Warning - very long post trying to summarize many things about COVID-19...
Seems like a lot of people are underplaying this, presumably because they simply don't fully understand the fundamental science of infectious disesases, the epidemiology of viral infections, and the risks involved in the face of high uncertainties on transmission rates and mortality rates - some similarities exist to deterministic numerical weather prediction models with there being a range of outcomes out in time that become more uncertain the further out in time one goes. However, this is not a "chaotic" system, like weather, so there are a much narrower set of outcomes possible. Here's my attempt to try to explain why this is not the flu and why the risks of inaction or poorly executed actions are far greater than for the flu or SARS/MERS.
The bottom line for everyone is that SARS-CoV2 has a significantly greater transmission rate than influenza (R-naught is 2-3 vs. about 1.3 for the flu, meaning without intervention, each infected person would be expected to infect 2-3 others for coronavirus and only 1.3 others for influenza) and has significantly greater mortality (and I'll get to this in a second) and hospitalization rates than influenza, such that if we treated it like the flu, i.e., did essentially nothing, we'd see many more deaths than the 30-60K we have each year in the US (and more hospitalizations). How effective we'll be in the US in making this less impactful than influenza is an open question.
http://www.cidrap.umn.edu/news-perspective/2020/03/study-highlights-ease-spread-covid-19-viruses
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)30567-5/fulltext?fbclid=IwAR0LaDqifJTW9mENQXL6olEkj7jkEBarsm_cYLlTXpj88rALqP9Vz5gBljo
