Those graphs are Ft. Lauderdale specific?Not according to the data...

Colleges
- AAC
- ACC
- Big 12
- Big East
- Big Ten
- Pac-12
- SEC
- Atlantic 10
- Conference USA
- Independents
- Junior College
- Mountain West
- Sun Belt
- MAC
- More
- Navy
- UAB
- Tulsa
- UTSA
- Charlotte
- Florida Atlantic
- Temple
- Rice
- East Carolina
- USF
- SMU
- North Texas
- Tulane
- Memphis
- Miami
- Louisville
- Virginia
- Syracuse
- Wake Forest
- Duke
- Boston College
- Virginia Tech
- Georgia Tech
- Pittsburgh
- North Carolina
- North Carolina State
- Clemson
- Florida State
- Cincinnati
- BYU
- Houston
- Iowa State
- Kansas State
- Kansas
- Texas
- Oklahoma State
- TCU
- Texas Tech
- Baylor
- Oklahoma
- UCF
- West Virginia
- Wisconsin
- Penn State
- Ohio State
- Purdue
- Minnesota
- Iowa
- Nebraska
- Illinois
- Indiana
- Rutgers
- Michigan State
- Maryland
- Michigan
- Northwestern
- Arizona State
- Oregon State
- UCLA
- Colorado
- Stanford
- Oregon
- Arizona
- California
- Washington
- USC
- Utah
- Washington State
- Texas A&M
- Auburn
- Mississippi State
- Kentucky
- South Carolina
- Arkansas
- Florida
- Missouri
- Ole Miss
- Alabama
- LSU
- Georgia
- Vanderbilt
- Tennessee
- Louisiana Tech
- New Mexico State
- Middle Tennessee
- Western Kentucky
- UTEP
- Florida International University
High School
- West
- Midwest
- Northeast
- Southeast
- Other
- Alaska
- Arizona
- California
- Colorado
- Nevada
- New Mexico
- Northern California
- Oregon
- Southern California Preps
- Washington
- Edgy Tim
- Indiana
- Kansas
- Nebraska
- Iowa
- Michigan
- Minnesota
- Missouri
- Oklahoma Varsity
- Texas Basketball
- Texas
- Wisconsin
- Delaware
- Maryland
- New Jersey Basketball
- New Jersey
- New York City Basketball
- Ohio
- Pennsylvania
- Greater Cincinnati
- Virginia
- West Virginia Preps
ADVERTISEMENT
Install the app
How to install the app on iOS
Follow along with the video below to see how to install our site as a web app on your home screen.
Note: This feature may not be available in some browsers.
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
COVID-19 Pandemic: Transmissions, Deaths, Treatments, Vaccines, Interventions and More...
- Thread starter RU848789
- Start date
- Status
- Not open for further replies.

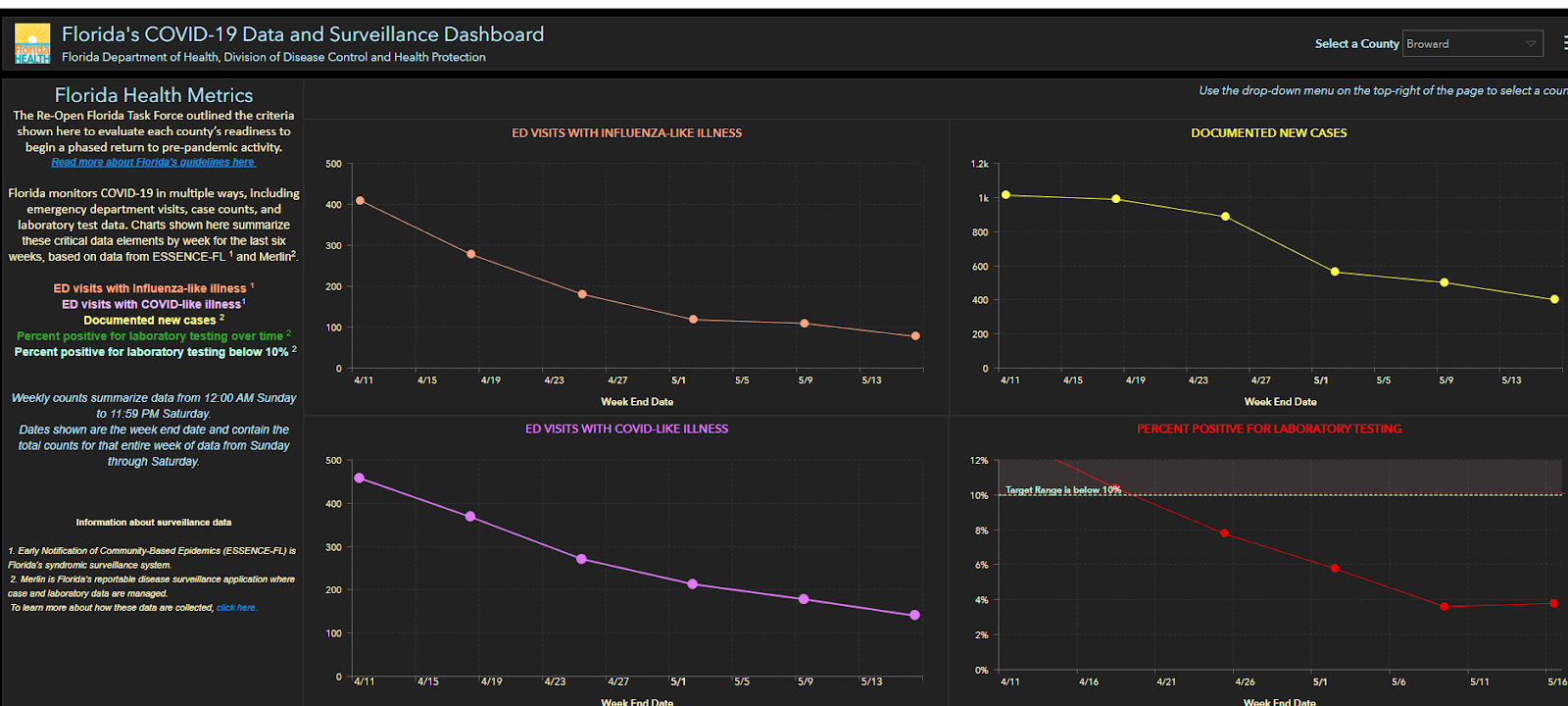
Again- her correspondence with me is not an assertion on the entire state but for the FtL area.
