
You offer just one view, which you've repeated every day, multiple times a day, for months on end. So you can stop now. It's very tiresome.I am saying ask questions. I am stop believing everything Msm tells you. I am saying lots of different options exist and lots of different views on this exist
Colleges
- American Athletic
- Atlantic Coast
- Big 12
- Big East
- Big Ten
- Colonial
- Conference USA
- Independents (FBS)
- Junior College
- Mountain West
- Northeast
- Pac-12
- Patriot League
- Pioneer League
- Southeastern
- Sun Belt
- Army
- Charlotte
- East Carolina
- Florida Atlantic
- Memphis
- Navy
- North Texas
- Rice
- South Florida
- Temple
- Tulane
- Tulsa
- UAB
- UTSA
- Boston College
- California
- Clemson
- Duke
- Florida State
- Georgia Tech
- Louisville
- Miami (FL)
- North Carolina
- North Carolina State
- Pittsburgh
- Southern Methodist
- Stanford
- Syracuse
- Virginia
- Virginia Tech
- Wake Forest
- Arizona
- Arizona State
- Baylor
- Brigham Young
- Cincinnati
- Colorado
- Houston
- Iowa State
- Kansas
- Kansas State
- Oklahoma State
- TCU
- Texas Tech
- UCF
- Utah
- West Virginia
- Illinois
- Indiana
- Iowa
- Maryland
- Michigan
- Michigan State
- Minnesota
- Nebraska
- Northwestern
- Ohio State
- Oregon
- Penn State
- Purdue
- Rutgers
- UCLA
- USC
- Washington
- Wisconsin
High Schools
- Illinois HS Sports
- Indiana HS Sports
- Iowa HS Sports
- Kansas HS Sports
- Michigan HS Sports
- Minnesota HS Sports
- Missouri HS Sports
- Nebraska HS Sports
- Oklahoma HS Sports
- Texas HS Hoops
- Texas HS Sports
- Wisconsin HS Sports
- Cincinnati HS Sports
- Delaware
- Maryland HS Sports
- New Jersey HS Hoops
- New Jersey HS Sports
- NYC HS Hoops
- Ohio HS Sports
- Pennsylvania HS Sports
- Virginia HS Sports
- West Virginia HS Sports
ADVERTISEMENT
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
COVID-19 Pandemic: Transmissions, Deaths, Treatments, Vaccines, Interventions and More...
- Thread starter Richie O
- Start date
- Status
- Not open for further replies.

Current total patients in all three USC hospitals with Covid?
8.
8.
Oh! So Newsom's interventions worked? Awesome.Current total patients in all three USC hospitals with Covid?
8.
Are you guys going to bring this up once a week? Sweden has the 6th highest per capita death rate in the world (ignoring the tiny countries of Andorra and San Marino) and has 10X or more deaths per capita than its similarly situated (wrt/density and culture) Nordic neighbors Norway and Finland. Quite a success story. Yes, infections/deaths are way down, but they're way down in most of Europe now.
What's wrong with looking at what other countries did and what the results were so we can learn from them?
I'm assuming you read the article. What do you think about what the doctor says about T-cells? do you think that's a possible explanation for why people in Sweden aren't getting it anymore?
What's wrong with looking at what other countries did and what the results were so we can learn from them?
I'm assuming you read the article. What do you think about what the doctor says about T-cells? do you think that's a possible explanation for why people in Sweden aren't getting it anymore?
Nothing is wrong with it, but we’ve literally had this discussion 500 times.
Interesting. So what would be Sweden's working age (e.g.18-65) and student per capita chicomvirus death rates (without the economy lockdowns!)? Around 250-300/1MM?Add Sweden to that list too.
