
Colleges
- American Athletic
- Atlantic Coast
- Big 12
- Big East
- Big Ten
- Colonial
- Conference USA
- Independents (FBS)
- Junior College
- Mountain West
- Northeast
- Pac-12
- Patriot League
- Pioneer League
- Southeastern
- Sun Belt
- Army
- Charlotte
- East Carolina
- Florida Atlantic
- Memphis
- Navy
- North Texas
- Rice
- South Florida
- Temple
- Tulane
- Tulsa
- UAB
- UTSA
- Boston College
- California
- Clemson
- Duke
- Florida State
- Georgia Tech
- Louisville
- Miami (FL)
- North Carolina
- North Carolina State
- Pittsburgh
- Southern Methodist
- Stanford
- Syracuse
- Virginia
- Virginia Tech
- Wake Forest
- Arizona
- Arizona State
- Baylor
- Brigham Young
- Cincinnati
- Colorado
- Houston
- Iowa State
- Kansas
- Kansas State
- Oklahoma State
- TCU
- Texas Tech
- UCF
- Utah
- West Virginia
- Illinois
- Indiana
- Iowa
- Maryland
- Michigan
- Michigan State
- Minnesota
- Nebraska
- Northwestern
- Ohio State
- Oregon
- Penn State
- Purdue
- Rutgers
- UCLA
- USC
- Washington
- Wisconsin
High Schools
- Illinois HS Sports
- Indiana HS Sports
- Iowa HS Sports
- Kansas HS Sports
- Michigan HS Sports
- Minnesota HS Sports
- Missouri HS Sports
- Nebraska HS Sports
- Oklahoma HS Sports
- Texas HS Hoops
- Texas HS Sports
- Wisconsin HS Sports
- Cincinnati HS Sports
- Delaware
- Maryland HS Sports
- New Jersey HS Hoops
- New Jersey HS Sports
- NYC HS Hoops
- Ohio HS Sports
- Pennsylvania HS Sports
- Virginia HS Sports
- West Virginia HS Sports
ADVERTISEMENT
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
COVID-19 Pandemic: Transmissions, Deaths, Treatments, Vaccines, Interventions and More...
- Thread starter Richie O
- Start date
- Status
- Not open for further replies.

"EVIDENCE IS STRONGER THAN FOR ANYTHING I"VE EVER STUDIED"
Renowned epidemiologist sees 'massive disinformation campaign' against hydroxychloroquine
Renowned epidemiologist sees 'massive disinformation campaign' against hydroxychloroquine
Has the World hit its peak of COVID transmission ?? Worldwide COVID cases are finally showing an overall downward trend for the first time since it joined the human population! The Worldometer data shows that after a mostly uninterrupted rise, the worldwide 7 day moving average leveled off from Aug 2 to Aug 13 and hovered in and around 260K new cases a day ...and peaked on Aug 13. Now, the last 10 days have seen daily decreases and it appears to be trending downward for the first time. Now down to 247K per day. Finally looking like worldwide it has finally hit its peak. Hope it continues in this direction and we can all get back to our normal lives soon !!
https://www.worldometers.info/coronavirus/#countries
https://www.worldometers.info/coronavirus/#countries
Great post and agree with everything you've said. Having been under the tent to a degree with the FDA on this since March, it was clear that they were trying to get as many shots on goal as possible and fast tracking everything. I sensed a panic on the calls but also an all-hands type of response that was pretty inspiring to be honest. I have seen the Mayo data and also enough anecdotal cases to feel the same way. If I was admitted and tested postive, I would ask for a CCP transfusion immediately.
Interesting perspective - can you share what your role has been on this? Maybe I missed it, but don't recall you posting in this thread. I've found the Mayo Clinic-driven work to be inspiring, since that started out as a grass roots effort by some doctors/researchers, like Casadevall, and grew way beyond anything they could have imagined (as Dr. Joyner, head of the Mayo effort has said - he thought they might get 5000 patients via the expanded access program and they got 90,000 so far).
I do think the FDA dropped the ball, here, though, by not insisting on and leading (or finding someone to lead) a randomized clinical trial, especially back in April in NJ/NY, when there were tons of patients and no good options - now it's much tougher as people seriously might not want placebo or standard of care when they could have CP (I wouldn't enroll if I had COVID, I'd just want the plasma). I think the FDA was the only option to run such a trial, since CP is not "owned" by a pharma company that would normally do all the work to plan/execute a clinical trial (with FDA's advice/consent/oversight). What are your thoughts on that?