Broward County, I highly doubt the whole county dropped from 450 to around 150 ED visits due to CV19 while Fort Lauderdale got worse. If you believe that then ....Those graphs are Ft. Lauderdale specific?
Those graphs I replied to you are from Broward County, home of Ft Lauderdale. There is no way what she said is accurate according to the data. No way.Again- her correspondence with me is not an assertion on the entire state but for the FtL area.
Maybe the distinction is a month ago many people were visiting the ED but were not in need of being hospitalized?Broward County, I highly doubt the whole county dropped from 450 to around 150 ED visits due to CV19 while Fort Lauderdale got worse. If you believe that then ....
Could be why the Flu ED visits were so high a month ago as well.
Edit: Ya looked into it a little, and FL(unlike NJ) does not list current hospitalizations. So I don't think we can definitely say that current Ft. Lauderdale hospitalizations have dropped. Not from that graph anyways.
Florida actually does a couple things on their dashboard which suggests they are trending downward, when that might not be accurate.
Last edited:
Remember, my post had 2 points. You just agreed with the first one that the LTC dynamic is skewing the current results and the fatality rate will decrease. Thank you.
However, you forgot to address the second, which makes your post above meaningless. Death numbers are starting to be independently investigated and revised. CO just decreased their state death count. We know NY and NJ data includes many patients that did not die due to corona. Once a national standard is set, we will know the true data to use.
Actually, he didn't agree with your first point. He said it was possible.
As to your second point, arguing cause of death is pointless. For one thing, while there may be patients whose deaths were not directly attributed to Covid-19, there are also deaths not attributed. My wife's aunt, who died in March in a nursing home, perfectly fits the profile but because she was, for all intents and purposes, Patient #1 in that facility she wasn't tested and we didn't have the time to either realize what was going on or demand that she be tested.
Also, you guys (and you know who I mean) are all running around talking about "The Pandemic of 1968" - which was a flu pandemic. One thing that we certainly know about high death counts from the flu is that they're always way overestimated.
So you can't have it both ways. If you want to stipulate that the death count from C-19 is, say, half of what is being presented then you have to stipulate to the same with regard to H3N2.
Or, you could just accept all the numbers for what they are. We'll give you the 100k deaths in 1968 and you admit that the death toll from C-19 is going to be easily 3x that.
T2K - you are relentlessly deflective and illogical, but that's your game. It's barely worth arguing with you, especially as you're doing what your leadership is good at - focusing on largely inconsequential details to obscure the far larger problem of a pandemic aimed at killing 1MM+ in the US. I didn't "agree" with your point on the early outbreak data potentially containing bias (unintentional) - as 4Real said, I said it was possible.
However, the important point is that even if the IFR eventually is as low as 0.5%, which is pretty unlikely given it's now at 1.0-1.2% in the three locations with antibody testing (0.7-0.9% seems much more likely), that's still 5X the IFR of the flu and 60% infection rate is 5.6X the infection rate per year we see in flu (where only 10% are infected per year; roughly 35K dead in 35MM infected) and 28 x 35K/year is 980K deaths per year (if it were a year - could take 2 years), which is very close to the calculation I had above or 990K, which is basically 1MM.
And you're going to try to argue that the reported death rates are too high? Almost nobody thinks that other than you. Even the CDC, which has become a shell of itself under Redfield, published the NYC numbers on excess deaths essentially saying the actual deaths from coronavirus are likely several thousand greater than what has been reported, which would bring the NYC IFR to 1.4% as per Worldometers), as per below. I think that is too high, but there's little doubt the "presumed deaths" most of which occurred in hospitals with patients with all COVID symptoms (and doing the confirming viral test was unnecessary and is dangerous to the staff, so they sometimes skipped it), were due to COVID.
Actual Deaths (23,000: almost twice the number of confirmed deaths)
As of May 1, New York City reported 13,156 confirmed deaths and 5,126 probable deaths (deaths with COVID-19 on the death certificate but no laboratory test performed), for a total of 18,282 deaths [source]. The CDC on May 11 released its "Preliminary Estimate of Excess Mortality During the COVID-19 Outbreak — New York City, March 11–May 2, 2020" [source] in which it calculated an estimate of actual COVID-19 deaths in NYC by analyzing the "excess deaths" (defined as "the number of deaths above expected seasonal baseline levels, regardless of the reported cause of death") and found that, in addition to the confirmed and probable deaths reported by the city, there were an estimated 5,293 more deaths to be attributed. After adjusting for the previous day (May 1), we get 5,148 additional deaths, for a total of actual deaths of 13,156 confirmed + 5,126 probable + 5,148 additional excess deaths calculated by CDC = 23,430 actual COVID-19 deaths as of May 1, 2020 in New York City.
Infection Fatality Rate (23k / 1.7M = 1.4% IFR)
Actual Cases with an outcome as of May 1 = estimated actual recovered (1,671,351) + estimated actual deaths (23,430) = 1,694,781.
Infection Fatality Rate (IFR) = Deaths / Cases = 23,430 / 1,694,781 = 1.4% (1.4% of people infected with SARS-CoV-2 have a fatal outcome, while 98.6% recover).
https://www.worldometers.info/coronavirus/coronavirus-death-rate/
It will definitely be lower than 0.5%. Let's see how things go with count revisions and as new cases come more from the general pop and not LTC. Our LTC pop in the US is only 0.4%, but currently accounts for 11% of all confirmed cases and 40% of deaths. This will change over time.T2K - you are relentlessly deflective and illogical, but that's your game. It's barely worth arguing with you, especially as you're doing what your leadership is good at - focusing on largely inconsequential details to obscure the far larger problem of a pandemic aimed at killing 1MM+ in the US. I didn't "agree" with your point on the early outbreak data potentially containing bias (unintentional) - as 4Real said, I said it was possible.
However, the important point is that even if the IFR eventually is as low as 0.5%, which is pretty unlikely given it's now at 1.0-1.2% in the three locations with antibody testing (0.7-0.9% seems much more likely), that's still 5X the IFR of the flu and 60% infection rate is 5.6X the infection rate per year we see in flu (where only 10% are infected per year; roughly 35K dead in 35MM infected) and 28 x 35K/year is 980K deaths per year (if it were a year - could take 2 years), which is very close to the calculation I had above or 990K, which is basically 1MM.
