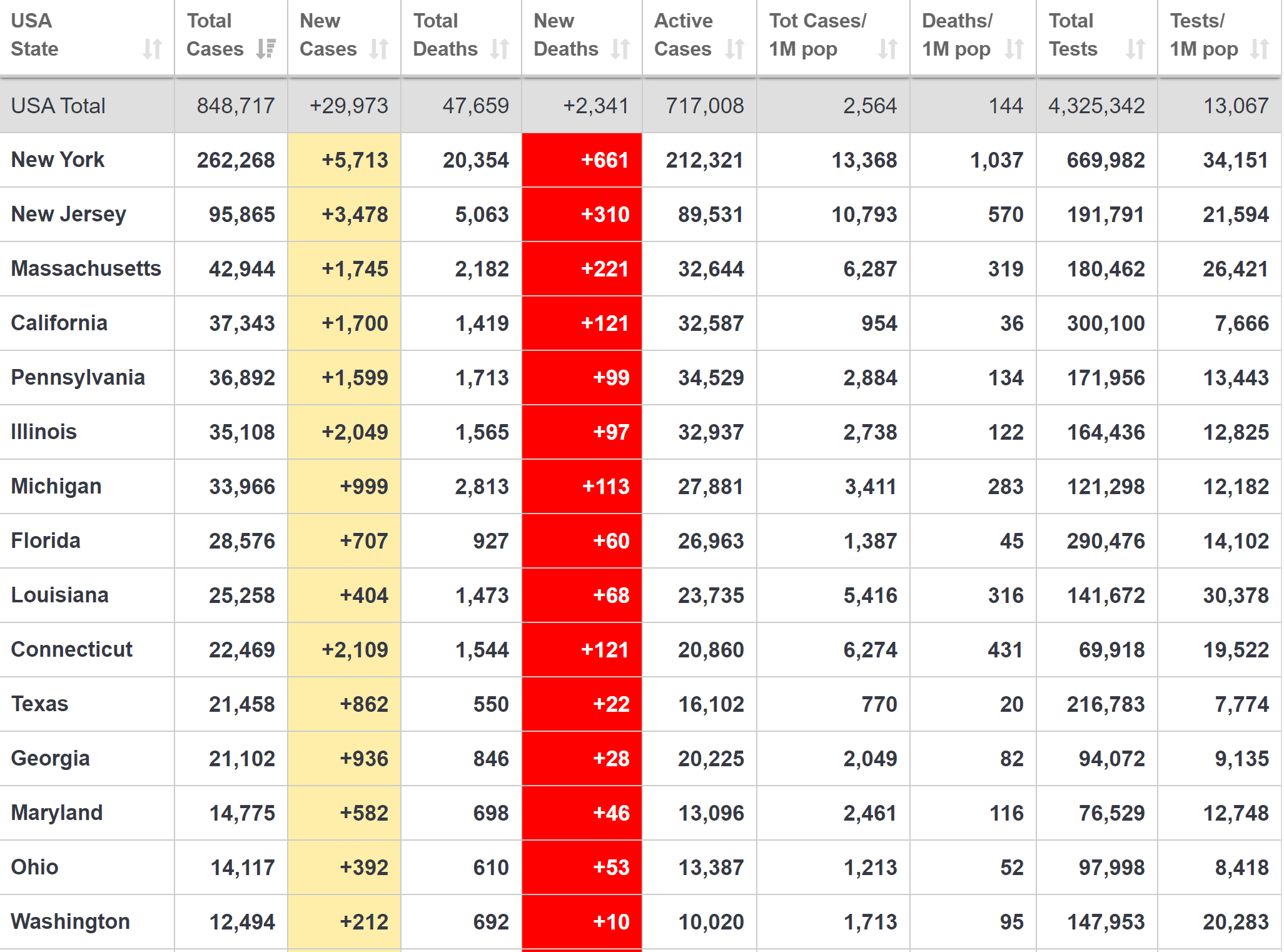
Some comments on NY/NJ/US and from Cuomo’s 4/23 presser
- The most important number in comparing outbreak severity, IMO, is deaths per 1MM people. Italy, Spain and Belgium are the highest in the world, in the neighborhood of 400-500 deaths/1MM, although Belgium is the only one of the major countries reporting “presumed COVID” deaths, which are ~54% of their total. The US is in the middle of the pack with ~144 deaths/1MM, although the US is earlier in its outbreak and will likely catch up somewhat.
- While the US, overall, looks better by comparison, if NY were a country it would have the worst outbreak in the world at 1037 deaths/1MM, while NJ is a little worse than the worst European countries at ~570 deaths/1MM.
- Excluding NY/NJ, the rest of the US is “only” at 74 deaths per 1MM, which is similar to Germany, the “best” of the populous European countries with 63 deaths/1MM. But that needs to be put in context of what is considered “good” control of the epidemic: South Korea, China, Taiwan, Japan, Singapore and more all have <10 deaths/1MM and were all hit with their first waves before the US and Europe. Most believe the differences are primarily due to early/aggressive testing, aggressive contact tracing and quarantining, moderate to aggressive social distancing, and establishing a mask culture.
- The news today from the Northeastern study that NYC likely had 10K cases on 3/1 (with none known and <200 tested through 3/6) means the outbreak was far worse than anyone knew and it’s no surprise that the NYC metro area has gone on to become the worst outbreak in the world, given high density/high commuting density and a very late start on testing and interventions/social distancing (3/16 schools/restaurants/bars closed and 3/22 stay at home orders). In hindsight, the NYC area would have likely needed to lockdown on 3/1 or earlier to have avoided 80-90% of the deaths, once again highlighting why we should have had aggressive early testing to know we had such a bad outbreak.