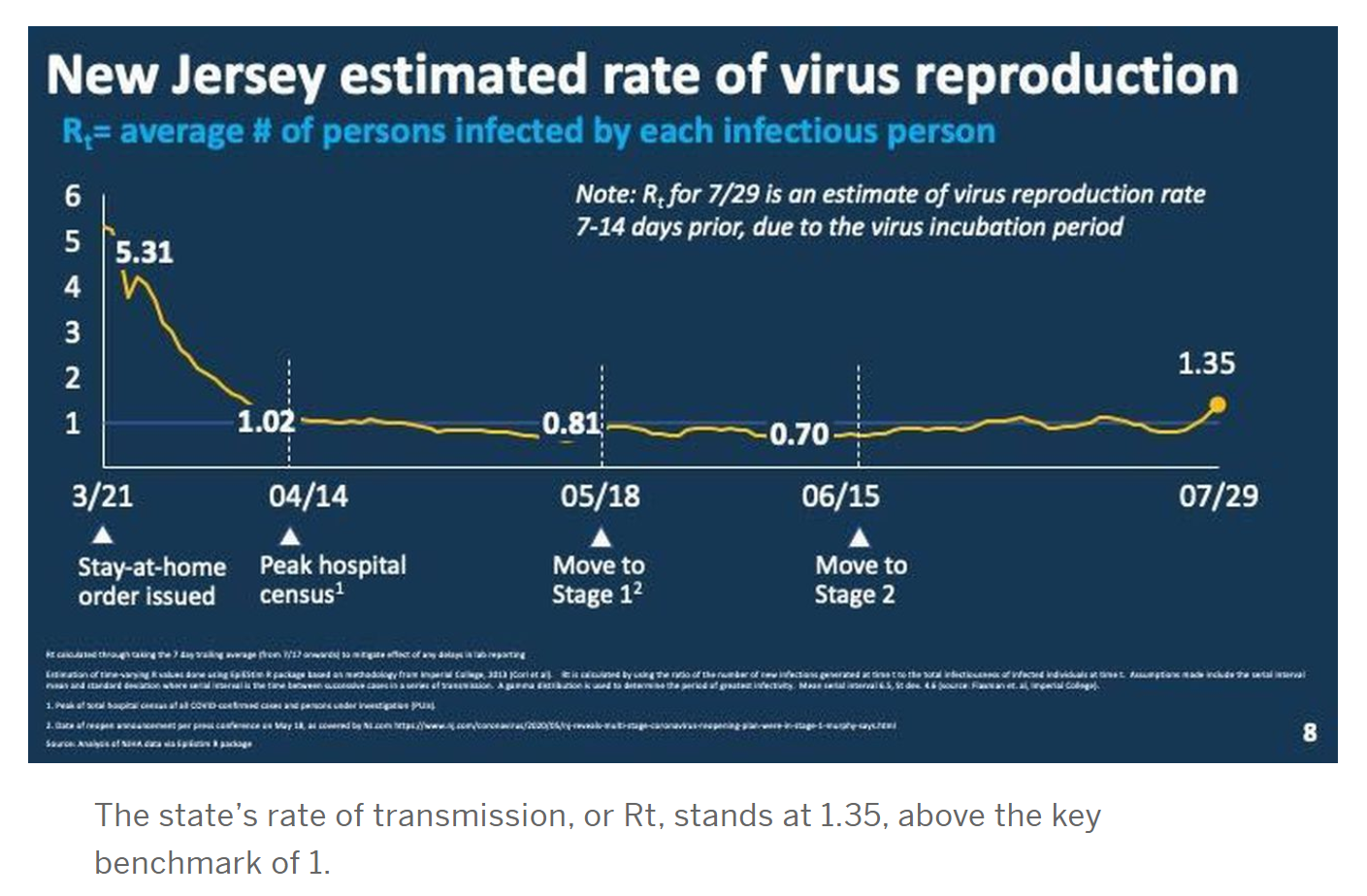
Does anybody know if the RT model that NJ is using has been proven to be an effective model of Covid transmission?
My gut tells me that the Imperial College London model NJ has been using is better than the Rt-live model that many use, as per my post from the other night below. I'd rather have a more sensitive model to see possible changes than one that is too insensitive and might miss important changes in behaviors/transmissions. The obvious downside of that, though, is the potential to overreact to fluctuations that could arise spuriously. I've posted links to both sources before and they're easy to find via Google, if you want more info.
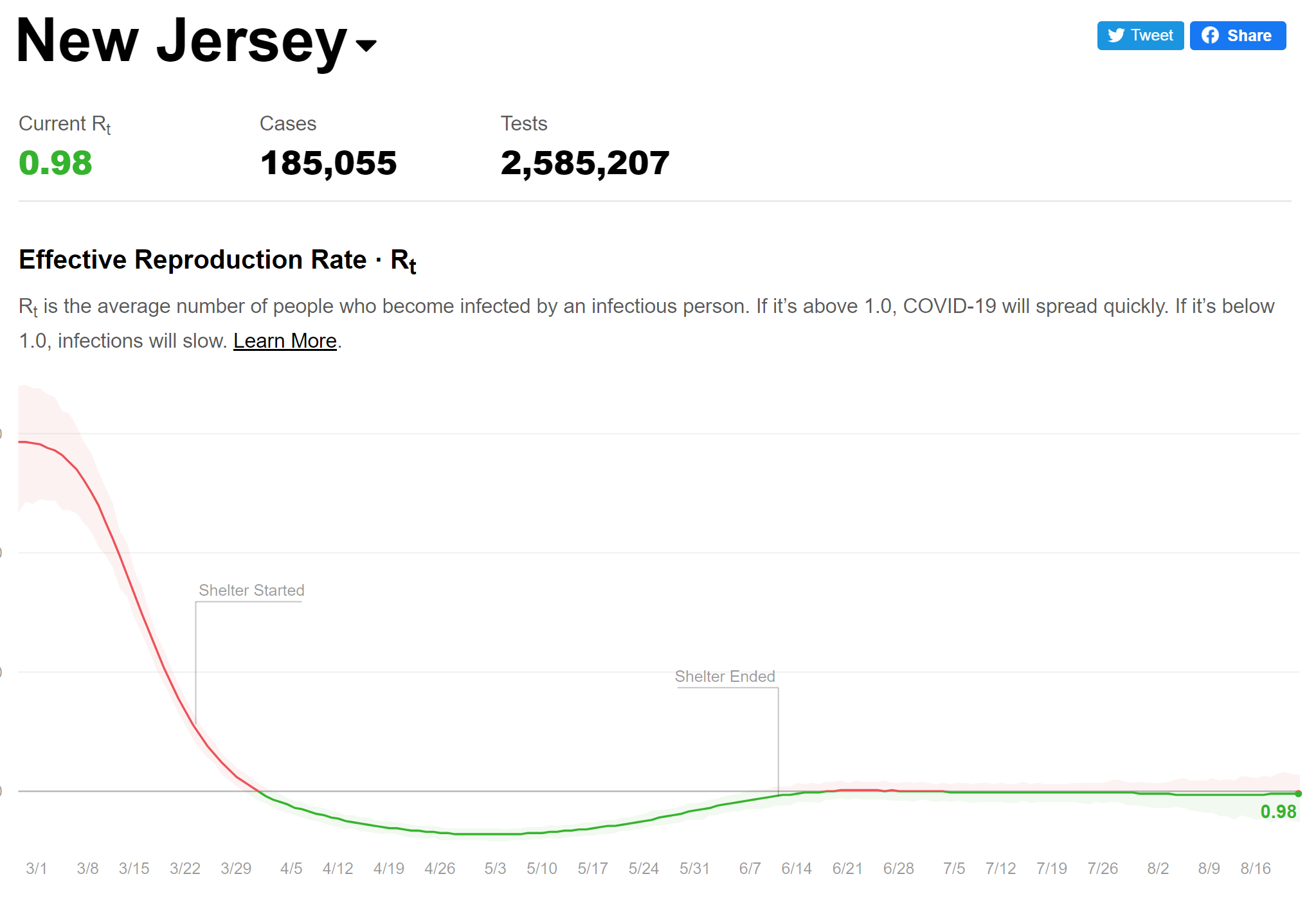
There's no secret that the NJ is using the Imperial College London version of the Rt calculation, built by epidemiologists, instead of the Rt-live version, built by a couple of non-epidemiologists who used to work at Instagram. The fact that it's sometimes (not always - need to go look at the historical charts) higher is a function of the algorithms used.
From what I've read, the Imperial College version is more sensitive to fluctuations about the 7-day moving average, which can be useful or not depending on other factors. For me, I think it's better because of that, since the Rt-live version is just not responsive enough. I think it's even worse that the Rt-live number barely budged when the NJ 7-day avg went from 214 on 7/23 to over 400 in the first few days of August - it should've responded. Rt-live was also around 1 and not moving in mid-June, when the UK one was down around 0.7-0.8, which I'm certain was more accurate, as we were just coming out of shut downs.
Also, there have been delays and batches of data being reported late throughout the pandemic and while that may have influenced the Rt here, there's also no doubt that behaviors in many places across the state (parties/bars) were getting out of hand. You seem to see it as nefarious - I don't. I know you don't like Murphy, but you need more than Kurt whining to convince people that something wrong was done.