Last edited:
What you are saying makes no sense. Who is not asking questions? Who believes everything that is told to them? I am more of a republican than democrat. I voted for Trump. I am a republican around fiscal issues and Democrat around social issues. I question everything. The plan right now that we are doing in NJ is very sensible from what I see. I don’t agree with the number of people limits at indoor and outdoor gatherings. That to me is dumb as people have different sized yards and houses. I am not saying every call has been perfect at all but indoor restaurant eating should be banned for now. Masks should be worn at all indoor stores and outdoors where you can’t socially distant masks should be worn. That’s it. What do you disagree with there? Even if masks aren’t perfect they have been proven to reduce the risk.
Why are there are almost no cases in Sweden and Denmark without masks
Nope. There was never any need for them. It’s all a lie.Oh! So Newsom's interventions worked? Awesome.
because masks cause the virus to spread, and also breathing in your own co2 isn't healthy. It is known that mask wearing plus demon sperm dreams lowers immunity.Why are there are almost no cases in Sweden and Denmark without masks
Geez "Greg", you have some weird thoughts.because masks cause the virus to spread, and also breathing in your own co2 isn't healthy. It is known that mask wearing plus demon sperm dreams lowers immunity.
What's wrong with looking at what other countries did and what the results were so we can learn from them?
I'm assuming you read the article. What do you think about what the doctor says about T-cells? do you think that's a possible explanation for why people in Sweden aren't getting it anymore?
Nothing wrong with it - I just wish people would make relevant comparisons and the most relevant comparison is Sweden to Norway/Finland (similar population densities/cultures) and Sweden has done far, far worse, so holding Sweden up as some success story seems quite inappropriate to me. The fact that Sweden has a similar per capita death rate as ~5-10X more densely populated countries, like Italy, UK, France, Spain, etc., is another sign of how badly they did.
I was the first person on this board to bring up the intriguing possibility of T-cell cross-reactivity from prior exposure to other coronaviruses conferring some or even significant immunity to people who had never been exposed to SARS-CoV-2, so yeah, I know a little about it. The problem is scientists simply don't know if this cross-reactivity provides immunity or not for small or large numbers of people and are unlikely to ever know, since assessment of COVID infections for people with and without such T-cells, in large numbers would be the only way to know and I don't think there's any way that can be done with extremely-difficult-to-measure T-cells (but it would be a great study to do).
Also, given Sweden's/Stockholm's much lower level of people with antibodies (~6%/10% respectively, as per below), reflecting past COVID infection, vs. areas like NY/NYCMetro (13.4%/21.6%, respectively, with the Bronx up to 32%), London, Northern Italy, etc., I'd say it's highly unlikely that, even if there is some 20-40% magic cap on those infected due to cross-reactivity, Sweden would still be quite far from that, as opposed to NYC. And the fact that both (with close to 10MM people each) have in the range of 200-400 cases per day on a 7-day moving average tells me that their interventions are working (distancing in Sweden and masks/distancing in NYC with a far higher density), but that the virus is nowhere near under control.
I'm praying for cross-reactivity to be real and to equate to some cap on how many can become infected, which could lead to herd immunity levels being much lower than currently thought (55-80% range), but in the absence of compelling data to that effect, I think our focus should be on: a) reducing transmissions, cases, hospitalizations and deaths by masking/distancing with testing/tracing/isolating to prevent small flare-ups from becoming major outbreaks and b) continuing our extraordinary scientific efforts to find working treatments/cures and on developing and distributing vaccines (also vaccines should improve everyone's immunity, even those with cross-reactive T-cells).
Being cagey again? Direct is better, IMO. If you want to argue about "dark matter" and the potential that there's some hidden 20% cap to infections, have at it. But the fact that neighborhoods in NYC and Italy had 50-65% with antibodies and there have been smaller closed populations (prisons, meatpacking plants, etc.) with up to 80% infected, as measured by the viral PCR test, makes that 20% cap seem unlikely. If you want to argue the potential immunity in unexposed people due to T-cell cross-reactivity, that's a much more scientific possibility, but nobody knows yet if that response to COVID in cell cultures of people never exposed to COVID means they have little, some or complete immunity.