Fortunately, we have epidemiologists and infectious disease scientists who actually know stuff, which is why every country in the world, including even the US, despite elements of our government leadership downplaying this, is taking moderate to very aggressive steps to contain the burgeoning outbreaks in order to greatly reduce transmission rates (since mortality rates are mostly constant, until and unless we get some medical treatment breakthroughs - and vaccines aren't "treatment" - they're only prevention and we won't have any until at least next winter), so that the actual outcomes aren't worse than the flu or even that close, if we do this right.
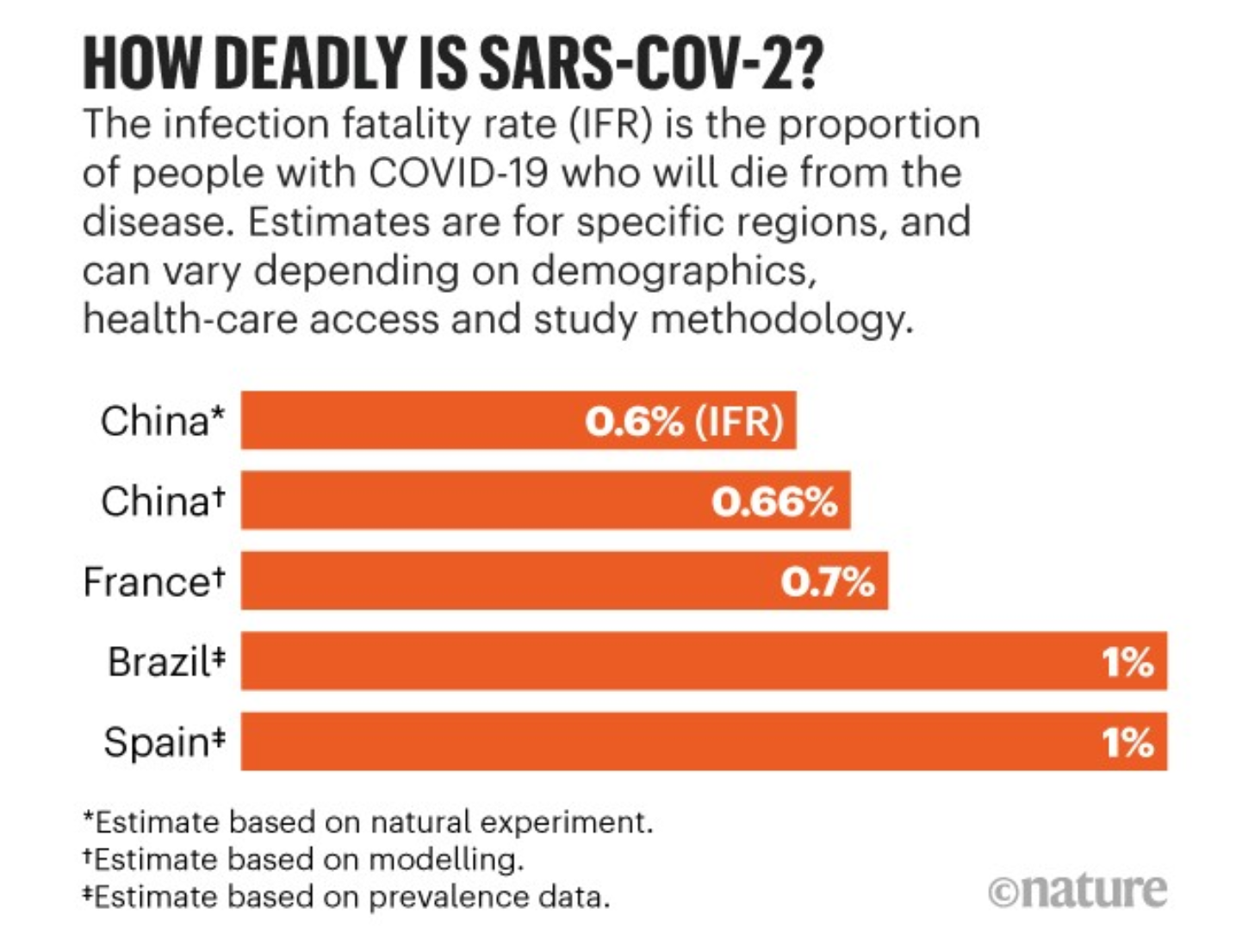
So, let's talk about mortality rates. Yes, the overall currently reported mortality rates of 2-5% are inflated, because the denominator of total infections is not well known in most countries, largely due to far from comprehensive testing. A much more likely eventual mortality rate is about 0.5-1.0%, based on the ~0.7% seen so far in South Korea, where they've tested 10X more people than anyone and close to 1000X more people (per capita) than the US. Even at 0.5% that's 2.5-5X the average overall influenza mortality rate of 0.1-0.2% (depending on severity that season) worldwide and at 1.0% that would be 5-10X the mortality rate of influenza. Those are the mutlipliers (or more we'd likely see if we did nothing at all). Also, the mortality rate on that floating coronavirus experiment, the Diamond Princess, showed an overall mortality rate of about 1% (close to the SK number and the number postulated in the link below), with all the deaths being in those over 80.
https://slate.com/technology/2020/0...wRWmsoZJ8PHkgyHu6WDNkDwVRsvZ-cdQZd-pV2OwP6PQ0
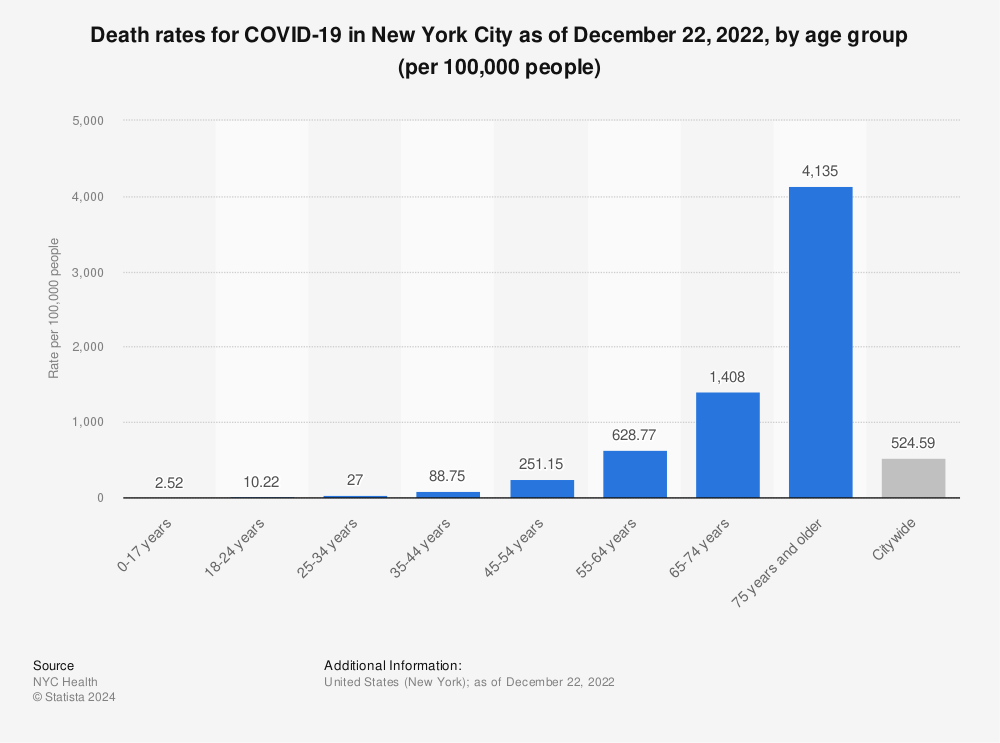
Now let's talk about age group mortality rates. The best data on that is still from China, given how large and long lasting their outbreak has been - of course these might be a bit high vs. "true" mortality rates, when compared to SK, assuming SK has close to the "true" rates, as the overall rate in China has been reported to be anywhere from 1.4-3.4% but they're at least illustrative.