Interesting that the Johns Hopkins Corona Virus Resource Center Home page for weeks and weeks had on its front page, a prominently displayed chart for "have countries flattened the curve?" as the US was spiking upwards. But just about a week or so ago, as it became clear the US data was improving dramatically and the case count started on its current steep downward decline..... that chart magically disappeared from its prominent position on their front page! It is still there on its site, but you need to drill down a couple pages to find it. Why are they so afraid of sharing good news? As soon as the news starts to get good.... viola !! Its hard to find. Anyone shocked anymore? Of course the individual state data is still showing fluctuations up and down, so they still keep that chart on the front page were they can highlight in red on that page that there are still hot spots. Even though most of the red zones have mostly been in the less populous states as of late. .
Have Countries Flattened the Curve?
Exactly!
Could mini-mike have something to do with why are they so afraid of sharing good news? Asking for a friend
Johns Hopkins Bloomberg School of Public Health
Michael R. Bloomberg's historic $1.8 billion gift in support of financial aid at Johns Hopkins will fuel student access and mobility, ensuring that a Hopkins education is within reach for qualified, high-achieving students, regardless of their ability to pay.

Bloomberg's record gift helps Johns Hopkins realize key goal of need-blind admissions
$1.8B donation in support of financial aid will allow university to eliminate student loans from financial aid packages for all current and future undergraduateshub.jhu.edu
Some of you will look for conspiracies everywhere. Hint - they simply redid the homepage to make it much more useful, IMO. I like homepages that show a bunch of links to many items of interest rather than focusing on one or two things. It's one simple click from the homepage to the country graphic you're whining about. I don't watch CNN much, but tuned in this morning and they had a story on the significant decline in cases/hospitalizations recently and the likely coming decline in deaths. Of course, as they should, they also had a separate report that reopening schools and the return to colder weather could reverse those trends in the fall, which is quite possible.
Also BIGRU, JHU has been the driving force, via Dr. Casadevall's efforts, for the convalescent plasma effort for months and he and JHU haven't changed how they're discussing plasma at all, so your Bloomberg comment is off-base.
Can’t believe people are still posting about HCQ. Truly bizarre.
"they simply redid the homepage to make it much more useful, IMO."