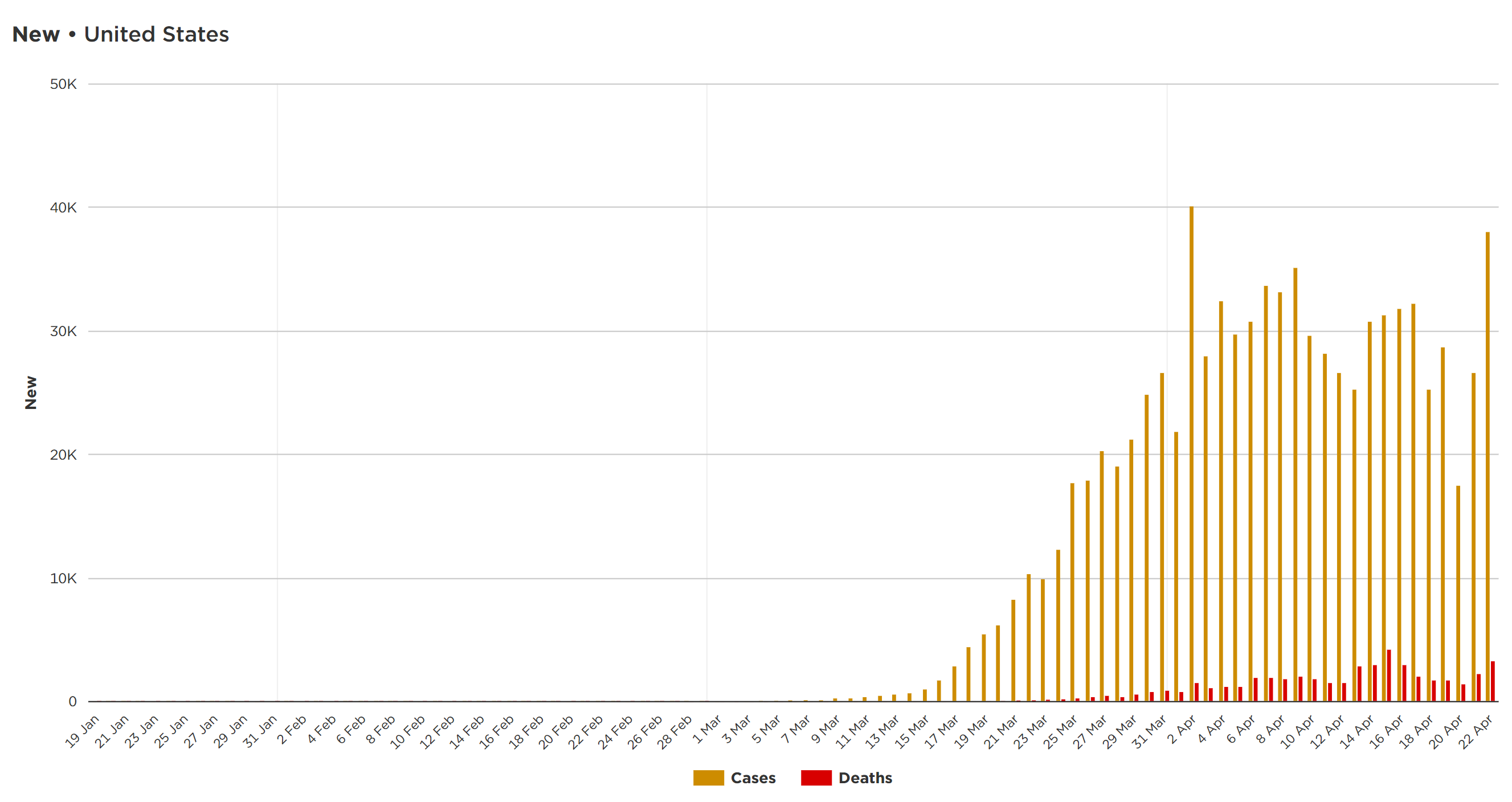
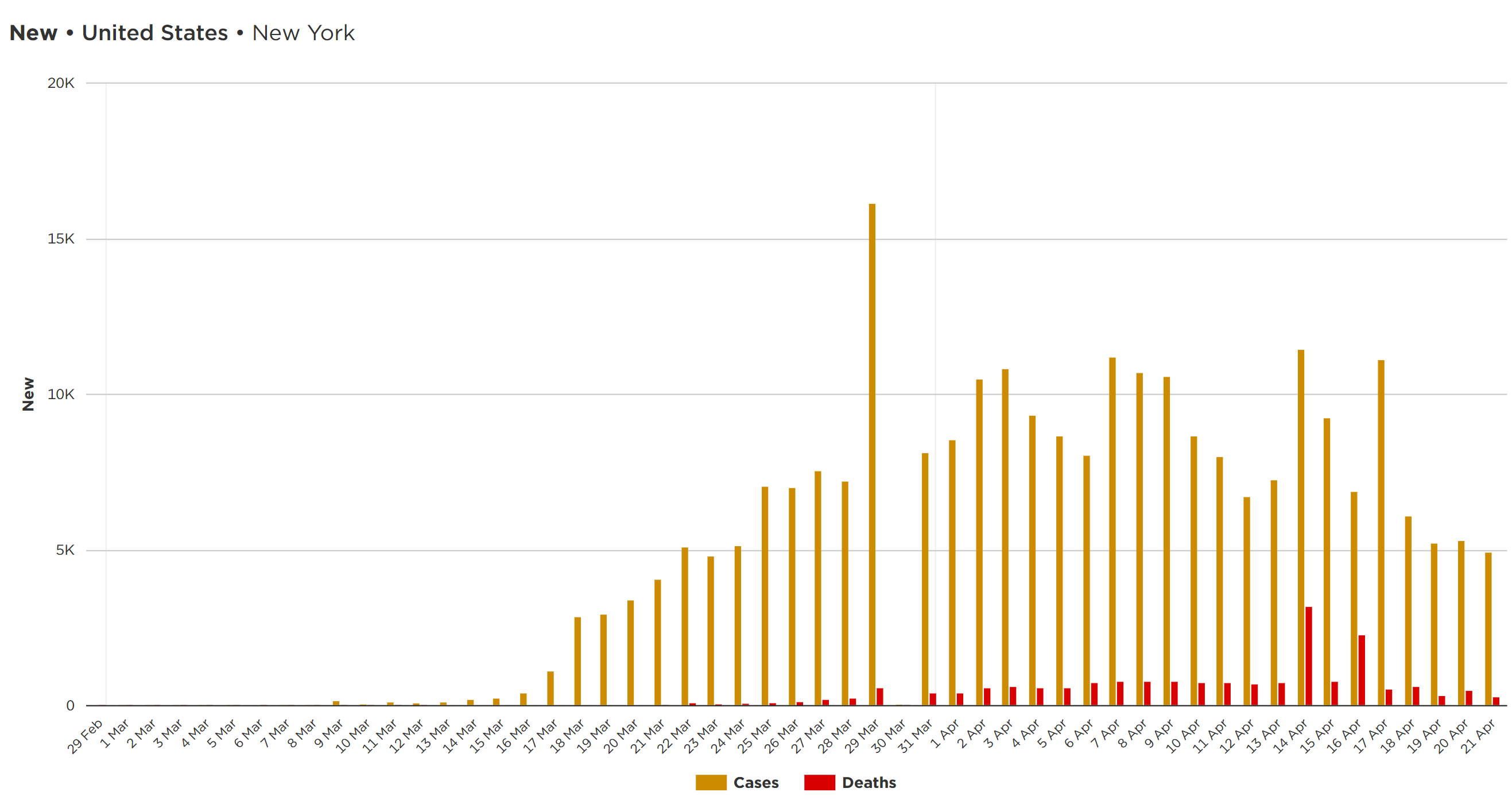
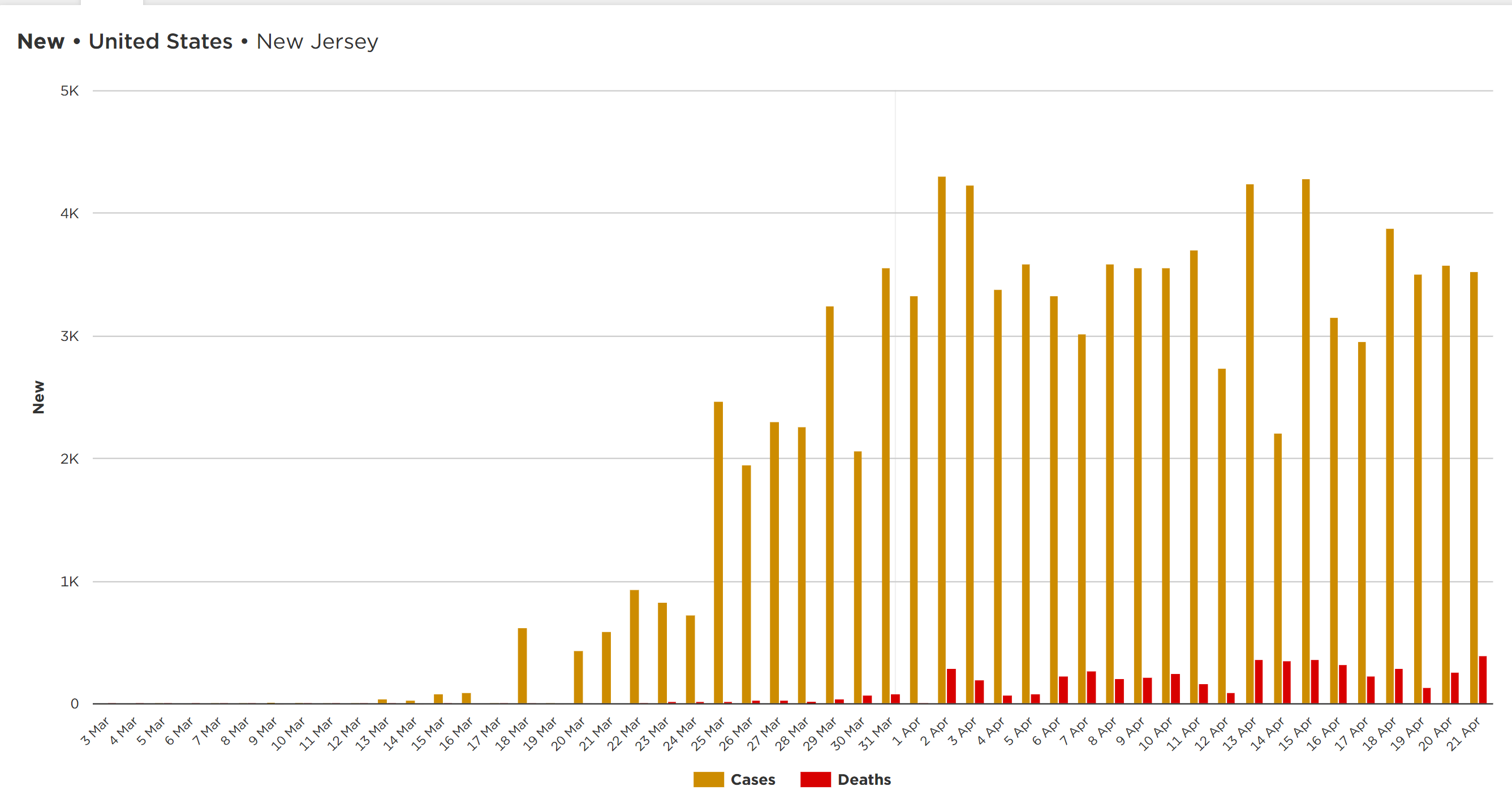
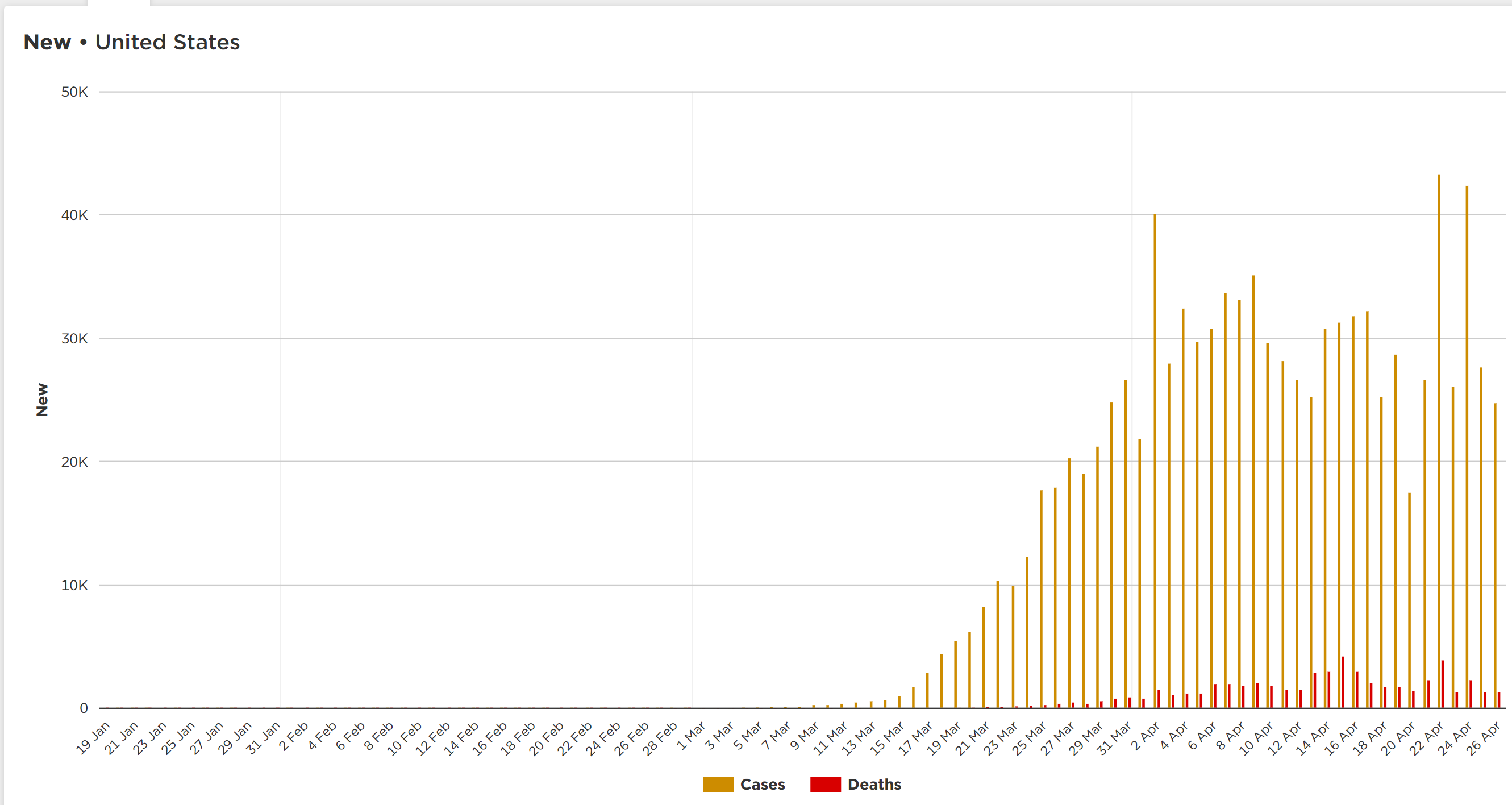
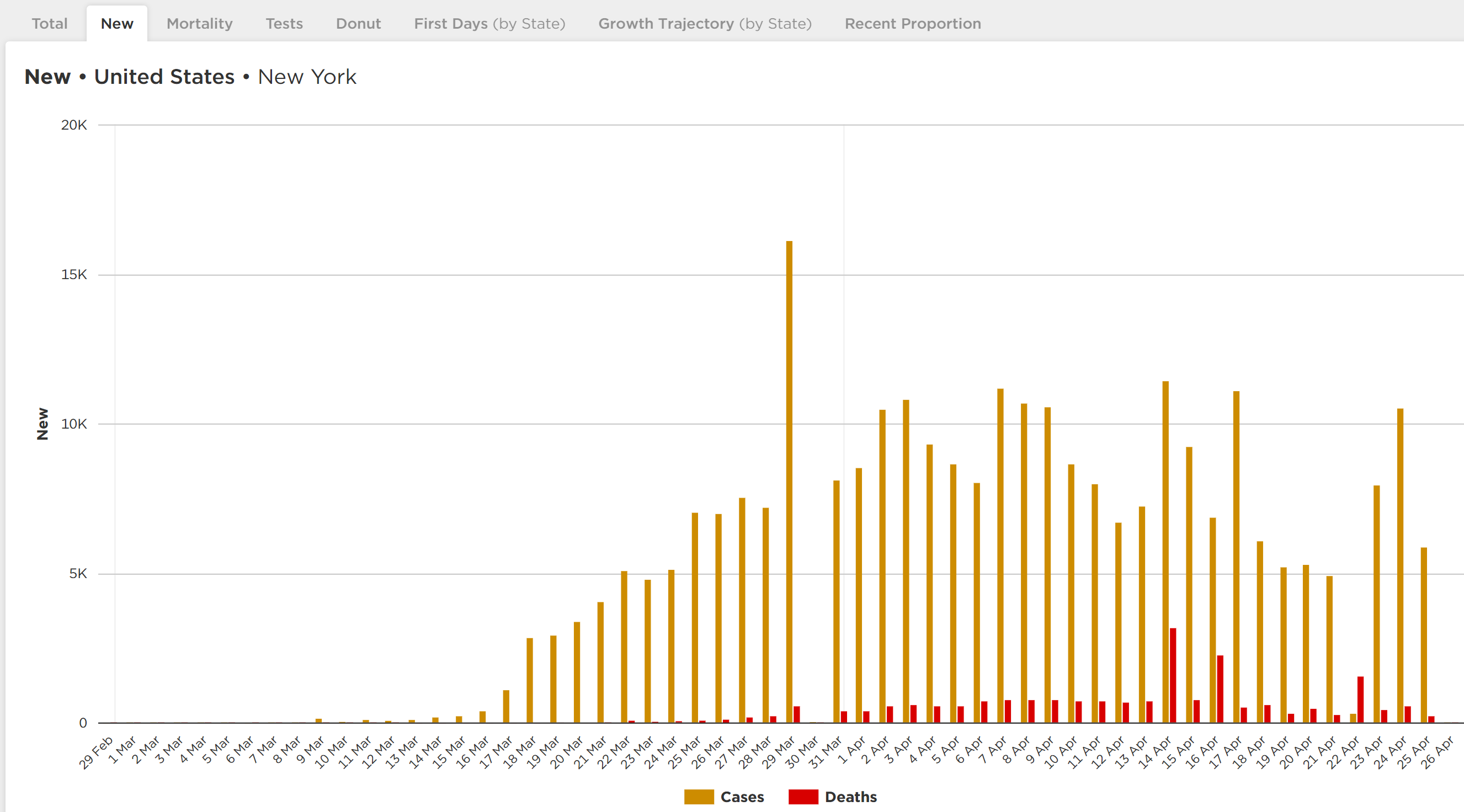
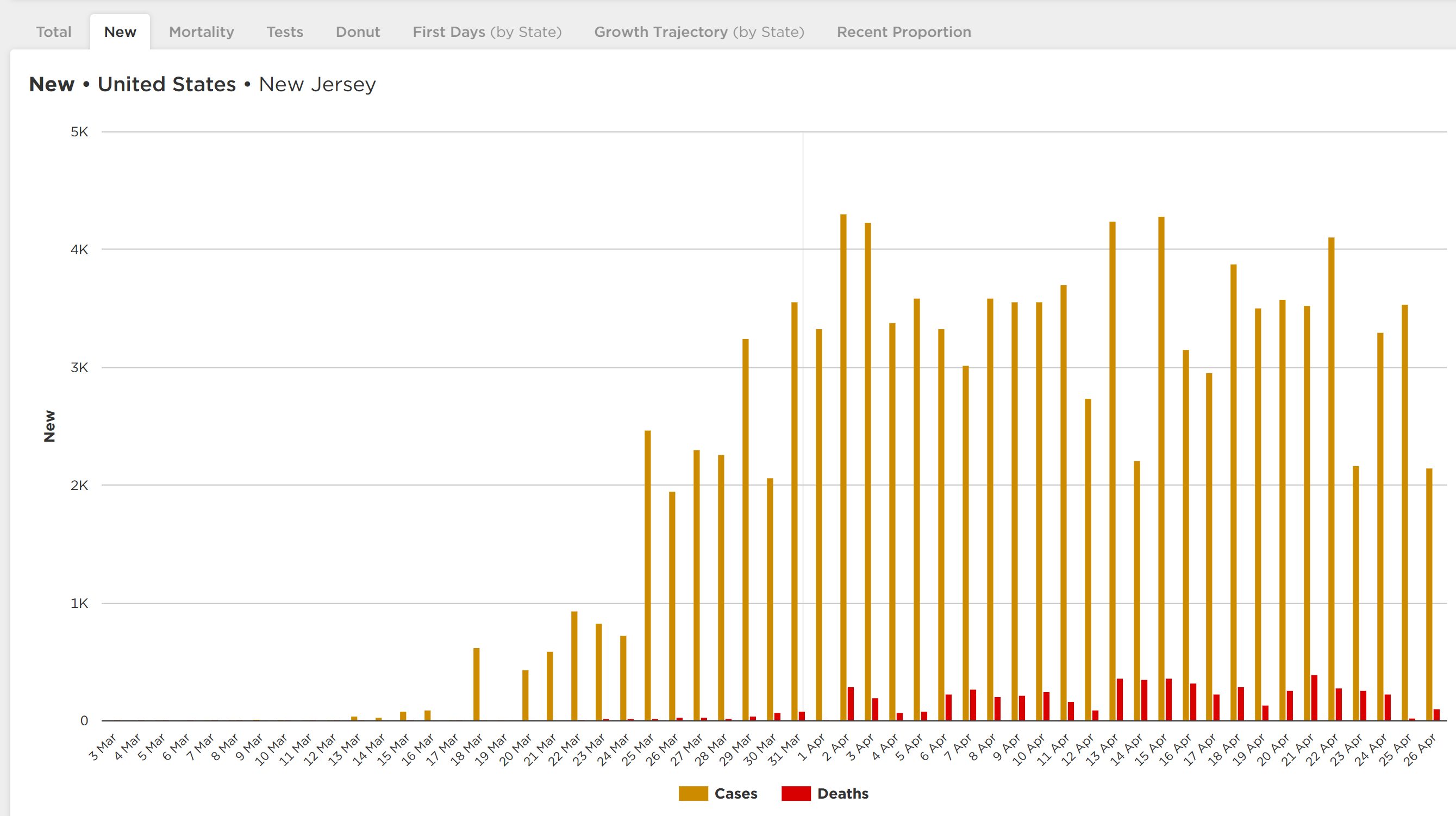
- US deaths have roughly plateaued in the 1500-2500/day range for about the past 12 days (with some fluctuations, including a huge fluctuation when NY added 3800 deaths on 4/14 that were presumed due to COVID, but never had a viral test done (most were in hospitals and it was obvious they had COVID0) and on 4/22 (3300 deaths, but not sure why the jump). Hopefully we’ll see this start to decline in a week or so, as deaths lag cases. NY deaths per day plateaued around 700-800/day for over a week, but declined and have now been 400-500/day over the last 5 days. NJ deaths have fluctuated a fair amount lately, but the moving average shows we’re in a plateau and Gov Murphy said today, that they feel the outbreak is slowing a bit with regard to cases.