Anyway, that test of 50K people was done by a private company and was not randomly drawn from the population, so it was likely not representative of the country's population. In addition, the 14% result was for Stockholm, not for the country, which would be much lower, given the much lower density of the remaining 75% of Sweden's population and lower transmission rates outside of Stockholm.
https://www.thelocal.se/20200618/one-in-seven-stockholmers-had-coronavirus-antibody-in-private-tests
Better data on antibody levels in Sweden are from the blood donor studies, which are more representative than the private tests where people are motivated to get a result because they suspect infection. As of the end of May, 6.3% of Sweden was found to have antibodies and given the low infection rates since then, it's unlikely that more than 7-8% have been infected as of now.
Analysis of samples collected at Week 21 shows that antibodies to covid-19 are detected in 6.3 percent of the studied population. Antibodies continue to be lowest among older adults 65-95 years with 3.9 percent and higher among adults 20-64 years with 7.6 percent and among children 0-19 years with 7.5 percent.
Data at the regional level is presented only for Stockholm, Västra Götaland and Skåne as the number of samples collected for the other regions is less than 100 and therefore cannot give reliable results. In the Stockholm region, Week 21 had the highest proportion of antibody positives with 10.0 percent, followed by Skåne with 4.5 percent and Västra Götaland with 2.7 percent.
http://outbreaknewstoday.com/sweden...fection-antibody-tests-in-blood-donors-98648/
Edit: added link to NY/NYC antibody data...
https://www.6sqft.com/new-york-covid-antibody-test-preliminary-results/
This metric is highly variable depending on how stringent "no symptoms" means. All people have daily or weekly little things.....headache, sore throat, small cough due to numerous reasons, etc. Does this daily background noise count as a "symptom" or not? Change this a little bit and this metric would be very different.
The doctor did say he was speaking anecdotally and while those of us not trained as science or medical professionals look to that I believe those trained in those professions want more than anecdotal reports.What's wrong with looking at what other countries did and what the results were so we can learn from them?