"IMO" is the key. everyone has one. And I disagree with yours. Thegraphic was a simple snapshot to quickly see if the country is flattening the curve, It was removed. I see nothing more useful about the page now. Everything else is basically still there... just not a quick snapshot to see how a country is doing.... IMO
"IMO" is the key. everyone has one. And I disagree with yours. Thegraphic was a simple snapshot to quickly see if the country is flattening the curve, It was removed. I see nothing more useful about the page now. Everything else is basically still there... just not a quick snapshot to see how a country is doing.... IMO
Has the World hit its peak of COVID transmission ?? Worldwide COVID cases are finally showing an overall downward trend for the first time since it joined the human population! The Worldometer data shows that after a mostly uninterrupted rise, the worldwide 7 day moving average leveled off from Aug 2 to Aug 13 and hovered in and around 260K new cases a day ...and peaked on Aug 13. Now, the last 10 days have seen daily decreases and it appears to be trending downward for the first time. Now down to 247K per day. Finally looking like worldwide it has finally hit its peak. Hope it continues in this direction and we can all get back to our normal lives soon !!
https://www.worldometers.info/coronavirus/#countries
Possibly, although 23.5MM positive cases by viral PCR testing probably means 235MM infected so far (using the general 10:1 ratio of infections to cases, which may be less accurate for the planet), which is about 3% of the world's population, whereas some countries are likely at more like 5-10% infected, with areas with major outbreaks at 15-25%, based on antibody studies. So, it's hard to truly know how many have been infected worldwide, but certainly in urban areas that have 15-25% (and locally up to 40-50% in spots) infected, that's enough to slow transmissions somewhat, even if there were no interventions, just because there are significantly less targets to infect.
My guess is we won't see area-wide major outbreaks in urban areas like we've seen so far, any more, but we will still see plenty of localized flare-ups where there are no controls (masking/distancing, especially indoors), but I just don't see 5-10K+ cases per day outbreaks happening again in hard hit areas, like NY/NJ/LA and now FL, TX, AZ etc. (or London, Paris, Lombardy, etc.). The areas of concern for exponential outbreaks now are areas that were never hit hard so far, like most of East Asia, if they slip up badly from their excellent controls to date (Japan and S. Korea are seeing more cases lately, although far less, still than anywhere in the US per capita), and possibly large swaths of Africa (where the data are less dependable).
Unfortunately, I don't think we'll be anywhere near close enough to herd immunity to allow life to "return to normal" until after we've deployed vaccines in a decent % of the population - and even if we get vaccines approved by the end of the year, it'll take months to get to vaccinating more than those at highest risk.
Yes, but you're making all kinds of conclusions about nefarious political motivations for changing a friggin' homepage, while I wouldn't make any political conclusions either way. You don't think you might be reaching just a bit here?"they simply redid the homepage to make it much more useful, IMO."
"IMO" is the key. everyone has one. And I disagree with yours. Thegraphic was a simple snapshot to quickly see if the country is flattening the curve, It was removed. I see nothing more useful about the page now. Everything else is basically still there... just not a quick snapshot to see how a country is doing.... IMO
And Murphy “ data determines dates” is waiting for what?225 new cases yesterday, Rt down to .85, under 259 Covid+ in the hospitals.
I didn't mention JHU and convalescent plasma, so what are you trying to lecture me about now?Some of you will look for conspiracies everywhere. Hint - they simply redid the homepage to make it much more useful, IMO. I like homepages that show a bunch of links to many items of interest rather than focusing on one or two things. It's one simple click from the homepage to the country graphic you're whining about. I don't watch CNN much, but tuned in this morning and they had a story on the significant decline in cases/hospitalizations recently and the likely coming decline in deaths. Of course, as they should, they also had a separate report that reopening schools and the return to colder weather could reverse those trends in the fall, which is quite possible.
Also BIGRU, JHU has been the driving force, via Dr. Casadevall's efforts, for the convalescent plasma effort for months and he and JHU haven't changed how they're discussing plasma at all, so your Bloomberg comment is off-base.
"EVIDENCE IS STRONGER THAN FOR ANYTHING I"VE EVER STUDIED"
Renowned epidemiologist sees 'massive disinformation campaign' against hydroxychloroquine
*cancer epidemiologist
I quibble because HCQ is not a cancer drug. If this were cut and dry, the President of the United States would be reciting a renowned infectious disease expert, instead of looking for dissenting voices from other fields.
Either there is a conspiracy of silence, or a lack of evidence suggesting this drug is our solution. I find the latter far more likely.
And Murphy “ data determines dates” is waiting for what?
What is the data he is using? How clean is the data? Have these models been proven?
Yes, but you're making all kinds of conclusions about nefarious political motivations for changing a friggin' homepage, while I wouldn't make any political conclusions either way. You don't think you might be reaching just a bit here?
I was "reaching" about the Hopkins site change as much as I am "reaching" regarding the behavior of the apple news app that came with my iphone. Surprisingly, when Biden was officially nominated last week... there was a pop up alert from the Apple News App to tell me about that "breaking" news. (Was this nomination ever in doubt since May?) There have been maybe 2-3 other events that have been newsworthy enough over the last 5 months that resulted in this pop up alert. Meanwhile Trump was officially nominated earlier this afternoon. No alert...... what a shocker !! I guess there was no nefarious political motivation from Apple in that decision either.
Last edited:
Great post and agree with everything you've said. Having been under the tent to a degree with the FDA on this since March, it was clear that they were trying to get as many shots on goal as possible and fast tracking everything. I sensed a panic on the calls but also an all-hands type of response that was pretty inspiring to be honest. I have seen the Mayo data and also enough anecdotal cases to feel the same way. If I was admitted and tested postive, I would ask for a CCP transfusion immediately.
However, while we agree that CP is likely helpful and have no issues with its use, I think we should all be a bit concerned with how this is being politicized, as I said earlier. Derek Lowe has a blog entry on this today and he never gets political (have maybe seen this 2-3 times in 20 years of following his blog), but he did today (link below) and makes some great points. He expressed great concern over the FDA invoking the Administration in their communication of the emergency use authorization (he says it's the first time he's ever seen that and it's very inappropriate), as well as calling it a "major breakthrough" when it's not, really.