Older adults have been hit the hardest. The death rate soars to 14.8% in those 80 and older; among those ages 70 to 79, the COVID-19 death rate in China seems to be about 8%, whereas it’s 3.6% for those ages 60 to 69, 1.3% for 50 to 59, 0.4% for those 40 to 49; and just 0.2% for people ages 10 to 39. No deaths in children under 9 have been reported. Even if these were cut by half or by 2/3, they're still well beyond what we see for influenza, where mortality rates in those over 65 is about 1% of those infected and is about 0.02% for those under 40, giving the overall rate of 0.1-0.2%.
https://www.livescience.com/new-coronavirus-compare-with-flu.html
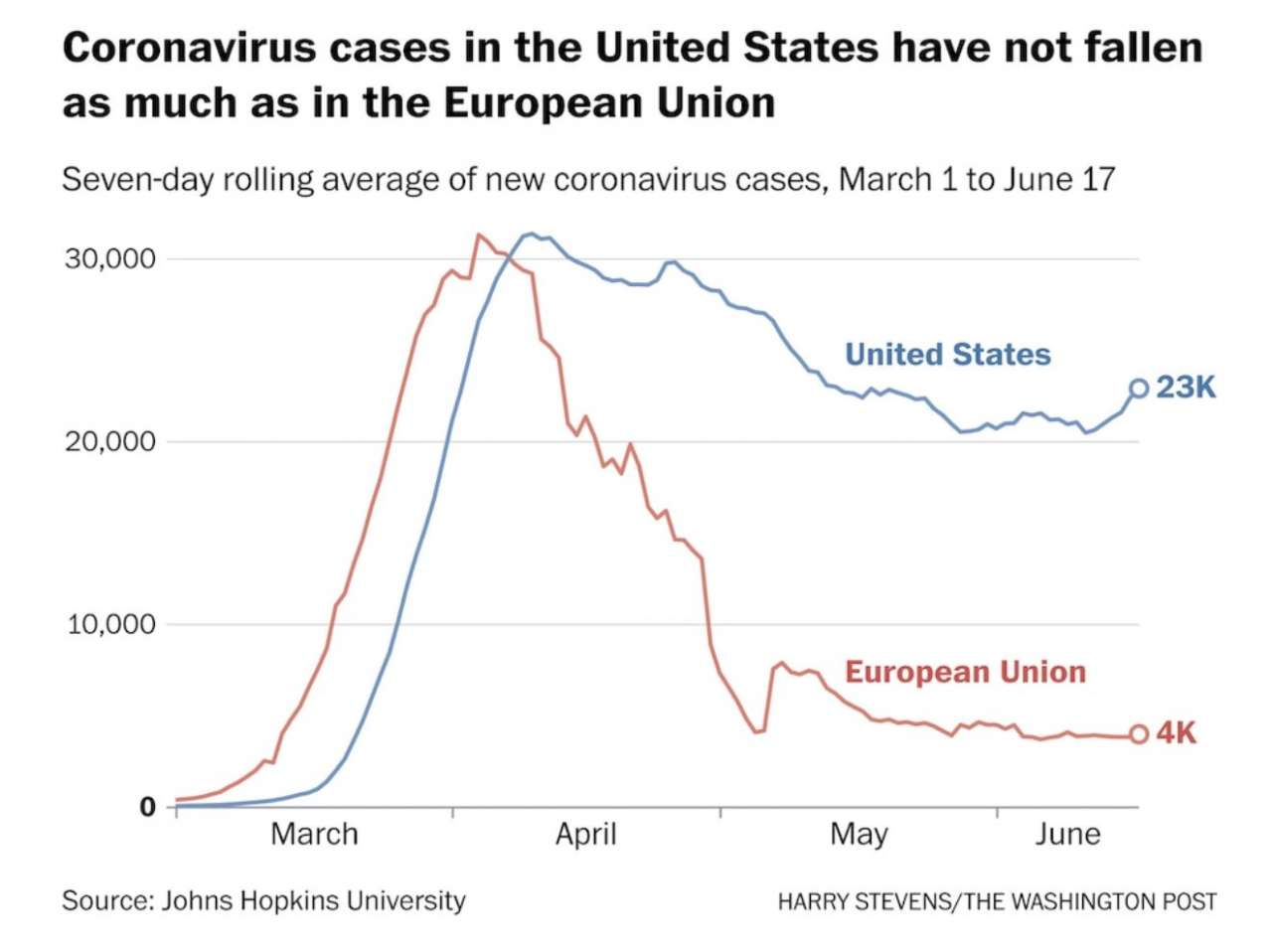
Finally, given the ongoing pandemic, what do we do about it? Well, as I've posted several times, I think the answer lies in South Korea. The most important element of their programs is that they've been testing like crazy (over 190,000 tests so far vs. about 7500 confirmed cases) and practicing effective social distancing/self-quarantining, including not allowing large crowds to gather (but not in full lockdown); in addition, finding out positive cases early on means both better treatment outcomes and self-quarantining of infected people, greatly reducing transmission rates.. They've essentially flattened the Farr's Law epidemiological curve, as per the first graphic, below, to reduce the peak "height" of max number of cases, so that health systems can keep up with infections, rather than being overwhelmed as occurred in Wuhan and is occurring in Iran and Italy - and I think is likely to occur here, at least in very densely populated areas like the DC-Boston corridor.