And you're going to try to argue that the reported death rates are too high? Almost nobody thinks that other than you. Even the CDC, which has become a shell of itself under Redfield, published the NYC numbers on excess deaths essentially saying the actual deaths from coronavirus are likely several thousand greater than what has been reported, which would bring the NYC IFR to 1.4% as per Worldometers), as per below. I think that is too high, but there's little doubt the "presumed deaths" most of which occurred in hospitals with patients with all COVID symptoms (and doing the confirming viral test was unnecessary and is dangerous to the staff, so they sometimes skipped it), were due to COVID.
Actual Deaths (23,000: almost twice the number of confirmed deaths)
As of May 1, New York City reported 13,156 confirmed deaths and 5,126 probable deaths (deaths with COVID-19 on the death certificate but no laboratory test performed), for a total of 18,282 deaths [source]. The CDC on May 11 released its "Preliminary Estimate of Excess Mortality During the COVID-19 Outbreak — New York City, March 11–May 2, 2020" [source] in which it calculated an estimate of actual COVID-19 deaths in NYC by analyzing the "excess deaths" (defined as "the number of deaths above expected seasonal baseline levels, regardless of the reported cause of death") and found that, in addition to the confirmed and probable deaths reported by the city, there were an estimated 5,293 more deaths to be attributed. After adjusting for the previous day (May 1), we get 5,148 additional deaths, for a total of actual deaths of 13,156 confirmed + 5,126 probable + 5,148 additional excess deaths calculated by CDC = 23,430 actual COVID-19 deaths as of May 1, 2020 in New York City.
Infection Fatality Rate (23k / 1.7M = 1.4% IFR)
Actual Cases with an outcome as of May 1 = estimated actual recovered (1,671,351) + estimated actual deaths (23,430) = 1,694,781.
Infection Fatality Rate (IFR) = Deaths / Cases = 23,430 / 1,694,781 = 1.4% (1.4% of people infected with SARS-CoV-2 have a fatal outcome, while 98.6% recover).
https://www.worldometers.info/coronavirus/coronavirus-death-rate/
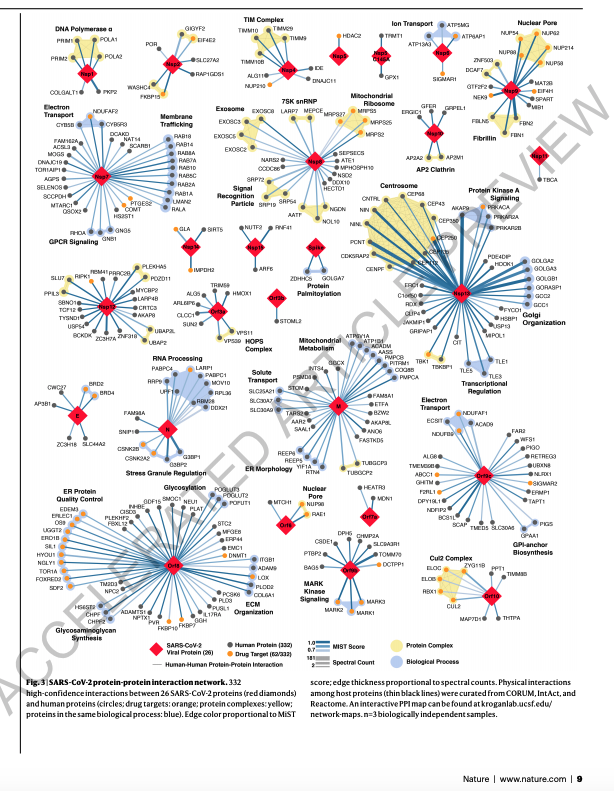
Another way to attack the virus - we went over this new paper in our weekly COVID-19 discussion group that was published in Nature a few days ago: "A SARS-CoV-2 protein interaction map reveals targets for drug repurposing". Very interesting - I thought folks might be interested in a summary.
A huge group of scientists worked together to figure out what human proteins interact with the virus proteins. Keep in mind, a virus hijacks the functions of our cells when it invades. This is the only way a virus can make copies of itself and go on to infect other cells and other people. Kind of like a burglar who breaks into your house, but then is hungry and thirsty so he eats your food, drinks your wine and then realizes he doesn't even have a way to get the stolen stuff home - so he takes your wheelbarrow, too!
OK, so in the figure below (no need to read the small text, just look a the image) the red diamonds are the individual virus proteins. Each line from each red diamond connects to a human protein that the scientists, experimentally, found interacted with the virus protein. This is called an "interactome".
The main point of this image is to show how damn complex this all is and how much we still have to learn, but it also shows potential ways to fight the virus, as shown in the next figure.
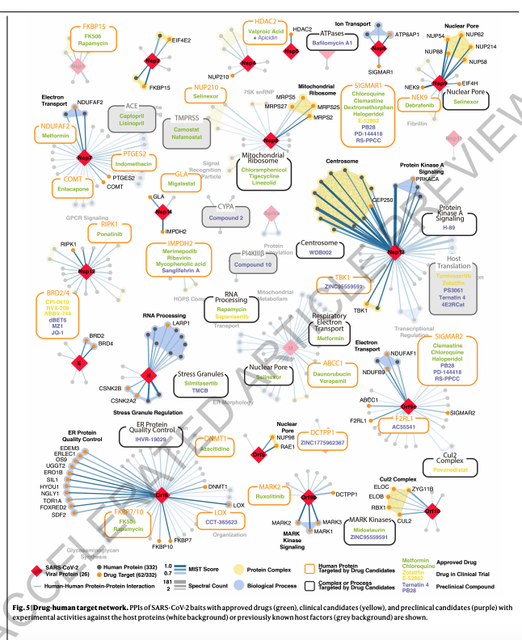
The second image below is the good news. This is the same image from above, but now the scientists have added in the names of drugs that target the function of the human proteins (not the virus proteins).
These drugs (all approved for use in people) might block the function of human proteins that are essential for the virus to survive and make copies of itself. In other words, no wheelbarrow for the burglar, so not much damage is done.
Several of these drugs were tested by the scientists and were shown to impact the virus. This provides a large new set of potential drugs that might stop COVID-19 and they are already used in people. Lots of work to be done, but I thought this was very cool.
A huge group of scientists worked together to figure out what human proteins interact with the virus proteins. Keep in mind, a virus hijacks the functions of our cells when it invades. This is the only way a virus can make copies of itself and go on to infect other cells and other people. Kind of like a burglar who breaks into your house, but then is hungry and thirsty so he eats your food, drinks your wine and then realizes he doesn't even have a way to get the stolen stuff home - so he takes your wheelbarrow, too!