He also shared the concern of many that the FDA way overstated the case for CP in their announcements, as the 35% mortality reduction from the high/low titer treatment evaluations cannot be stated with confidence from a non-RCT with potential differences in the populations being treated (2nd link). This is not the way to announce something like this and plants seeds of doubt about the independence of the FDA (which is supposed to be sacrosanct), which will likely translate into skepticism about the safety and efficacy of any vaccines that the FDA approves, especially if they're approved without full transparency and with this kind of hoopla. I'm not going to go further, as it will likely get bogged down in politics, but we do not need people starting to wonder about the independence of the FDA.
Science | AAAS
You implied Bloomberg was influencing JHU to not share "good news" on CV and I showed an example where JHU is sharing plenty of good news on plasma to make it clear that if that's what Bloomberg is doing, he's not doing it very well.I didn't mention JHU and convalescent plasma, so what are you trying to lecture me about now?
Sure, I am involved on the collection side and have been on several calls with Dr. Joyner. I used to post on the CE Board on this topic quite a bit (back to March) but when that collapsed I stopped coming to this site altogether. Given the announcement yesterday, I decided to come back and noticed that OT topics are being discussed on the Football board.Interesting perspective - can you share what your role has been on this? Maybe I missed it, but don't recall you posting in this thread. I've found the Mayo Clinic-driven work to be inspiring, since that started out as a grass roots effort by some doctors/researchers, like Casadevall, and grew way beyond anything they could have imagined (as Dr. Joyner, head of the Mayo effort has said - he thought they might get 5000 patients via the expanded access program and they got 90,000 so far).
I do think the FDA dropped the ball, here, though, by not insisting on and leading (or finding someone to lead) a randomized clinical trial, especially back in April in NJ/NY, when there were tons of patients and no good options - now it's much tougher as people seriously might not want placebo or standard of care when they could have CP (I wouldn't enroll if I had COVID, I'd just want the plasma). I think the FDA was the only option to run such a trial, since CP is not "owned" by a pharma company that would normally do all the work to plan/execute a clinical trial (with FDA's advice/consent/oversight). What are your thoughts on that?
Agree on your perspective on the FDA although their energy (rightfully so) was focused on getting the industry to collect the plasma, which was not an easy task. For instance, the Red Cross decided to bail on the agreed upon process at the 11th hour in April, forcing the rest of the industry to scramble unnecessarily. At some point they should have doubled back on the RCT. I also not enroll in the study at this point for the reasons you cited.
Hal Turner is claiming that the test for COVID-19 is actually for something else,possibly a Trojan horse.
He says that will reveal what it is on his internet radio show tonight.
This is likely his way of raising funds,but as Joaquin Andujar said:youneverknow.
He says that will reveal what it is on his internet radio show tonight.
This is likely his way of raising funds,but as Joaquin Andujar said:youneverknow.
Unfortunately, this is being politicized like you said and it shouldn't be. Trump brought that on by making the announcement right before the convention, but the MSM and anti-Trumpers would have done the same thing if he announced it any other time.However, while we agree that CP is likely helpful and have no issues with its use, I think we should all be a bit concerned with how this is being politicized, as I said earlier. Derek Lowe has a blog entry on this today and he never gets political (have maybe seen this 2-3 times in 20 years of following his blog), but he did today (link below) and makes some great points. He expressed great concern over the FDA invoking the Administration in their communication of the emergency use authorization (he says it's the first time he's ever seen that and it's very inappropriate), as well as calling it a "major breakthrough" when it's not, really.
He also shared the concern of many that the FDA way overstated the case for CP in their announcements, as the 35% mortality reduction from the high/low titer treatment evaluations cannot be stated with confidence from a non-RCT with potential differences in the populations being treated (2nd link). This is not the way to announce something like this and plants seeds of doubt about the independence of the FDA (which is supposed to be sacrosanct), which will likely translate into skepticism about the safety and efficacy of any vaccines that the FDA approves, especially if they're approved without full transparency and with this kind of hoopla. I'm not going to go further, as it will likely get bogged down in politics, but we do not need people starting to wonder about the independence of the FDA.
Science | AAAS
blogs.sciencemag.org
I really only care about the science and I do believe there is no downside from what I can see in treating patients, even if we don't have a study completed.
COVID-19 Pandemic: Transmissions, Deaths, Treatments, Vaccines, Interventions and More...
Relatives and friends of those who died certainly will remember. Many books and scholarly papers will still be studied 20 years from now. We have a lot to learn about this virus and those that may come after. Preparation and response will be better. This virus and response will not...
 rutgers.forums.rivals.com
rutgers.forums.rivals.com
Missed this correspondence/paper before...which shares more clinical data showing that HCQ is not effective as a prophylactic in patients with lupus or rheumatoid arthritis. As per the above post, I've been talking about this one for a long time and it's good to see more comprehensive clinical data being shared finally. This study clearly shows that HCQ has no clinical benefit in preventing COVID in these at-risk patients. While this doesn't absolutely confirm that HCQ wouldn't be an effective prophylactic in normal patients, it certainly suggests that to be the case. This was just HCQ use, as these patients don't take azithromycin or zinc.