- 47.6K, 20.3K and 5.0K total deaths, respectively, through 4/22 in the US, NY, and NJ. The latest U of Washington projection of 66K US deaths might be low at this rate. One oddity though: Worldometer has NY deaths at 20.3K, while Cuomo has NY deaths at 15.5K – NY is still not including the “presumed COVID” (i.e., not tested) deaths.
- The Earth hit 2.63MM cases on 4/18 with 739K cases in the US, 241K in NY and 81K in NJ.
- Both NY and NJ have reached the “peak plateau” in new cases, with some decline in cases definitely occurring in NY, but it’s hard to say that for NJ with so much fluctuation. The big question for NY and eventually NJ is how quickly does the new case rate decline and to what level? Not known now. The US new case rate has been at a plateau for awhile, but has also had some major fluctuations, including yesterday with a huge backlog of tests being reported. It’s why 5-day moving averages are better for trend analyses, but I don’t have those charts.
- NY now has done about 34K tests per 1MM in population, which is more than almost any other country; NJ is at 21K tests per 1MM and the US is at 13K tests per 1MM, both of which are middle-of-the-pack (vs. countries with major outbreaks). As discussed elsewhere, though, it’s not total tests that is critical – it’s testing very aggressively early in an outbreak so that it can be controlled – when that is done, the ratio of positives to tests is low and that never happened in the US or Europe as we feel way behind the oubreak. Fortunately, NY/NYC positives are now down around 25% of total tests from a long plateau in the 40-50% range. NJ test are still up around 50% positive, meaning NJ isn’t testing enough.
- Total number of hospitalized in NY continues to decline steadily.
- As promised, NY is now sending ventilators to other needy states, like Massachusetts, Michigan and Maryland
- Currently, the latest hotspot is Arkansas where new cases jumped nearly 20% yesterday; CT jumped almost 10%.
- He talked at length on the path back to the “new normal”: “Test – Trace – Isolate” is the slogan, with the major focus on the need for fast, massive testing for the virus, to know who is sick or getting sick, so they can be quarantined and their contacts traced, as well as massive antibody testing to know who already has had the virus and now likely has immunity, at least for months to maybe years.
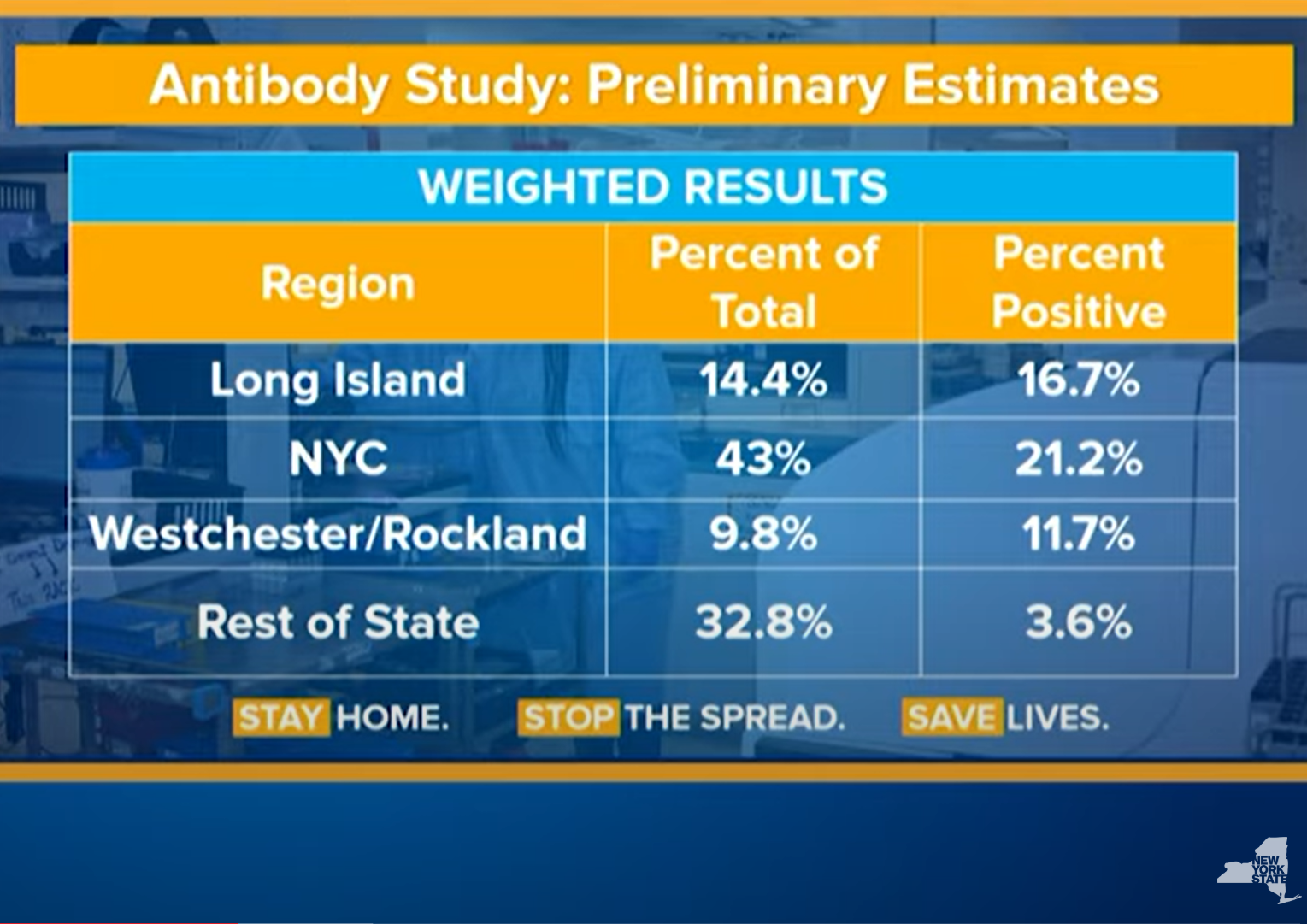
- He also revealed prelimiinary results from their testing of thousands of people from a random, representative sample of the population (3000 so far), to estimate the percentage of people in NY who have had the virus: 1.3% of NY has tested positive by the virus test and preliminary antibody tests show that ~14% of NYers have antibodies, while ~21% of NYC residents have antibodies. Note that these were people who were out and about in stores, so it may be an overestimate. That number greatly impacts how many can go back to work without risks of getting or giving the virus and how much more transmission will occur (with less targets).