I'm assuming you read the article. What do you think about what the doctor says about T-cells? do you think that's a possible explanation for why people in Sweden aren't getting it anymore?
I also think there were some interesting comments. 2 towards the end wish he had a response to.
I also wonder if a country of 350 million countries have handled this the same way as a country of 10 million
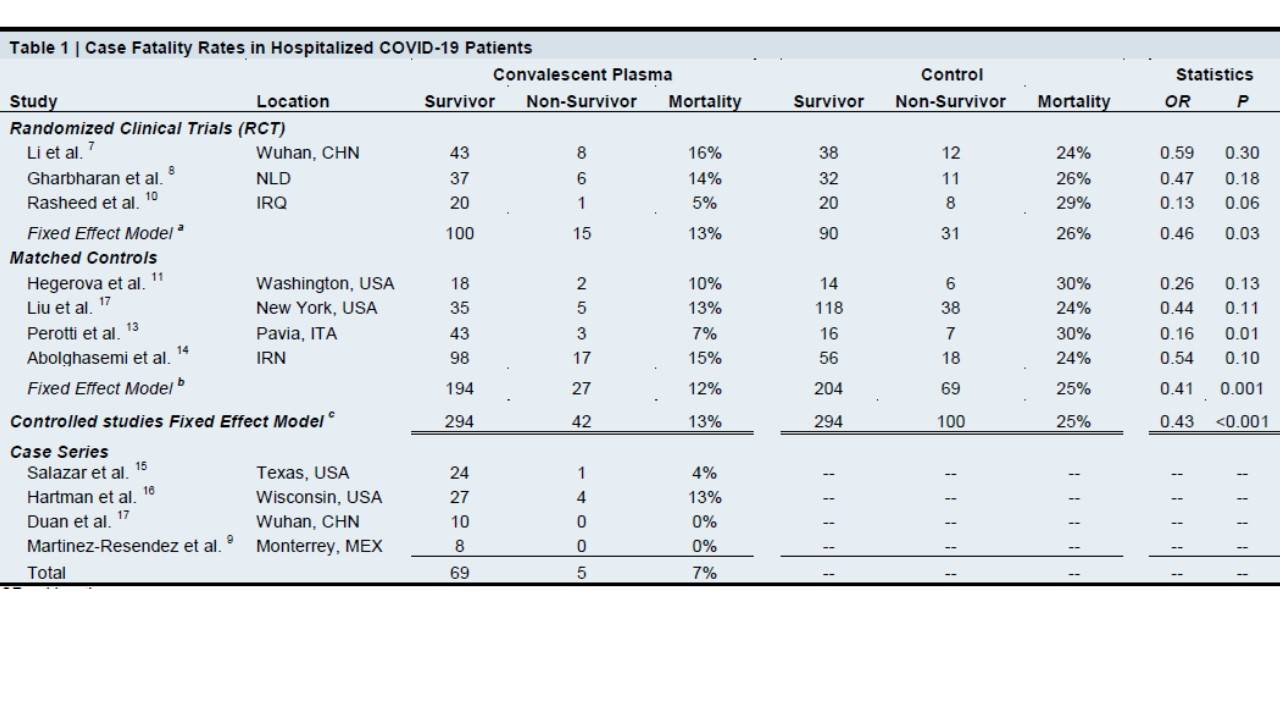
As most here know, I've been very hopeful (since March!) that convalescent plasma from COVID survivors, containing protective antibodies to the virus would be an effective treatment for COVID patients. Well, we don't quite have ironclad results from a formal randomized, controlled, blinded clinical trial, but today we got a preprint from the leaders of the CP expanded access program (overseen by the Mayo Clinic, with over 50,000 patients infused so far) featuring a meta-analysis aggregating results from all controlled trials to date and the results are very encouraging, with a highly statistically significant mortality reduction of 57%.
https://www.medrxiv.org/…/10…/2020.07.29.20162917v1.full.pdf
We've heard countless anecodotes of success and many of these individual studies showed mortality reduction, but weren't statistically powered well enough (not enough patients) to be considered statistical "proof" of efficacy. By aggregating the studies and controlling for patient variables as well as possible, there was enough statistical strength for the authors to feel that there is now very strong evidence of morality reduction at a p-value of <0.001 (normally "statistically significant" is indicated by a p-value of <0.05, translating to 95% probability that the treatment outcome is valid - it's more complicated than that, but not worth repeating here, IMO).
These results also bode well for the effectiveness of engineered antibodies, which should be more consistent and highly targeted than CP (plasma is very variable based on the patient); these should be done with phase III trials by the end of August. I'm also much more confident, now, that use of plasma is one of the key reasons fatality rates have dropped significantly in this 2nd wave, as 50,000 patients infused is a decent percentage of those that have been pretty ill - would be nice to see more data on that to prove or disprove that thinking. I'm still a bit disappointed they didn't just do a randomized/controlled right away back in April, so we'd have even better data, but that's water under the bridge now.