New Research Finds Hydroxychloroquine Is Not a Possible Defense Against COVID-19
Hydroxychloroquine (HCQ) ineffective as a preventive antiviral against COVID-19. Researchers at Case Western Reserve University have added to the growing body of understanding about how hydroxychloroquine (HCQ) is not a possible defense against COVID-19. Specifically, they found that HCQ is n
scitechdaily.com
“Our study shows, with a large degree of confidence, that HCQ is ineffective as a preventive antiviral in people with SLE (lupus) and/or RA taking drugs that suppress their immune system, putting them at greater risk,” said Mendel Singer, PhD, MPH, lead author and associate professor and vice chair for education in the Department of Population & Quantitative Health Sciences at the Case Western Reserve School of Medicine. “Given how the study was structured, one can make an educated extension that it is not effective in preventing COVID-19 in people without those conditions. It is not uncommon for something to show promise in the lab, and then prove ineffective in the more complex biological landscape of humans.”
Unfortunately, this is being politicized like you said and it shouldn't be. Trump brought that on by making the announcement right before the convention, but the MSM and anti-Trumpers would have done the same thing if he announced it any other time.
I really only care about the science and I do believe there is no downside from what I can see in treating patients, even if we don't have a study completed.
Are you a doctor?
Noooo
Sorry, read your post wrong! Would be cool to see how board doctors feel about CP and how it stacks up against some other therapies.
We were specifically discussing the simple covid case snapshot being removed from the JHU homepage just as that graphic was showing an improved situation for the U.S. So yeh that would have a political smell to it since it is a quick summary for the general viewing public to see and understand....IMO.You implied Bloomberg was influencing JHU to not share "good news" on CV and I showed an example where JHU is sharing plenty of good news on plasma to make it clear that if that's what Bloomberg is doing, he's not doing it very well.
I don't see this summary snapshot graphic vs. a more detailed presentation of CP therapeutic advances for those interested in that level of detail as the same at all vis-a-vis a political perspective...although we'll see how JHU handles the CP developments now that it appears to quickly becoming a political issue.
Last edited:
@RU848789 this is the third request for you to address Rt. You mock Rt live and say the states model is better, despite the wild fluctuations which I believe to be the result of reporting errors. For he last time, here are scientific criticisms of NJs Rt. If you are confident that NJs model is superior to that of RtLive, would you address them or should I assume you don't have an answer?@RU848789 asking for your review and thoughts.
Hal Turner is claiming that the test for COVID-19 is actually for something else,possibly a Trojan horse.
He says that will reveal what it is on his internet radio show tonight.
This is likely his way of raising funds,but as Joaquin Andujar said:youneverknow.
Conspiracy by the vegetable industry to blunt our senses of smell and taste
Or an agenda@RU848789 this is the third request for you to address Rt. You mock Rt live and say the states model is better, despite the wild fluctuations which I believe to be the result of reporting errors. For he last time, here are scientific criticisms of NJs Rt. If you are confident that NJs model is superior to that of RtLive, would you address them or should I assume you don't have an answer?
@RU848789 this is the third request for you to address Rt. You mock Rt live and say the states model is better, despite the wild fluctuations which I believe to be the result of reporting errors. For he last time, here are scientific criticisms of NJs Rt. If you are confident that NJs model is superior to that of RtLive, would you address them or should I assume you don't have an answer?
Not sure what you're asking about. I addressed your original questions early Saturday about how Rt was calculated and showed that the UK model did not always show a higher Rt than the Rt-live site - it's just that it's more sensitive to changes than the Rt-live site, which I prefer, while you may not. I've also never "mocked" Rt-live and not sure why you said I did.
COVID-19 Pandemic: Transmissions, Deaths, Treatments, Vaccines, Interventions and More...
Whine? I Report positive news. You hope for bad news. Why? I don't root for bad news at all. "Good news" is all relative these days, tho. You whine about restaurants and gyms every day, no matter what. You think that's having an impact? It's just a pretty weak look. Take a long weekend -...
rutgers.forums.rivals.com
Edit: @DJ Spanky - hey, just curious, the text one sees when looking at the post of mine I linked above is actually from multiple other posts by other people, (including one from King of S at 1:44 pm on Friday and fsg's follow-up to that post a few hours later), not from my post, but if you click on the post link, it does bring you to my post. Thought that was really weird - any explanation?
The twitter thread you posted isn't very helpful in explaining your point, although I'll admit I don't use Twitter much so maybe I'm missing something - all I see is Kurt talking about how deaths are reported in the UK. You've mentioned reporting errors, as did Murphy.
Do you have confirmation that numbers around 7/20, which were a local minimum, and numbers by the end of July, which were a local maximum, were due purely to reporting errors with regard to timing? It's one thing to hear that there were reporting issues (which there have been throughout the pandemic, as it's hard, in the midst of chaos to always get the data correct) and another to know exactly what happened.
If you're right, then yeah, Murphy shouldn't have used rising numbers and a rising Rt as justification for adding restrictions, although he wasn't making things up about a spate of well-publicized incidents of really bad behaviors around the state.
Regardless, looking at the case numbers and the transmission numbers now from both Rt sites, it certainly seems like NJ could be at least incrementally reopening things to, say, NY's level. And Murphy said so much today. I also don't buy the "power trip" angle at all - I just think he truly doesn't want to see us slip back like so many other places have - and it's certainly not something that's making him more popular.