OK, so in the figure below (no need to read the small text, just look a the image) the red diamonds are the individual virus proteins. Each line from each red diamond connects to a human protein that the scientists, experimentally, found interacted with the virus protein. This is called an "interactome".
The main point of this image is to show how damn complex this all is and how much we still have to learn, but it also shows potential ways to fight the virus, as shown in the next figure.
The second image below is the good news. This is the same image from above, but now the scientists have added in the names of drugs that target the function of the human proteins (not the virus proteins).
These drugs (all approved for use in people) might block the function of human proteins that are essential for the virus to survive and make copies of itself. In other words, no wheelbarrow for the burglar, so not much damage is done.
Several of these drugs were tested by the scientists and were shown to impact the virus. This provides a large new set of potential drugs that might stop COVID-19 and they are already used in people. Lots of work to be done, but I thought this was very cool.
Wow, this is by far the most clear and logical analysis of the numbers I have seen. What is still in flux with these calculations is how the IFR will be improved by the improved care patients will receive now that doctors have, unfortunately, had a lot of practice. On the flip side, the IFR could get much worse as the virus hits areas that have much less access to ICUs.
Thanks for taking the time to post.
Thanks, especially coming from someone who knows what's going on. Believe it or not, I was trying to be brief, lol, so didn't go into a number of other qualifiers and you're absolutely right that we should now be better at this medically in areas that have a lot of experience, whereas other areas might do worse.
Another new variable is convalescent plasma: over 11,000 patients, mostly seriously ill ones (and there are only currently 16.3K "serious/critical" cases in the US, have been infused and if preliminary indications of "significant" reductions in mortality are confirmed (seen in the ~3361 ICU cases from the paper I posted the other day, although it's not a controlled study and no formal efficacy claims are being made - yet), that would put a significant dent in the IFR, eventually, which is great.
Show your work - if the LTC population is 0.4% of 330MM, that's 1.32MM vs. your 40% of 90K deaths, which is only 36K deaths out of 1.32MM (2.7%) - how does that mean there aren't a lot more deaths to go in the LTC population? Count revisions are also much more likely to move the IFR up not down and while it's a reasonable hypothesis that a greater percentage of vulnerable people were hit in the first wave than might be hit in the future, I've seen no study showing that to be true.It will definitely be lower than 0.5%. Let's see how things go with count revisions and as new cases come more from the general pop and not LTC. Our LTC pop in the US is only 0.4%, but currently accounts for 11% of all confirmed cases and 40% of deaths. This will change over time.
Also, the large number of states that haven't been hit hard yet also means their vulnerable people haven't been hit hard yet - but hopefully we have learned some lessons about reducing transmissions in LTC facilities, although given that we don't appear to have learned much from the hard hit states in the lesser impacted states that are prematurely opening up, that might not hold true.
https://www.nature.com/articles/s41586-020-2286-9_reference.pdfAnother way to attack the virus - we went over this new paper in our weekly COVID-19 discussion group that was published in Nature a few days ago: "A SARS-CoV-2 protein interaction map reveals targets for drug repurposing". Very interesting - I thought folks might be interested in a summary.
A huge group of scientists worked together to figure out what human proteins interact with the virus proteins. Keep in mind, a virus hijacks the functions of our cells when it invades. This is the only way a virus can make copies of itself and go on to infect other cells and other people. Kind of like a burglar who breaks into your house, but then is hungry and thirsty so he eats your food, drinks your wine and then realizes he doesn't even have a way to get the stolen stuff home - so he takes your wheelbarrow, too!
OK, so in the figure below (no need to read the small text, just look a the image) the red diamonds are the individual virus proteins. Each line from each red diamond connects to a human protein that the scientists, experimentally, found interacted with the virus protein. This is called an "interactome".
The main point of this image is to show how damn complex this all is and how much we still have to learn, but it also shows potential ways to fight the virus, as shown in the next figure.
The second image below is the good news. This is the same image from above, but now the scientists have added in the names of drugs that target the function of the human proteins (not the virus proteins).
These drugs (all approved for use in people) might block the function of human proteins that are essential for the virus to survive and make copies of itself. In other words, no wheelbarrow for the burglar, so not much damage is done.
Several of these drugs were tested by the scientists and were shown to impact the virus. This provides a large new set of potential drugs that might stop COVID-19 and they are already used in people. Lots of work to be done, but I thought this was very cool.
I am having flashbacks seeing the evaluation of PD-144418...
Powerful article and data.
The Case for Reopening Schools
Lots of other countries have decided that it's time to take this step. Why is the US holding back?
"It would seem more rational to start by getting kids in school, then sending parents back to work."
https://www.wired.com/story/the-case-for-reopening-schools/
The Case for Reopening Schools
Lots of other countries have decided that it's time to take this step. Why is the US holding back?
"It would seem more rational to start by getting kids in school, then sending parents back to work."
https://www.wired.com/story/the-case-for-reopening-schools/
Powerful article and data.
The Case for Reopening Schools
Lots of other countries have decided that it's time to take this step. Why is the US holding back?
"It would seem more rational to start by getting kids in school, then sending parents back to work."
https://www.wired.com/story/the-case-for-reopening-schools/
Welcome to the grown-ups table. Thought provoking article. You may recall my "plan" from many weeks ago where I thought the best thing we could do was to quarantine everyone of school age in school for 3-4 weeks with some under 25 teachers/chaperones (at low risk), so they could reach herd immunity and not be a vector for future infections. Ethically nobody would've done it, but we could have probably taken 15-20% of the population off the table for infecting others by doing that.
Given where we are today and the very conflicting evidence on children under 18 and how infectious they are when they become infected (link below has a lot more examples of concerning data), my thinking would be to wait a few weeks and see how the "experiments" in some of these other countries go and if they look pretty good, then let's do it here, too.
https://www.businessinsider.com/can-children-spread-the-coronavirus-to-others-evidence-2020-5
Some details in the Oxford Vaccine. Definitely one of the vaccine candidates that could be ready by year end.
https://news.sky.com/story/coronavi...ed-and-when-will-we-know-if-it-works-11990155
https://news.sky.com/story/coronavi...tember-if-trial-succeeds-says-sharma-11990039
https://news.sky.com/story/coronavi...ed-and-when-will-we-know-if-it-works-11990155
https://news.sky.com/story/coronavi...tember-if-trial-succeeds-says-sharma-11990039
Seriously? Gotta read something to recall it.You may recall my "plan" from many weeks ago where I thought the best thing we could do was to quarantine everyone of school age in school for 3-4 weeks with some under 25 teachers/chaperones (at low risk), so they could reach herd immunity and not be a vector for future infections. Ethically nobody would've done it, but we could have probably taken 15-20% of the population off the table for infecting others by doing that.