- The antibody results also might mean the R0 is very high (5.7 as recently postulated) and that up to 80% of the US/world could become infected if we do nothing, killing hundreds of thousands in the US alone, even if this means the current 7.6% case fatality rate in NY (20K deaths/264K positives) can now finally be translated to an infection fatality rate of 0.7% (20K/2.66MM w/antibodies); if that IFR held and 80% of the US became infected if we did nothing (as we’ve seen in the Ohio prison), that would translate to 330MM x 0.8 x 0.007 = 1.8MM deaths. That’s why we need testing/tracing/isolating and social distancing until we have a proven treatment or vaccine to prevent a calamithy. It’s likely the IFR will continue to decline and the infected % won’t really reach 80%, but even with an IFR of 0.1%, like the flu) and 60% infected, that’s still 200K dead if we do nothing – these were essentially the original arguments for interventions before the outbreak, which way too many downplayed.
- Cuomo rightly slammed Senate Majority Leader McConnell’s frankly heinous statements about not funding states hardest hit by this virus, including funds for health care workers, fire, police, schools, etc., because they’re “blue states.” No words.
Summary/commentary for some key World/US data through 4/26:
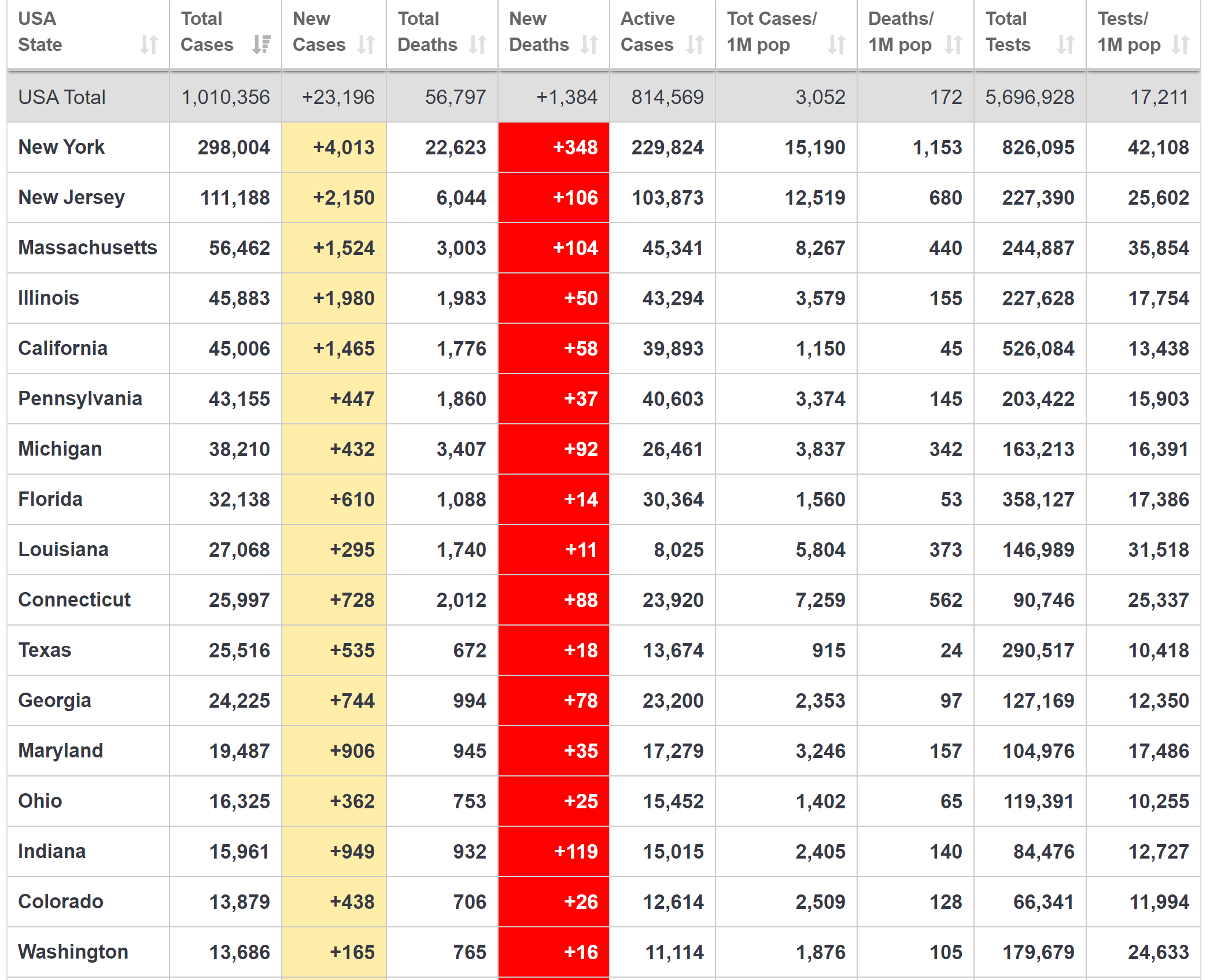
- The most important number in comparing outbreak severity, IMO, is deaths per 1MM people. Italy and Spain are the highest in the world of the major countries (>40MM) in the neighborhood of 450-500 deaths/1MM, The US is in the middle of the pack with ~168 deaths/1MM, although the US is earlier in its outbreak and will likely catch up somewhat.
- While the US, overall, looks better by comparison, if NY were a country it would have the worst outbreak in the world at 1085 deaths/1MM, while NJ is a little worse than the worst European countries at 632 deaths/1MM.
- Excluding NY/NJ, the rest of the US is “only” at 84 deaths per 1MM, which is similar to Germany, the “best” of the populous European countries with 71 deaths/1MM. But that needs to be put in context of what is considered “good” control of the epidemic: South Korea, China, Taiwan, Japan, Singapore and more all have <10 deaths/1MM and were all hit with their first waves before the US and Europe. Most believe the differences are primarily due to early/aggressive testing, aggressive contact tracing and quarantining, moderate to aggressive social distancing, and establishing a mask culture.