Gov. Murphy Suggests Reopening Gyms, Indoor Dining On Horizon In New Jersey
Dining out in New Jersey, one of the slowest states in the country to reopen, still means dining outside. There's now a glimmer of hope.
 newyork.cbslocal.com
newyork.cbslocal.com
Last edited:
If anyone ever doubted the stupidity of some Americans, never fear, they're still here. If it weren't so sad and dangerous I'd be tempted to laugh, as I just never thought I'd see something like this.
 dfw.cbslocal.com
dfw.cbslocal.com
 www.kxan.com
www.kxan.com
CBS Texas - Breaking Local News, First Alert Weather & I-Team Investigations
Latest breaking news from CBS11 KTVT-TV | KTXA-TV.
dfw.cbslocal.com
Don’t drink bleach: Texas Poison Center Network getting 100s of calls about ingesting cleaning products
Data shows across the state, 278 calls were received about ingesting bleach among people 30-years and older between March 1 to June 5. More than three hundred calls were about children 5 years or y…
No issue with masks for the sick and those with symptoms
My whole point is this spreads..masks or no masks. Virus going to virus...look at Cali..Hawaii..Austrailia..spain..Italy..hong ko g
Look at Germany, Japan , South Korea.
COVID deaths well below 10,000 ( 1,000 in Japan) while the US is at 177,000.
However, while we agree that CP is likely helpful and have no issues with its use, I think we should all be a bit concerned with how this is being politicized, as I said earlier. Derek Lowe has a blog entry on this today and he never gets political (have maybe seen this 2-3 times in 20 years of following his blog), but he did today (link below) and makes some great points. He expressed great concern over the FDA invoking the Administration in their communication of the emergency use authorization (he says it's the first time he's ever seen that and it's very inappropriate), as well as calling it a "major breakthrough" when it's not, really.
He also shared the concern of many that the FDA way overstated the case for CP in their announcements, as the 35% mortality reduction from the high/low titer treatment evaluations cannot be stated with confidence from a non-RCT with potential differences in the populations being treated (2nd link). This is not the way to announce something like this and plants seeds of doubt about the independence of the FDA (which is supposed to be sacrosanct), which will likely translate into skepticism about the safety and efficacy of any vaccines that the FDA approves, especially if they're approved without full transparency and with this kind of hoopla. I'm not going to go further, as it will likely get bogged down in politics, but we do not need people starting to wonder about the independence of the FDA.
Science | AAAS
Was very happy to see FDA Commissioner Hahn publicly acknowledging his mistaken take on plasma last night in a tweet tonight, after much criticism today in the scientific community (like the article above and the one from the Times earlier today). This was a huge, important step for those concerned about the independence of the Agency.

F.D.A. ‘Grossly Misrepresented’ Blood Plasma Data, Scientists Say (Published 2020)
Many experts — including a scientist who worked on the Mayo Clinic study — were bewildered about where a key statistic came from.
but virus gonna virusLook at Germany, Japan , South Korea.
COVID deaths well below 10,000 ( 1,000 in Japan) while the US is at 177,000.
"Virus gonna virus" might be the dumbest thing bac has ever posted and he posts it regularly.but virus gonna virus
Japan is having its most serious spike of the pandemic, with near/over 1000 cases per day the past few days, although it's worth noting for comparison, that that would translate to about 2500 cases per day in the US, where we've been averaging 65,000, roughly, so it's bad, but not very bad - yet - will be interesting to see if they can get control of this (my guess is yes). Their death rate is about 8 per 1MM (vs. ours of 470/1MM).
They've been one of the model countries, so far, with near universal mask-wearing and impressive contact tracing through their health care system. As in the US, most of the cases are coming from the young; their clusters have originated in gyms, pubs, music venues, karaoke rooms, and "hostess" rooms, but not from their notoriously packed subways (probably due to better masking, shorter exposures and less talking). It just goes to show, though, how easily transmissions can jump up so quickly.