Given where we are today and the very conflicting evidence on children under 18 and how infectious they are when they become infected (link below has a lot more examples of concerning data), my thinking would be to wait a few weeks and see how the "experiments" in some of these other countries go and if they look pretty good, then let's do it here, too.
https://www.businessinsider.com/can-children-spread-the-coronavirus-to-others-evidence-2020-5
:)
Based on this data, doesn't seem to be any legit reason for not starting back up the normal school operation.
Two more clinical trials showing no efficacy for HCQ, as well as statistically significant side effects in one of the studies. The weight of evidence against HCQ efficacy in moderately to severely ill patients in a hospital setting has become nearly overwhelming. And recall, these were the kinds of patients that Dr. Raoult had studied and said were "cured" by reducing viral loads to zero, which was the basis for the late March barrage by many (including the POTUS) touting HCQ as a cure. We await results from prophylactic treatment and treatment of mildly ill patients early in their infections.
The first HCQ study was an observational one with a control arm, but not blinded, and was conducted in France in patients with low oxygen levels. Among the 181 patients eligible for analysis, 84 received HCQ within 48 hours of admission, eight received HCQ more than 48 hours after admission, and 89 did not receive HCQ at all. Also, apart from azithromycin in some patients, the patients in this study did not receive any other drugs; in particular, potential confounders such as antiviral and anti-inflammatory treatments, including steroids, before admission to intensive care (which was one of the primary endpoints). Here are the conclusions from this peer-reviewed study.
https://www.bmj.com/content/369/bmj.m1844
Conclusions: In patients admitted to hospital with covid-19 pneumonia who require oxygen, hydroxychloroquine treatment seemed to have no effect on reducing admissions to intensive care or deaths at day 21 after hospital admission. Additionally, hydroxychloroquine treatment did not have any effect on survival without acute respiratory distress syndrome at day 21 after hospital admission. These results do not support the use of hydroxychloroquine in these patients.
The second HCQ study was a standard-of-care controlled, randomized (but open label) study conducted in China evaluating HCQ in mild to moderately ill patients in a hospital setting, in which 150 patients admitted to the hospital with COVID-19 were randomly split into two equal-sized 75 patient groups assigned to receive either HCQ plus standard of care or standard of care alone. This study showed that HCQ did not clear the virus more quickly than those receiving standard care and showed that adverse events were higher in those who received hydroxychloroquine.
https://www.bmj.com/content/369/bmj...=hootsuite&utm_content=sme&utm_campaign=usage
Conclusion and policy implications
The results of our trial did not show additional benefits of virus elimination from adding hydroxychloroquine to the current standard of care in patients with mainly persistent mild to moderate covid-19. Adverse events, particularly gastrointestinal events, were more frequently reported in patients receiving hydroxychloroquine, who were given a loading dose of 1200 mg daily for three days followed by a maintenance dose of 800 mg daily for the remaining days for a total treatment duration of two weeks in patients with mild to moderate disease and three weeks in those with severe disease. Overall, these data do not support the addition of hydroxychloroquine to the current standard of care in patients with persistent mild to moderate covid-19 for eliminating the virus. Our trial may provide initial evidence for the benefit-risk profile of hydroxychloroquine and serve as a resource to support further research.
The first HCQ study was an observational one with a control arm, but not blinded, and was conducted in France in patients with low oxygen levels. Among the 181 patients eligible for analysis, 84 received HCQ within 48 hours of admission, eight received HCQ more than 48 hours after admission, and 89 did not receive HCQ at all. Also, apart from azithromycin in some patients, the patients in this study did not receive any other drugs; in particular, potential confounders such as antiviral and anti-inflammatory treatments, including steroids, before admission to intensive care (which was one of the primary endpoints). Here are the conclusions from this peer-reviewed study.
https://www.bmj.com/content/369/bmj.m1844
Conclusions: In patients admitted to hospital with covid-19 pneumonia who require oxygen, hydroxychloroquine treatment seemed to have no effect on reducing admissions to intensive care or deaths at day 21 after hospital admission. Additionally, hydroxychloroquine treatment did not have any effect on survival without acute respiratory distress syndrome at day 21 after hospital admission. These results do not support the use of hydroxychloroquine in these patients.
The second HCQ study was a standard-of-care controlled, randomized (but open label) study conducted in China evaluating HCQ in mild to moderately ill patients in a hospital setting, in which 150 patients admitted to the hospital with COVID-19 were randomly split into two equal-sized 75 patient groups assigned to receive either HCQ plus standard of care or standard of care alone. This study showed that HCQ did not clear the virus more quickly than those receiving standard care and showed that adverse events were higher in those who received hydroxychloroquine.
https://www.bmj.com/content/369/bmj...=hootsuite&utm_content=sme&utm_campaign=usage
Conclusion and policy implications
The results of our trial did not show additional benefits of virus elimination from adding hydroxychloroquine to the current standard of care in patients with mainly persistent mild to moderate covid-19. Adverse events, particularly gastrointestinal events, were more frequently reported in patients receiving hydroxychloroquine, who were given a loading dose of 1200 mg daily for three days followed by a maintenance dose of 800 mg daily for the remaining days for a total treatment duration of two weeks in patients with mild to moderate disease and three weeks in those with severe disease. Overall, these data do not support the addition of hydroxychloroquine to the current standard of care in patients with persistent mild to moderate covid-19 for eliminating the virus. Our trial may provide initial evidence for the benefit-risk profile of hydroxychloroquine and serve as a resource to support further research.