https://www.bloomberg.com/amp/news/...hundreds-of-thousands-to-fight-virus-outbreak
https://gisanddata.maps.arcgis.com/apps/opsdashboard/index.html#/bda7594740fd40299423467b48e9ecf6
Without such testing, as has largely been the case here, there are likely many infected, but asymptomatic or mildly symptomatic people walking around taking no precautions and infecting other people, some of whom are likely in much higher risk age/condition groups - so even though people under 40 are unlikely to be seriously impacted (although fatality rates in China were still above those of influenza, except for children), they can still have a large impact by simply being carriers, especially since the median incubation time from infection to symptoms is 5 days - hence the need for testing and social distancing.
And while SK has 7500 cases, most of that originated early on when travel from China was not restricted. However, recently, the case rate is decreasing, plus their mortality rate is much lower than anywhere else (0.7% vs. 2-5% elsewhere), partly because of early identification/treatment and partly because the denominator is likely close to the real denominator, since they're finding mildly symptomatic people others aren't - and in fact the "true" mortality rate is probably close to SK's, but that's impossible to know without a lot more testing in these other countries.
Unfortunately, the US is not taking SK's approach, having completely bungled testing, which continues, as we've tested 1000X less people, per capita than SK (see table below). It's unconscionable - this lack of testing is putting us at real risk of an Italy-style outbreak, especially in highly densely populated areas like DC to Boston, including NJ/NY, obviously. So, think about all of this when you get annoyed at that school closing or event being cancelled or having to work from home. Hopefully we'll start to see a lot more proactive efforts here at home soon, because if we don't it's going to get ugly fast.
https://www.businessinsider.com/coronavirus-testing-covid-19-tests-per-capita-chart-us-behind-2020-3
https://www.sciencenews.org/article/coronavirus-testing-diagnostic-covid19-united-states
Once again, this is not influenza - it's much more dangerous, even if the outcomes, worldwide, end up showing far less deaths than influenza, due to countries realizing the risks and implementing interventions to reduce transmission rates, since "true" mortality rates should be a constant. Kind of like Y2K, where billions were spent to prevent a potential catastrophe and then when the catastrophe didn't occur because of those efforts, many people said we wasted our efforts.
As an aside, I've never worried about any infections before, but I'm worried about this one - we've been in near lockdown for the past 8 days (some asthma and other issues). I'm not worried much about me, but I also don't want to go out and catch the virus and infect my wife and son or anyone else, really) and we have about a month's worth of non-perishable food.
One more thing. We also don't know yet if this will be seasonal, like the flu and die down in spring - one would think it should be, given virus sensitivity to heat/UV and increased humidity reducing transmission rates (more effective mucus and less "travel"/resuspension in air of viruses when it's humid) and less people being confined from the cold. However, SARS petered out before spring and MERS started in September in Saudi Arabia, so we don't know the seasonal behavior of those coronaviruses. In addition, it's becoming more likely that this virus will be around for awhile.
https://www.marketwatch.com/story/why-this-epidemiologist-is-more-worried-about-coronavirus-than-he-was-a-month-ago-2020-03-09
Ok last thing: I'd love to know what's going on in Germany. 1565 cases and only 2 deaths (0.1-0.2% mortality rate). Data problem, weird outlier, lack of reporting?
3/11 Edit: Not surprisingly, many experts are giving credit to Germany's aggressive testing approach (see link), which is not surprising since the Germans were the ones who developed the WHO-approved test in late January that much of the world uses (but not the US). Also, it should be noted that Germany is the oldest country in Europe (older even than Italy), so high fatality rates, like Italy has seen (6%) are not necessarily a given, due to an aging population. Having said that, though, it's still too early in the evolution of this situation to declare "victory" in Germany, but it's definitely worth paying attention to.
https://www.nytimes.com/aponline/2020/03/09/world/europe/ap-eu-virus-outbreak-germany.html