The present analyses included a total of twelve studies including three RCTs, five matchedcontrol studies, and four case series studies containing 804 COVID-19 patient outcomes from around the world (Table 1). The mean or median age of patients enrolled in these studies ranged from 48 to 70 years, with a greater proportion of men than women in most studies (proportion of women: 25% to 56%). All studies included patients with severe or life-threatening COVID-19. At the time of plasma transfusion, the proportion of patients on mechanical ventilation varied by study from 0% to 81%. The duration of follow up ranged from 7 to 30 days. All case-series studies demonstrated relatively low mortality rates for COVID-19 patients transfused with convalescent plasma (0% to 13%). Among RCTs, patients transfused with convalescent plasma exhibited a reduced mortality rate (13%) compared to non-transfused COVID-19 patients (26%; OR: 0.46, P = 0.03). Among matched control studies, patients transfused with convalescent plasma exhibited a reduced mortality rate (12%) compared to nontransfused COVID-19 patients (25%; OR: 0.41, P = 0.001). When patient outcomes from controlled studies were aggregated, patients transfused with convalescent plasma exhibited a reduced mortality rate (13%) compared to non-transfused COVID-19 patients (25%; OR: 0.43, P < 0.001). Meta-regression analysis indicated that mean or median cohort age, proportion of cohort receiving mechanical ventilation, and duration of study follow up did not affect the aggregate OR computed for all controlled studies (all coefficients P > 0.22). The fixed effect OR (OR: 0.44, P<0.001) was not different when outlier mortality rates from the matched control study by Xia and colleagues were included in analyses (case mortality rate: 2%, control mortality rate: 4%).
Excellent article from a few days ago in the Times, discussing convalescent plasma in more detail. While the 57% mortality reduction calculated from pooling various smaller studies, above, is great, it's still not a single randomized controlled trial (RCT) showing that, so there will always be nagging doubts on its effectiveness until we have such data.
This article at least dives in and explains some reasons why we don't have such data yet, with two key issues emerging: doctors/patients being unwilling to forego plasma vs. possibly getting a placebo (or standard care, which hasn't been that great) as part of a trial, plus outbreaks being greatly reduced in areas where some RCTs were underway. At this point, there are researchers now sending plasma to places like Brazil to try to complete their trials.
In many ways the success of the expanded access program (over 80,000 now have been treated with CP and 1500 patients per day are now being treated across the US) has killed the ability to do these RCTs. In hindsight, it probably would've been better to simply start with an RCT to eliminate any doubts. Assuming the 57% mortality reductions are real, at 1500 patients per day, this would likely be part of the significant reduction in deaths per cases we're seeing in this 2nd wave.
There are parallels to HCQ here, also, where it would've been better to do an RCT before giving the drug to hundreds of thousands of patients without any indication of efficacy. At least CP has a history of being safe and effective in previous viral diseases and has absolutely been shown to be safe in COVID patients. Given its past history and very promising data to date, though, it's clear that the medical community, including our top goverment medical leaders are very supportive of expanding CP use further, as per comments by Drs Birx and Hahn in the article.
https://www.nytimes.com/2020/08/04/health/trump-plasma.html
But the unexpected demand for plasma has inadvertently undercut the research that could prove that it works. The only way to get convincing evidence is with a clinical trial that compares outcomes for patients who are randomly assigned to get the treatment with those who are given a placebo. Many patients and their doctors — knowing they could get the treatment under the government program — have been unwilling to join clinical trials that might provide them with a placebo instead of the plasma.
The trials have also been stymied by the waning of the virus outbreak in many cities, complicating researchers’ ability to recruit sick people. One of those clinical trials, at Columbia University, sputtered to a halt after the outbreak subsided in New York. One of its leaders, Dr. W. Ian Lipkin, looked for hospitals in other hot spots in the United States to continue the work. But he found few takers.
Edit: found my old post with a link to a comment from one of the leads on the plasma program and the quote in the article from 3/25 said, I'd like to know how we missed getting these data early on, before the very promising plasma results started coming in and before we ran out of patients in NYC.
In one of three proposed US trials, Liise-anne Pirofski, an infectious-disease specialist at Albert Einstein College of Medicine, says researchers plan to infuse patients at an early stage of the disease and see how often they advance to critical care. Another trial would enroll severe cases. The third would explore plasma’s use as a preventative measure for people in close contact with those confirmed to have COVID-19, and would evaluate how often such people fall ill after an infusion compared with others who were similarly exposed but not treated. These outcomes are measurable within a month, she says. “Efficacy data could be obtained very, very quickly.”
https://rutgers.forums.rivals.com/t...ventions-and-more.191275/page-34#post-4470810
Last edited:
The doctor did say he was speaking anecdotally and while those of us not trained as science or medical professionals look to that I believe those trained in those professions want more than anecdotal reports.