Some encouraging results from a retrospective analysis of patient data (an attempt to "control" the comparison was made after the fact, as is standard for these kinds of analyses, and it's a preprint, so a grain of salt is required here) for patients treated with Tocilizumab plus standard of care vs. standard of care, showing a small potential decrease in mortality for those with acute respiratory distress syndrome (ARDS). The study looked at a total of 94 patients with COVID-19 (with ARDS), in which 44 were in the study group, taking Tocilizumab, while 50 were in the control group, not taking Tocilizumab and where they tried to match both groups as closely as possible with regard to starting point and other treatments. Their conclusion is below. More to come...
https://www.medrxiv.org/content/10.1101/2020.05.13.20100081v1.full.pdf
CONCLUSION: Tocilizumab is a humanized monoclonal antibody against the in-terleukin-6 receptor (IL-6R) and is FDA-approved for cytokine release syndrome and recently, has been administered experimentally in the treatment of severe COVID-19 pneumonia in China and Italy with promising results16. Cytokine Release Syndrome (CRS) occurs in a large number of patients with severe COVID-19, which is also an important cause of death. IL- 6 is the key molecule of CRS, so Tocilizumab may be of value in improving outcomes. In our study Tocilizumab group seemed to have improved survival outcome. Results have to be interpreted with caution since this a retrospective study and mortality is affected by multiple, confounding factors. In the largest clinical trials database (clinicaltrials.gov) there are 35 ongoing studies registered around the world regarding the use of Tocilizumab in COVID-19 patients. We await the results of ongoing randomized controlled trials to definitely answer the question of whether Tocilizumab improves survival in COVID-19 ARDS patients.
https://www.medrxiv.org/content/10.1101/2020.05.13.20100081v1.full.pdf
CONCLUSION: Tocilizumab is a humanized monoclonal antibody against the in-terleukin-6 receptor (IL-6R) and is FDA-approved for cytokine release syndrome and recently, has been administered experimentally in the treatment of severe COVID-19 pneumonia in China and Italy with promising results16. Cytokine Release Syndrome (CRS) occurs in a large number of patients with severe COVID-19, which is also an important cause of death. IL- 6 is the key molecule of CRS, so Tocilizumab may be of value in improving outcomes. In our study Tocilizumab group seemed to have improved survival outcome. Results have to be interpreted with caution since this a retrospective study and mortality is affected by multiple, confounding factors. In the largest clinical trials database (clinicaltrials.gov) there are 35 ongoing studies registered around the world regarding the use of Tocilizumab in COVID-19 patients. We await the results of ongoing randomized controlled trials to definitely answer the question of whether Tocilizumab improves survival in COVID-19 ARDS patients.
heard the same from a nurse in Tampa, they had to open up a new covid wing last week.Admittedly this is not a statement on the entire state but I have a friend from HS who is a nurse in Ft Lauderdale. She says their hospital has seen a steady increase in cases and there has not been any sign of slowing in her area.
I agree with those who believe that administering HCQ to patients who are already circling the drain may be missing the point. I suspect its efficacy is in early stage disease, and perhaps as a prophylactic.
We'll find out soon, when the results of the UMN study are released.I agree with those who believe that administering HCQ to patients who are already circling the drain may be missing the point. I suspect its efficacy is in early stage disease, and perhaps as a prophylactic.
So NJ is testing less in recent weeks. The reason? Lack of interest from the public.
https://www.politico.com/states/new...rsey-rolled-out-testing-tracing-plans-1284088
https://www.politico.com/states/new...rsey-rolled-out-testing-tracing-plans-1284088
Moderna phase 1 vaccine. 8 for 8 in patients.
Phase 3 by July?
Phase 3 by July?
So NJ is testing less in recent weeks. The reason? Lack of interest from the public.
https://www.politico.com/states/new...rsey-rolled-out-testing-tracing-plans-1284088
I'm not sure I agree with "lack of interest from the public".
First, according to the state dashboard, the number of tests reported has increased every day for the past 5 days.
Second, I think there is still a lot of information out there that testing is limited to those showing severe symptoms, which limits who will even attempt to get tests. For example, the Somerset County website says "Because priority is being given to those who are exhibiting symptoms of the coronavirus, residents must have a valid doctor’s prescription." That will certainly discourage people who are asymptomatic or mildly symptomatic from getting a test. I would guess that many would not even bother to call a doctor for a prescription, if they believe they won't get one. This is especially true for those who previously tried to get tested and were denied by their doctor or test center, because they didn't meet the CDC testing criteria.
Third, I think there is not enough availability of the Rutgers saliva test. If I were mildly symptomatic or asymptomatic, and only mildly concerned, I would rather spit in a tube over having a swab stuck into my sinuses. If the state wants to increase testing rates, they need to make the easy saliva test more widely available, and let people know where it is available.
Fourth, at this point, the state also needs to ramp up antibody testing. And that also means that antibody testing sites need to indicate which antibody test they use, along with the specificity and sensitivity of those tests. I wouldn't bother getting an antibody test unless it was a highly accurate test like Roche or Abbott.
I'm not sure I agree with "lack of interest from the public".
First, according to the state dashboard, the number of tests reported has increased every day for the past 5 days.
Second, I think there is still a lot of information out there that testing is limited to those showing severe symptoms, which limits who will even attempt to get tests. For example, the Somerset County website says "Because priority is being given to those who are exhibiting symptoms of the coronavirus, residents must have a valid doctor’s prescription." That will certainly discourage people who are asymptomatic or mildly symptomatic from getting a test. I would guess that many would not even bother to call a doctor for a prescription, if they believe they won't get one. This is especially true for those who previously tried to get tested and were denied by their doctor or test center, because they didn't meet the CDC testing criteria.
Third, I think there is not enough availability of the Rutgers saliva test. If I were mildly symptomatic or asymptomatic, and only mildly concerned, I would rather spit in a tube over having a swab stuck into my sinuses. If the state wants to increase testing rates, they need to make the easy saliva test more widely available, and let people know where it is available.
Fourth, at this point, the state also needs to ramp up antibody testing. And that also means that antibody testing sites need to indicate which antibody test they use, along with the specificity and sensitivity of those tests. I wouldn't bother getting an antibody test unless it was a highly accurate test like Roche or Abbott.
Anecdotally, I’ve heard exactly what they said re: testing when I’ve visited the testing sites in Middlesex County. It seems they have the ability to test many many people but haven’t tested their capacity due to lack of public interest. When first opened it was nuts but now they are very slow in comparison and way under their caps.
https://www.cnbc.com/2020/05/18/mod...on-early-stage-coronavirus-vaccine-trial.htmlModerna phase 1 vaccine. 8 for 8 in patients.
Phase 3 by July?
Anecdotally, I’ve heard exactly what they said re: testing when I’ve visited the testing sites in Middlesex County. It seems they have the ability to test many many people but haven’t tested their capacity due to lack of public interest. When first opened it was nuts but now they are very slow in comparison and way under their caps.