- US deaths plateaued in the 1500-2500/day range from about 4/7 to 4/25 (with some fluctuations), but it’s possible we’re finally seeing a decrease as deaths dropped below 1500 the last two days. NY deaths per day continue to fall and are now down from a plateau of 700-800/day to 300-400/day (including nursing homes). NJ deaths have fluctuated a lot, but the moving average shows we’re in a plateau and hopefully starting to drop.
- 56.7K, 22.6K and 6.0K total deaths, respectively, through 4/27 in the US, NY, and NJ. The latest U of Washington projection of 67K US deaths will very likely be low at this rate. Worldometer and Cuomo still have a ~5K difference in NY deaths, as NY is still not including the “presumed COVID” (i.e., not tested) deaths.
- The Earth hit 2.99MM positive cases on 4/27 with 987K cases in the US, 298K in NY and 111K in NJ.
- Both NY and NJ have reached the “peak plateau” in new cases, with a decline in cases definitely occurring in NY and a decline likely starting in NJ, although harder to say with fluctuations – the better indicator for NJ is likely hospitalization rates which are down from 8200 to 6400, statewide over the last 2 weeks. The big question for NY and eventually NJ is how quickly does the new case rate decline and to what level? Not known now. The US new case rate has been at a plateau for awhile, but may be starting to decline..
- NY now has done about 42K tests per 1MM in population, which is more than almost any other country; NJ is at 25K tests per 1MM and the US is at 17K tests per 1MM, both of which are middle-of-the-pack (vs. countries with major outbreaks). As discussed elsewhere, though, it’s not total tests that is critical – it’s testing very aggressively early in an outbreak so that it can be controlled – when that is done, the ratio of positives to tests is low (<10%) and that never happened in the US or Europe as we feel way behind the oubreak. Fortunately, NY/NYC positives are now down around 20% of total tests from a long plateau in the 40-50% range. NJ positive tests have finally dropped below 40% from a long time at near 50% positive.
- Total number of hospitalized in NY continues to decline steadily.
- Currently, this is the first day I’ve seen where new cases didn’t jump more than 10% anywhere in the US which is great.
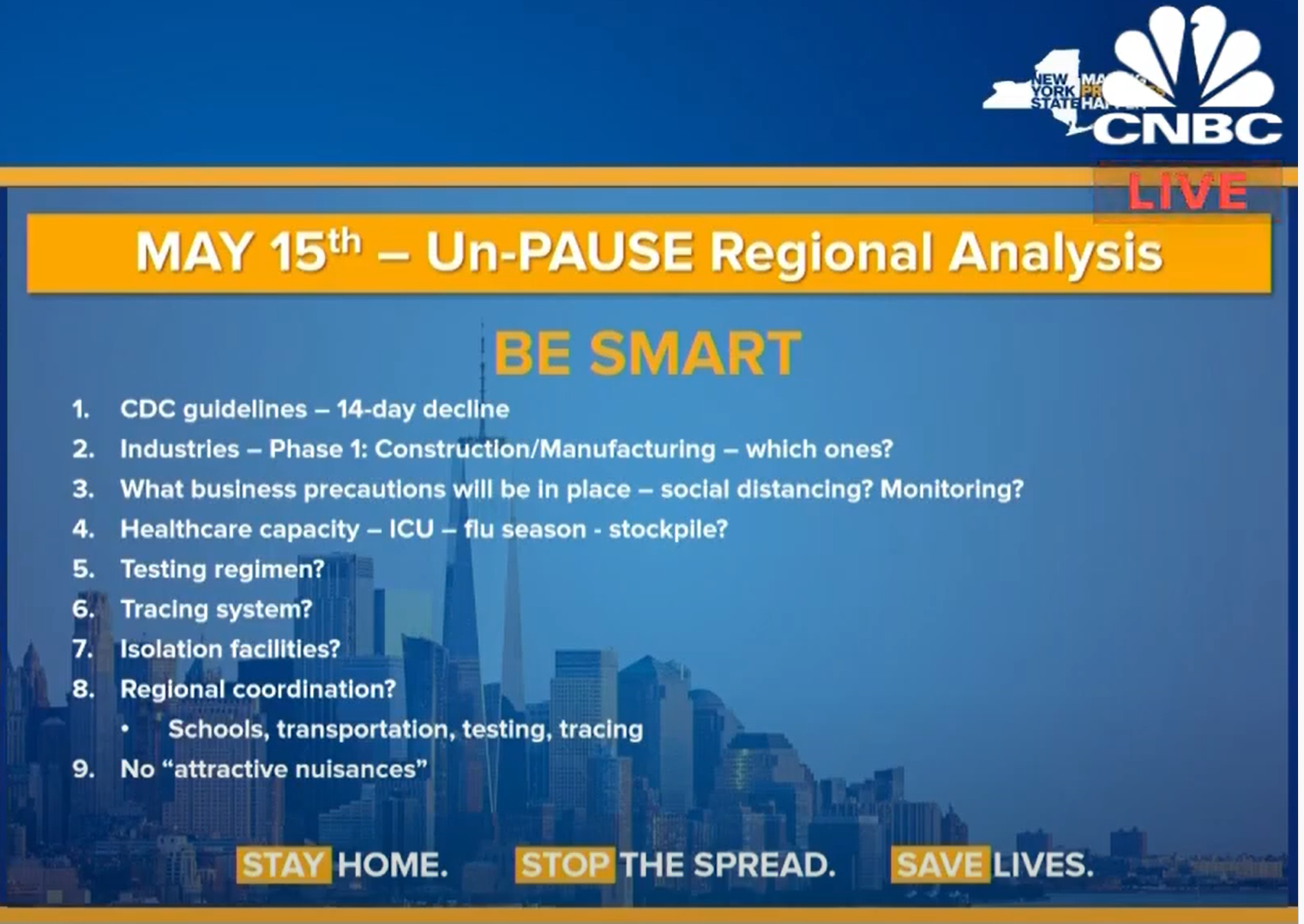
- Cuomo talked at length on the regional path back to the “new normal,” hopefully unpausing on 5/15, if they meet the CDC guidance for reopening: a 14-day decline in cases with testing/tracing/isolation: “Test – Trace – Isolate” is the slogan. he major focus on the need for fast, massive testing for the virus, to know who is sick or getting sick, so they can be quarantined and their contacts traced, as well as massive antibody testing to know who already has had the virus and now likely has immunity, at least for months to maybe years.
- Cuomo shared updated results from their testing of thousands of people from a random, somewhat representative sample (people who were out and about in stores, so it may be an overestimate) of the population (7500 so far), to estimate the percentage of people in NY who have had the virus: 1.5% of NY has tested positive by the virus test and preliminary antibody tests show that 14.9% of NYers (13.9% 5 days ago) have antibodies, while 24.1% of NYC residents have antibodies (21% 5 days ago). He also said antibody testing of police, firefighters and health care workers is also being done this week. Note that the WHO guidance didn’t say no antibodies = no immunity – it said we just can’t be sure, yet about extent and length of immunity until more research is done.