https://english.kyodonews.net/news/...-new-coronavirus-cases-record-daily-rise.html
https://www.sciencemag.org/news/2020/05/japan-ends-its-covid-19-state-emergency
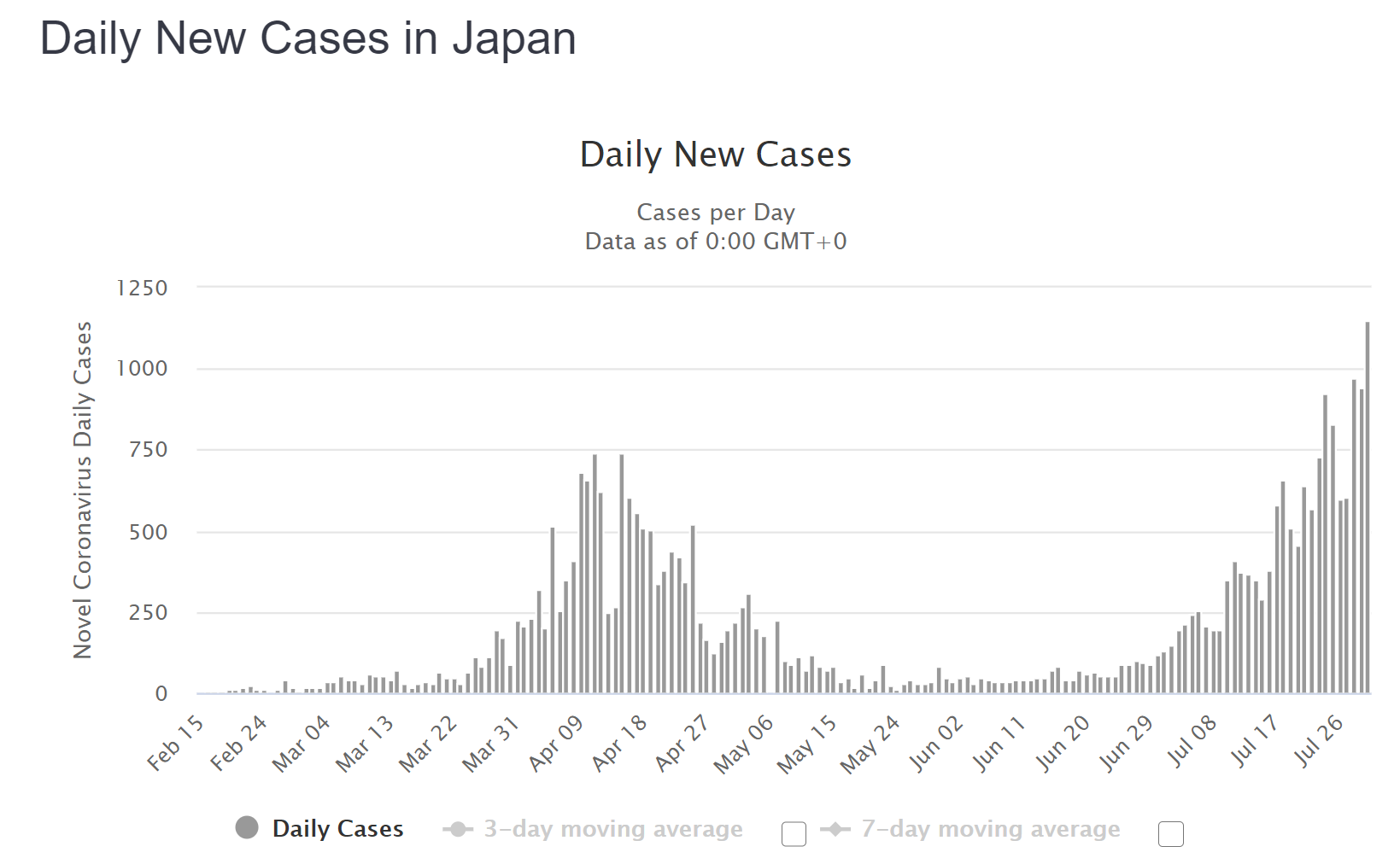
Looks like Japan was able to control their latest spike, as expected, at right around the peak where it was a few weeks ago, i.e., the 7-day moving average peak was about 1350 cases per day and is now back down below 1000/day. For comparison purposes, that's equivalent to about 3500 cases/day in the US and the recent US peak was about 67,000 cases/day, so on a per capita basis our peak was about 19X greater than Japan's. My guesstimate is it's likely going to raise their deaths per 1MM from 8 to about 25 vs. our 550 deaths/1MM - which will likely be close to 900/1MM by Dec.
Let's look at a few other countries that had been doing very well, but have lately had some significant spikes that had some folks around here thinking that this might invalidate their superb, proactive interventions, to date and might not be able to be easily controlled by short shutdowns and stricter mask/distancing policies. Doesn't look like it.
First let's look at Australia, which also just had a spike which now appears to be under control. Their 2nd wave peaked around 475 cases/day and is now down below 250 cases/day, as their interventions have been effective. For comparison purposes, that's equivalent to about 6175 cases/day in the US and the recent US peak was about 67,000 cases/day, so on a per capita basis our 2nd wave peak was about 11X greater than Japan's. My guesstimate is it's likely going to raise their deaths per 1MM from 5 before the spike to about 25-30/1MM (similar to Japan's) vs. our 550 deaths/1MM.
Second, let's look at New Zealand. They thought they had completely eradicated the virus, but somehow someone brought the virus in (probably some shipping/delivery contact) and they had an outbreak in Auckland that jumped up to 10-15 cases per day; by acting swiftly to shut Auckland down and conduct extensive testing, tracing and isolating, they're back down to single digit cases per day and expect to start relaxing restrictions again by this weekend. This small spike is much smaller than the one they had in March, so they're unlikely to see their 4 deaths/1MM increase much. Also, fwiw, SK has had, by far, the least GDP impact of any country in the world, since they haven't had to resort to significant lockdowns yet.
New Zealand extends Auckland lockdown, Australian COVID-19 cases fall to seven-week low
New Zealand Prime Minister Jacinda Ardern on Monday extended a coronavirus lockdown in the country's largest city until the end of the week and introduced mandatory mask wearing on public transport across the nation. Ardern said the four-day extension in the city of Auckland was critical to...
Finally, let's look at South Korea, which is in the midst of their biggest outbreak since March (where they had 600-800 cases per day), with 300-400 cases per day, but the increase has slowed, as SK has increased restrictions for public gatherings (most of the cases came from churches in Seoul) and reiterated the need for masks in public. My guess is their very proactive systems will allow them to control this outbreak too. If they do control it at current levels, it's likely their deaths per 1MM could jump from 6 to about 10 per 1MM - again vs. the US's 550/1MM and rising quickly.
These examples of recent outbreaks show how difficult it is to maintain control of this virus - not impossible, with very proactive testing/tracing/isolating augmented by masking/distancing (and occasionally shutdowns), but clearly difficult. If these countries can hang on a few more months without even more major outbreaks, until better treatments/vaccines are available, they'll have saved tens/hundreds of thousands of lives and 3-5X that many serious illnesses and will become the models for how to handle pandemics - even moreso than they already are.


- Status
- Not open for further replies.
Similar threads
- Replies
- 47
- Views
- 3K
- Replies
- 472
- Views
- 21K
- Replies
- 136
- Views
- 5K
- Replies
- 90
- Views
- 3K
- Replies
- 25
- Views
- 2K
ADVERTISEMENT
ADVERTISEMENT