My point above is that it is not lack of "public interest", but lack of "public awareness" that widespread testing is now available. For weeks we have heard that testing is limited and if you are asymptomatic or mildly symptomatic, then you can't get tested. Testing websites continue to indicate that testing is limited. If anyone can qualify to get tested now, that needs to be publicized.
Broward County, I highly doubt the whole county dropped from 450 to around 150 ED visits due to CV19 while Fort Lauderdale got worse. If you believe that then ....
If all Restrictions are removed in Florida right now you can see where the COVID Hospitalizations will be by the end of June. ( 66,000) Keeping it flat or declining is where we need it.
https://covidactnow.org/state/FL
I'm down with this article. I think this year is already screwed, but I'm ready to go back in September. What is going on right now should not be looked at as traditional home schooling or virtual learning. It's crisis learning and was thrown together on the fly. No matter how good it is, it can't replace face to face contact.Powerful article and data.
The Case for Reopening Schools
Lots of other countries have decided that it's time to take this step. Why is the US holding back?
"It would seem more rational to start by getting kids in school, then sending parents back to work."
https://www.wired.com/story/the-case-for-reopening-schools/
+1I'm down with this article. I think this year is already screwed, but I'm ready to go back in September. What is going on right now should not be looked at as traditional home schooling or virtual learning. It's crisis learning and was thrown together on the fly. No matter how good it is, it can't replace face to face contact.
Common sense post from an educational expert. We were told directly by our school that this is not "distance learning", but rather emergency learning. Such learning is more effective in the later grades, but still not a substitute for the real thing.
No reason other than fear to keep the schools closed. Makes no sense.
Moderna phase 1 vaccine. 8 for 8 in patients.
Phase 3 by July?
Sounds like it. And it looks like the lower does is doing well too which means it will be a lot easier to scale up.
The one thing I don’t understand is how important the “neutralizing antibodies” are and if they were hoping that to be found in everyone.
Edit: The data was only available for 8 people, not that it wasn’t found in everyone. So that’s good. The article below does a better job at summarizing the results.
“The vaccine also produced neutralizing antibodies against Covid-19 in at least eight participants, the company said. Experts have said neutralizing antibodies appear to be important in acquiring protection.”
https://www.biospace.com/article/moderna-s-preliminary-phase-i-covid-19-vaccine-data-is-positive/
Last edited:
I thinks it's important to note which types of testing. Antigen testing or molecular testing. From what I understand most testing is using antigen tests which give high false negatives. Are people with negative antigen tests gets a molecular test for confirmation? Otherwise we're in for trouble.My point above is that it is not lack of "public interest", but lack of "public awareness" that widespread testing is now available. For weeks we have heard that testing is limited and if you are asymptomatic or mildly symptomatic, then you can't get tested. Testing websites continue to indicate that testing is limited. If anyone can qualify to get tested now, that needs to be publicized.
Last edited:
I hope they don't remove all restrictions as they would seem like a bad decision based upon projections.If all Restrictions are removed in Florida right now you can see where the COVID Hospitalizations will be by the end of June. ( 66,000) Keeping it flat or declining is where we need it.
https://covidactnow.org/state/FL
That’s a pretty shitty school district if they are failing like you say.+1
Common sense post from an educational expert. We were told directly by our school that this is not "distance learning", but rather emergency learning. Such learning is more effective in the later grades, but still not a substitute for the real thing.
No reason other than fear to keep the schools closed. Makes no sense.
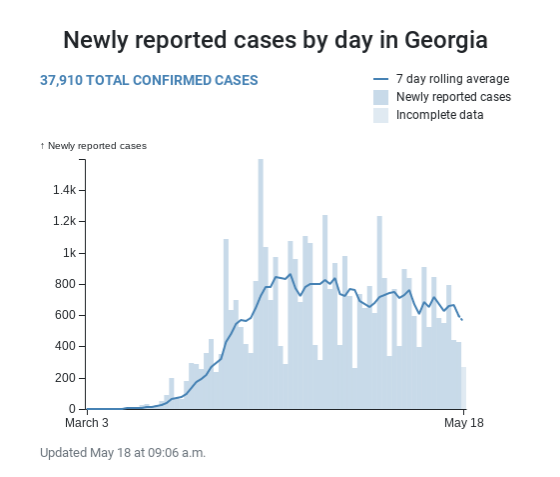
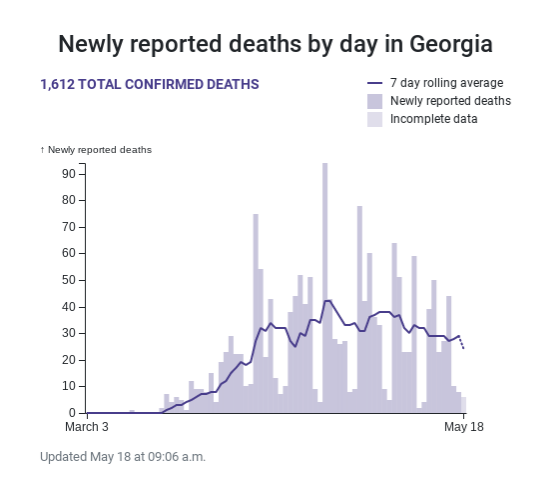
I hadn't seen the bizarre state-published chart that the AJC reported on. I've been going to https://dph.georgia.gov/covid-19-daily-status-report on a regular basis to see reported data (confirmed cases, cumulative cases, and deaths over time). The trends on that page continue to be positive. I don't know why someone thought that plotting the data on the chart the AJC criticized made any sense.You cant make this crap up...wasnt it Kemp who failed to realize CV-19 had shut states down for about a month and didnt know it could be spread by asymptomatic carriers? Then is one of the last states to shut down, one of the first to open up and his office misled people on the statistics? Bravo! This guy needs to be reelected!!!
I cannot find a way to easily grab the chart of reported cases from the daily status report but it plots the number of cases confirmed per day and the seven day running average number of cases. There is an marker at 14 days in the past because it can take up to that long for cases to be confirmed/show up, so data that is earlier than that point should be fairly stagnant.
The AJC's version of the chart is at https://www.ajc.com/news/coronavirus-georgia-covid-dashboard/jvoLBozRtBSVSNQDDAuZxH/. It also shows a slight decline in the trend of new cases. My takeaway is there's no spike of new cases evident in the data a couple of weeks into things starting to reopen. The rate of reopening appears to be picking up (anecdotal evidence only, but I've noticed more people out and about and more businesses reopening) so we will see if that trend continues or not.