I also think there were some interesting comments. 2 towards the end wish he had a response to.
I also wonder if a country of 350 million countries have handled this the same way as a country of 10 million
Its important to ask questions
Its also important to ask what the end games is...how many cases til we go to normal activities
Doesnt seem to be alot of discussion about if we do A than B can happen. Who gets to decide...certainly not the public
Interesting stuff, thanks for posting!
Interesting stuff, thanks for posting!
Just make sure you actually read the article, because that’s not what he says at all. Tweet titles like that are moronic.
Nothing is wrong with it, but we’ve literally had this discussion 500 times.
Yes, but things keep on changing. There's still a lot we don't know about the virus. Why can't we continue to collect data and make observations from all over the world. What's wrong with that?
Always ask questions both when you agree or disagree with the point of viewIts important to ask questions
Its also important to ask what the end games is...how many cases til we go to normal activities
Doesnt seem to be alot of discussion about if we do A than B can happen. Who gets to decide...certainly not the public
Always ask questions both when you agree or disagree with the point of view
except the msm isnt asking questions..in fact the general push here has been fall in line or you are some kind of red state Karen, albeit protests are encouraged because Corona knows to stay away
Its important to ask questions
Its also important to ask what the end games is...how many cases til we go to normal activities
Doesnt seem to be alot of discussion about if we do A than B can happen. Who gets to decide...certainly not the public
As to who makes the decision it is elected officials and then the public has the final day on Election Day
Nothing wrong with it - I just wish people would make relevant comparisons and the most relevant comparison is Sweden to Norway/Finland (similar population densities/cultures) and Sweden has done far, far worse, so holding Sweden up as some success story seems quite inappropriate to me. The fact that Sweden has a similar per capita death rate as ~5-10X more densely populated countries, like Italy, UK, France, Spain, etc., is another sign of how badly they did.
I was the first person on this board to bring up the intriguing possibility of T-cell cross-reactivity from prior exposure to other coronaviruses conferring some or even significant immunity to people who had never been exposed to SARS-CoV-2, so yeah, I know a little about it. The problem is scientists simply don't know if this cross-reactivity provides immunity or not for small or large numbers of people and are unlikely to ever know, since assessment of COVID infections for people with and without such T-cells, in large numbers would be the only way to know and I don't think there's any way that can be done with extremely-difficult-to-measure T-cells (but it would be a great study to do).
Also, given Sweden's/Stockholm's much lower level of people with antibodies (~6%/10% respectively, as per below), reflecting past COVID infection, vs. areas like NY/NYCMetro (13.4%/21.6%, respectively, with the Bronx up to 32%), London, Northern Italy, etc., I'd say it's highly unlikely that, even if there is some 20-40% magic cap on those infected due to cross-reactivity, Sweden would still be quite far from that, as opposed to NYC. And the fact that both (with close to 10MM people each) have in the range of 200-400 cases per day on a 7-day moving average tells me that their interventions are working (distancing in Sweden and masks/distancing in NYC with a far higher density), but that the virus is nowhere near under control.
I'm praying for cross-reactivity to be real and to equate to some cap on how many can become infected, which could lead to herd immunity levels being much lower than currently thought (55-80% range), but in the absence of compelling data to that effect, I think our focus should be on: a) reducing transmissions, cases, hospitalizations and deaths by masking/distancing with testing/tracing/isolating to prevent small flare-ups from becoming major outbreaks and b) continuing our extraordinary scientific efforts to find working treatments/cures and on developing and distributing vaccines (also vaccines should improve everyone's immunity, even those with cross-reactive T-cells).