- The antibody results also might mean the R0 is very high (5.7 as recently postulated) and that up to 80% of the US/world could become infected if we do nothing, killing hundreds of thousands in the US alone, even if this means the current 7.5% case fatality rate in NY (22.6K deaths/298K positives) can now finally be translated to an infection fatality rate of 0.7% (22.6K/2.98MM w/antibodies) – and even if nobody else died in NY and 80% were infected, that would still be an IFR of 0.14% (22.6K deaths/16MM). If that IFR holds for the rest of the US (no reason to think a viral IFR would be very different across states, unlike the CFR which is very dependent on testing) and 80% of the US became infected if we did nothing (as we’ve seen in the Ohio prison), that would translate to 330MM x 0.8 x 0.007 = 1.8MM deaths. That’s why we need testing/tracing/isolating and social distancing until we have a proven treatment or vaccine to prevent a calamity. It’s likely the IFR will continue to decline and the infected % won’t really reach 80%, but even with an IFR of 0.1-0.2%; flu is ~0.1%) and 60% infected, that’s still 200-400K dead if we do nothing – these were essentially the original arguments for interventions before the outbreak, which way too many downplayed.
- Cuomo rightly continued to slam Senate Majority Leader McConnell’s repugnant statements about not funding states hardest hit by this virus, including funds for health care workers, fire, police, schools, etc., because they’re “blue states.” He also showed how NY/NJ have always given far more to the Federal budget than we get back: NY and NJ provide $29BB and $18BB more to the Federal Government per year than we get back (#1 and #2), while KY gets $37BB more back from the Feds than they give (#3). Not quite fair for Mitch to be holding blue states hostage.

Last edited:
Some promising stuff out of the Jenner Institute at Oxford.
“In the worldwide race for a vaccine to stop the coronavirus, the laboratory sprinting fastest is at Oxford University.
Most other teams have had to start with small clinical trials of a few hundred participants to demonstrate safety. But scientists at the university’s Jenner Institute had a head start on a vaccine, having proved in previous trials that similar inoculations — including one last year against an earlier coronavirus — were harmless to humans.
That has enabled them to leap ahead and schedule tests of their new coronavirus vaccine involving more than 6,000 people by the end of next month, hoping to show not only that it is safe, but also that it works.
The Oxford scientists now say that with an emergency approval from regulators, the first few million doses of their vaccine could be available by September — at least several months ahead of any of the other announced efforts — if it proves to be effective.
Now, they have received promising news suggesting that it might.
Scientists at the National Institutes of Health’s Rocky Mountain Laboratory in Montana last month inoculated six rhesus macaque monkeys with single doses of the Oxford vaccine. The animals were then exposed to heavy quantities of the virus that is causing the pandemic — exposure that had consistently sickened other monkeys in the lab. But more than 28 days later all six were healthy, said Vincent Munster, the researcher who conducted the test.
“The rhesus macaque is pretty much the closest thing we have to humans,” Dr. Munster said, noting that scientists were still analyzing the result. He said he expected to share it with other scientists next week and then submit it to a peer-reviewed journal.”
#s: Do you think the US pharmaceuticals only jump in with this drug if they can only get worldwide exclusivity?
https://www.nytimes.com/2020/04/27/...action=click&module=Spotlight&pgtype=Homepage
Was just about to post this, thanks. I think any pharma company with significant manufacturing capability is going to jump in to help with little regard to cost or profit. This is much bigger than $$ (and of course, saving humanity looks good and creates good will). Merck makes very little $$ on the Ebola vaccine and makes nothing off its donations of ivermectin (antifungal) to cure River Blindness in Africa and other large pharma companies have done similar things.
I'd also love to see the Brits win the race over the Chinese on this (if the US doesn't), although I'll take any vaccine success at this point. One interesting side angle is that testing the vaccine will likely be much easier in the UK with an ongoing outbreak vs. China, who has controlled theirs. The more I hear the more likely I think my prediction of a commercial vaccine before the end of the year will be realized. Crossing fingers...
https://rutgers.forums.rivals.com/t...social-distancing.191275/page-82#post-4523426
Last edited:
Was just about to post this, thanks. I think any pharma company with significant manufacturing capability is going to jump in to help with little regard to cost or profit. This is much bigger than $$ (and of course, saving humanity looks good and creates good will). Merck makes very little $$ on the Ebola vaccine and makes nothing off its donations of ivermectin (antifungal) to cure River Blindness in Africa and other large pharma companies have done similar things.
Thanks. Hope your comments hold true regarding Big Pharma. This same article stated:
“But the team has not yet reached an agreement with a North American manufacturer, in part because the major pharmaceutical companies there typically demand exclusive worldwide rights before investing in a potential medicine.
“I personally don’t believe that in a time of pandemic there should be exclusive licenses,” Professor Hill said. “So we are asking a lot of them. Nobody is going to make a lot of money off this.”
Seems like Covid19 would outweigh the efforts for Ebola if not for the simple fact that the COVID pandemic has made a greater impression on the industrialized parts of the world unlike Ebola which to my knowledge has been relegated to mostly underdeveloped parts of the world.
GO RU
Thanks. Hope your comments hold true regarding Big Pharma. This same article stated:
“But the team has not yet reached an agreement with a North American manufacturer, in part because the major pharmaceutical companies there typically demand exclusive worldwide rights before investing in a potential medicine.
“I personally don’t believe that in a time of pandemic there should be exclusive licenses,” Professor Hill said. “So we are asking a lot of them. Nobody is going to make a lot of money off this.”
Seems like Covid19 would outweigh the efforts for Ebola if not for the simple fact that the COVID pandemic has made a greater impression on the industrialized parts of the world unlike Ebola which to my knowledge has been relegated to mostly underdeveloped parts of the world.
GO RU
They will - I wouldn't worry about that. The biggest issue for a company that might just do the manufacturing of a vaccine might be choosing which one if there are several that work in the trials. I doubt anyone wants to commit yet to any specific vaccine as it's just too early. I know that expanding vaccine manufacturing capability is being looked at by the major manufacturers in this area already.
Article on a Manhattan Project to address the virus:
https://www.wsj.com/articles/the-se...a-covid-19-plan-11587998993?mod=hp_lead_pos12
Most interesting quote-
In a group call afterward, one of the scientists said, of the FDA: “They’re the problem here.”
https://www.wsj.com/articles/the-se...a-covid-19-plan-11587998993?mod=hp_lead_pos12
Most interesting quote-
In a group call afterward, one of the scientists said, of the FDA: “They’re the problem here.”
Isn't the Bill and Melinda Gates foundation spending billions to spin up manufacturing sites so that I've a vaccine is ready to go, they'll be able to quickly ramp up production?
- Status
- Not open for further replies.
Similar threads
- Replies
- 93
- Views
- 3K
- Replies
- 8
- Views
- 1K
- Replies
- 7
- Views
- 729
- Replies
- 0
- Views
- 1K
ADVERTISEMENT
ADVERTISEMENT