Sounds like it. And it looks like the lower does is doing well too which means it will be a lot easier to scale up.
The one thing I don’t understand is how important the “neutralizing antibodies” are and if they were hoping that to be found in everyone.
Edit: The data was only available for 8 people, not that it wasn’t found in everyone. So that’s good. The article below does a better job at summarizing the results.
“The vaccine also produced neutralizing antibodies against Covid-19 in at least eight participants, the company said. Experts have said neutralizing antibodies appear to be important in acquiring protection.”
https://www.biospace.com/article/moderna-s-preliminary-phase-i-covid-19-vaccine-data-is-positive/
Neutralizing antibodies are critical to success of any vaccine (or antibody treatment); see the blog below.
Also, keep in mind that there are not any mRNA vaccines on the market that I'm aware of and that a couple of recent clinical trials with mRNA vaccines showed much less efficacy than expected and significant side effects (see the 2nd link). Doesn't mean Moderna won't be the first, but getting it right for is not going to be easy and is the reason why one of my very good friends, who knows a ton more about mRNA vaccines than I do is skeptical of the Moderna effort.
https://blogs.sciencemag.org/pipeli...-a-new-anti-coronovirus-neutralizing-antibody
https://www.nature.com/articles/nrd.2017.243
I hadn't seen the bizarre state-published chart that the AJC reported on. I've been going to https://dph.georgia.gov/covid-19-daily-status-report on a regular basis to see reported data (confirmed cases, cumulative cases, and deaths over time). The trends on that page continue to be positive. I don't know why someone thought that plotting the data on the chart the AJC criticized made any sense.
I cannot find a way to easily grab the chart of reported cases from the daily status report but it plots the number of cases confirmed per day and the seven day running average number of cases. There is an marker at 14 days in the past because it can take up to that long for cases to be confirmed/show up, so data that is earlier than that point should be fairly stagnant.
The AJC's version of the chart is at https://www.ajc.com/news/coronavirus-georgia-covid-dashboard/jvoLBozRtBSVSNQDDAuZxH/. It also shows a slight decline in the trend of new cases. My takeaway is there's no spike of new cases evident in the data a couple of weeks into things starting to reopen. The rate of reopening appears to be picking up (anecdotal evidence only, but I've noticed more people out and about and more businesses reopening) so we will see if that trend continues or not.
Update on Oxford's Jenner Institute and their weakened chimp adenovirus-based vaccine (with the CV spike protein added to it to elicit the desired antibody immune response), the paper finally came out describing their very successful vaccination trial was conducted with 6 rhesus macaques (and 3 control animals). All 6 were challenged via exposure to high levels of the coronavirus and all of them were essentially immune to the virus, producing antibodies and had no signs of respiratory infection at necropsy. Also, as of now most of the 1100 healthy volunteers have received the vaccine in the UK. Best case is phase III trial results by fall, which is ambitious. They've also partnered with AZ and others for manufacturing the vaccine at risk, in case of approval.
https://www.biorxiv.org/content/10.1101/2020.05.13.093195v1.full.pdf
https://www.marketwatch.com/story/e...-other-efforts-to-beat-coronavirus-2020-05-14
Unfortunately, some experts are now questioning the efficacy results in the macaques. It sounds like the vaccine still allowed infection, even if there was no pneumonia in the infected, vaccinated animals. This could also mean vaccinated people wouldn't be impacted by the disease, but might still be infectious. Nobody said this was going to be easy...
https://blogs.sciencemag.org/pipeli...8/criticism-of-the-oxford-coronavirus-vaccine
https://www.forbes.com/sites/willia...cine-work-in-monkeys-not-really/#43ef59d53c71
So far, so good. But both vaccinated and unvaccinated monkeys showed the same amount of viral genomic RNA from nose swab samples (Figure 3c). That’s the test that’s used out in the human population, and that means that the vaccinated animals would still be declared as positive for the coronavirus after being exposed to it. And the other thing that Haseltine notes is that the amount (the “titer”, in the lingo) of neutralizing antibodies in the blood of the vaccinated animals does not appear to be that high. You’d like to be able to dilute the blood antibody samples down by hundreds of times or even a thousandfold and still see antiviral activity in an in vitro assay, but in the Oxford case the activity started disappearing at about fortyfold dilution (Figure 2b).
On the positive side, 2/3 of the unvaccinated animals showed clear evidence of viral pneumonia at autopsy, but none of the vaccinated ones did. But on direct sampling of lung tissue. The conclusion is that the vaccinated animals were indeed infected – the vaccine did not protect against that – but that the disease was definitely less severe. But these results mean that the virus might well still be transmissible from people who had been so vaccinated, even if the disease course itself was not as deadly. You’d want to do better than that, if you can. Haseltine’s take is “Time will tell if this is the best approach. I wouldn’t bet on it.”
Its hard to say my cousin lives in a community in DelRay beach and they have not had a new case in his development in over 7 weeks and his development has about 900 homes!!Maybe the distinction is a month ago many people were visiting the ED but were not in need of being hospitalized?
Could be why the Flu ED visits were so high a month ago as well.
Edit: Ya looked into it a little, and FL(unlike NJ) does not list current hospitalizations. So I don't think we can definitely say that current Ft. Lauderdale hospitalizations have dropped. Not from that graph anyways.
Florida actually does a couple things on their dashboard which suggests they are trending downward, when that might not be accurate.
Seriously? Gotta read something to recall it.
:)
Based on this data, doesn't seem to be any legit reason for not starting back up the normal school operation.
Children are walking petri-dishes. Many first time parents of kids who just entered pre-k or kinder found this out the hard way.
You want to achieve herd immunity faster, use children as the carrier. Of course there will be many deaths. Including grandma.
Are the Georgia charts above the corrected ones with the dates in order?
- Status
- Not open for further replies.
Similar threads
- Replies
- 0
- Views
- 213
- Replies
- 14
- Views
- 636
- Replies
- 33
- Views
- 953
- Replies
- 17
- Views
- 903
- Replies
- 154
- Views
- 4K
ADVERTISEMENT
Latest posts
-
-
-
 Podcast Athan Kaliakmanis named QB1 + Gavin Wimsatt to the Portal
Podcast Athan Kaliakmanis named QB1 + Gavin Wimsatt to the Portal- Latest: Rusty_Screw_88
-

ADVERTISEMENT