I'm with you, I'm praying for cross-reactivity as well. Well, not actually praying. I'm an atheist. Let's just say I'm hoping. Too bad we'll never know for sure. Like you said, it's extremely difficult to measure T cells. I never knew that before. Thanks for the information.
ahem
https://www.cnbc.com/2020/08/07/cor...f-it-being-highly-effective-is-not-great.html
reality
https://www.cnbc.com/2020/08/07/cor...f-it-being-highly-effective-is-not-great.html
reality
- White House coronavirus advisor Dr. Anthony Fauci that the chances of scientists creating a highly effective vaccine — one that provides 98% or more guaranteed protection — for the virus are slim.
- Scientists are hoping for a coronavirus vaccine that is at least 75% effective, but 50% or 60% effective would be acceptable, too, he said.
- The FDA has said it would authorize a coronavirus vaccine so long as it is safe and at least 50% effective.
I don’t watch much MSM. I read a lot from the internet and I do speak to people in the medical community. I would never base my opinion on the likes of Joy Reid or Sean Hannityexcept the msm isnt asking questions..in fact the general push here has been fall in line or you are some kind of red state Karen, albeit protests are encouraged because Corona knows to stay away
The doctor did say he was speaking anecdotally and while those of us not trained as science or medical professionals look to that I believe those trained in those professions want more than anecdotal reports.
I also think there were some interesting comments. 2 towards the end wish he had a response to.
I also wonder if a country of 350 million countries have handled this the same way as a country of 10 million
I wonder as well, but I just found the article interesting. I'm not saying we should have done exactly what Sweden has done, but it is interesting that they now seem to be done with it.
I think it was a difficult decision either wayI wonder as well, but I just found the article interesting. I'm not saying we should have done exactly what Sweden has done, but it is interesting that they now seem to be done with it.
Yes, but things keep on changing. There's still a lot we don't know about the virus. Why can't we continue to collect data and make observations from all over the world. What's wrong with that?
That’s what this thread is for. There’s just nothing new with the Sweden discussion. Maybe I forget people don’t read every page, but there’s pages and pages on this topic.
How would you know? Can't prove a negative.Nope. There was never any need for them. It’s all a lie.
Your contribution to this thread has been nothing short of uncontrollable verbal diarrhea.
I'm an atheist also, which many know, so me "praying" means I really, really hope it happens, lol...I'm with you, I'm praying for cross-reactivity as well. Well, not actually praying. I'm an atheist. Let's just say I'm hoping. Too bad we'll never know for sure. Like you said, it's extremely difficult to measure T cells. I never knew that before. Thanks for the information.
Stop complimenting him...How would you know? Can't prove a negative.
Your contribution to this thread has been nothing short of uncontrollable verbal diarrhea.
I don’t watch much MSM. I read a lot from the internet and I do speak to people in the medical community. I would never base my opinion on the likes of Joy Reid or Sean Hannity
i dont watch them either for news
That’s what this thread is for. There’s just nothing new with the Sweden discussion. Maybe I forget people don’t read every page, but there’s pages and pages on this topic.
there is a post from a Swedish doctor on the front lines and that is much more than you have ever contributed
Nothing wrong with it - I just wish people would make relevant comparisons and the most relevant comparison is Sweden to Norway/Finland (similar population densities/cultures) and Sweden has done far, far worse, so holding Sweden up as some success story seems quite inappropriate to me. The fact that Sweden has a similar per capita death rate as ~5-10X more densely populated countries, like Italy, UK, France, Spain, etc., is another sign of how badly they did.
I was the first person on this board to bring up the intriguing possibility of T-cell cross-reactivity from prior exposure to other coronaviruses conferring some or even significant immunity to people who had never been exposed to SARS-CoV-2, so yeah, I know a little about it. The problem is scientists simply don't know if this cross-reactivity provides immunity or not for small or large numbers of people and are unlikely to ever know, since assessment of COVID infections for people with and without such T-cells, in large numbers would be the only way to know and I don't think there's any way that can be done with extremely-difficult-to-measure T-cells (but it would be a great study to do).
Also, given Sweden's/Stockholm's much lower level of people with antibodies (~6%/10% respectively, as per below), reflecting past COVID infection, vs. areas like NY/NYCMetro (13.4%/21.6%, respectively, with the Bronx up to 32%), London, Northern Italy, etc., I'd say it's highly unlikely that, even if there is some 20-40% magic cap on those infected due to cross-reactivity, Sweden would still be quite far from that, as opposed to NYC. And the fact that both (with close to 10MM people each) have in the range of 200-400 cases per day on a 7-day moving average tells me that their interventions are working (distancing in Sweden and masks/distancing in NYC with a far higher density), but that the virus is nowhere near under control.
I'm praying for cross-reactivity to be real and to equate to some cap on how many can become infected, which could lead to herd immunity levels being much lower than currently thought (55-80% range), but in the absence of compelling data to that effect, I think our focus should be on: a) reducing transmissions, cases, hospitalizations and deaths by masking/distancing with testing/tracing/isolating to prevent small flare-ups from becoming major outbreaks and b) continuing our extraordinary scientific efforts to find working treatments/cures and on developing and distributing vaccines (also vaccines should improve everyone's immunity, even those with cross-reactive T-cells).
Pretty good article today about the T Cell topic. I personally think a good chunk (~20%) of the general population has has immunity via other Coronavirus’. Which means in places like NYC, herd immunity may not be that far off.
https://www.washingtonpost.com/health/2020/08/08/asymptomatic-coronavirus-covid/
That’s what this thread is for. There’s just nothing new with the Sweden discussion. Maybe I forget people don’t read every page, but there’s pages and pages on this topic.
Actually, there is something new. The fact they are down to one death a day and some days without any deaths for a week. There's also very few new cases. There's no reason to not tract this. It's information and it's valuable. If all of a sudden, they experience a severe spike in deaths, I would post that as well. As of now, that it is not the case, but we should monitor them and everyone else's progress, look at what actions they took, and learn from them.
An excellent letter of concern written by a statistics PhD explains that if the recent hydroxychloroquine randomized trials had recruited cohorts as large as the hyped dexamethasone RECOVERY study, they would have exceeded dexa's statistical significance.
BTW, they are saying the same thing I shared with Boulware's colleague on their study. Their conclusion was wrong in that HCQ did show a positive effect as a PEP, especially when given in the first two days, but they lacked the numbers to statistically reject the null hypothesis. That is not the same thing as it does not have an effect.
BTW, they are saying the same thing I shared with Boulware's colleague on their study. Their conclusion was wrong in that HCQ did show a positive effect as a PEP, especially when given in the first two days, but they lacked the numbers to statistically reject the null hypothesis. That is not the same thing as it does not have an effect.
lmao I'd rather read his posts than the negatives you bring to the thread. Sweden sucked. Their death rates are horrible and their economy still got walloped. Facts matter.there is a post from a Swedish doctor on the front lines and that is much more than you have ever contributed
they have similar deaths a day to NJ now. Only difference is they are far less densely populated, younger, healthier, and live alone, and their economy is in the tank and most people there are still distancing.Actually, there is something new. The fact they are down to one death a day and some days without any deaths for a week. There's also very few new cases. There's no reason to not tract this. It's information and it's valuable. If all of a sudden, they experience a severe spike in deaths, I would post that as well. As of now, that it is not the case, but we should monitor them and everyone else's progress, look at what actions they took, and learn from them.
- Status
- Not open for further replies.
Similar threads
- Replies
- 47
- Views
- 3K
- Replies
- 472
- Views
- 19K
- Replies
- 136
- Views
- 5K
- Replies
- 90
- Views
- 3K
- Replies
- 25
- Views
- 2K
ADVERTISEMENT
ADVERTISEMENT