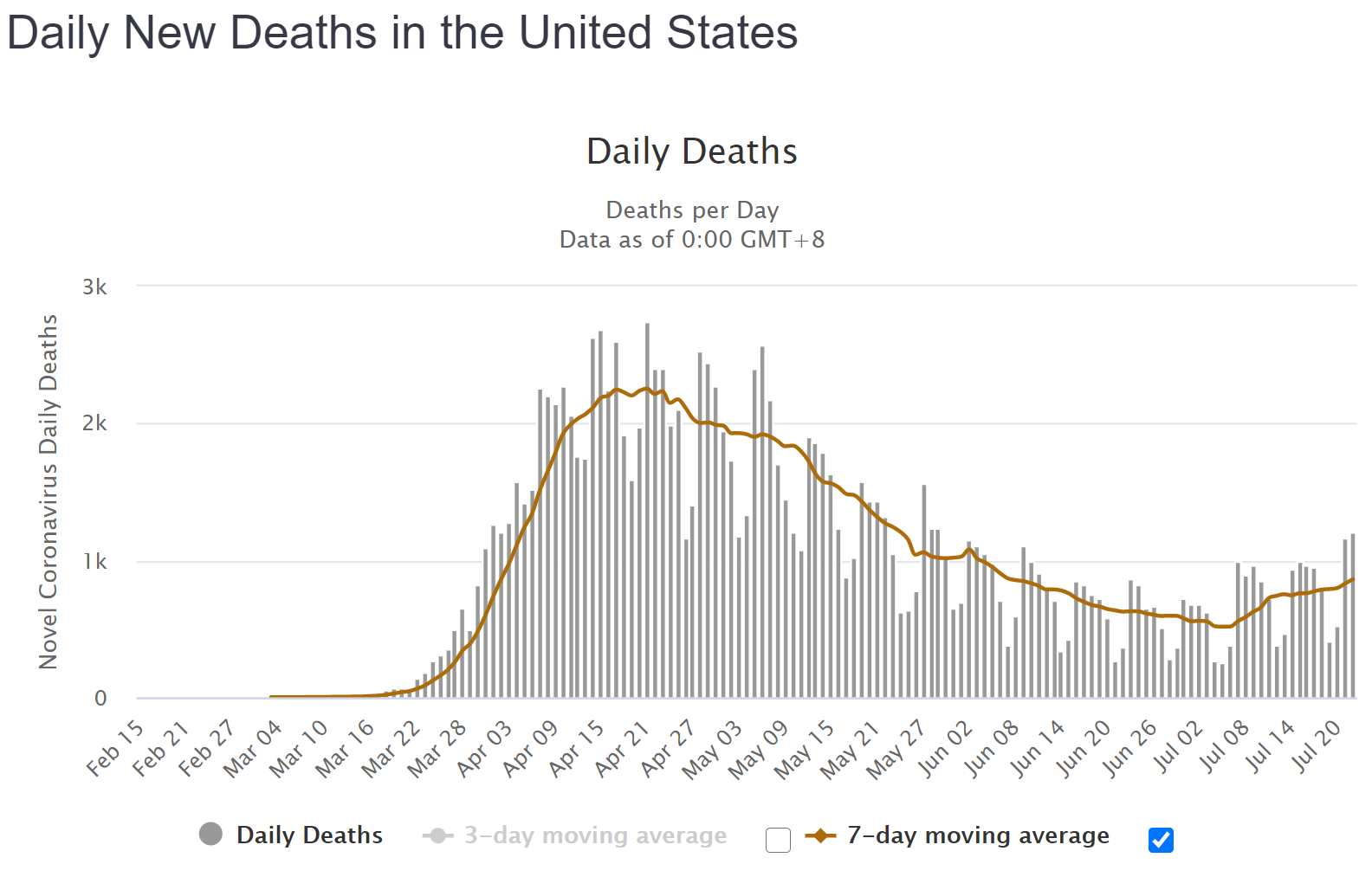
I don't have time for a full analysis of multiple states every night, like last night, but checking in on the national numbers is pretty easy. Below is the Worldometers detailed graphic of deaths, with today's total of 1205 being the highest number since 5/29 and close to 50% of the highest daily peaks in April.
https://www.worldometers.info/coronavirus/country/us
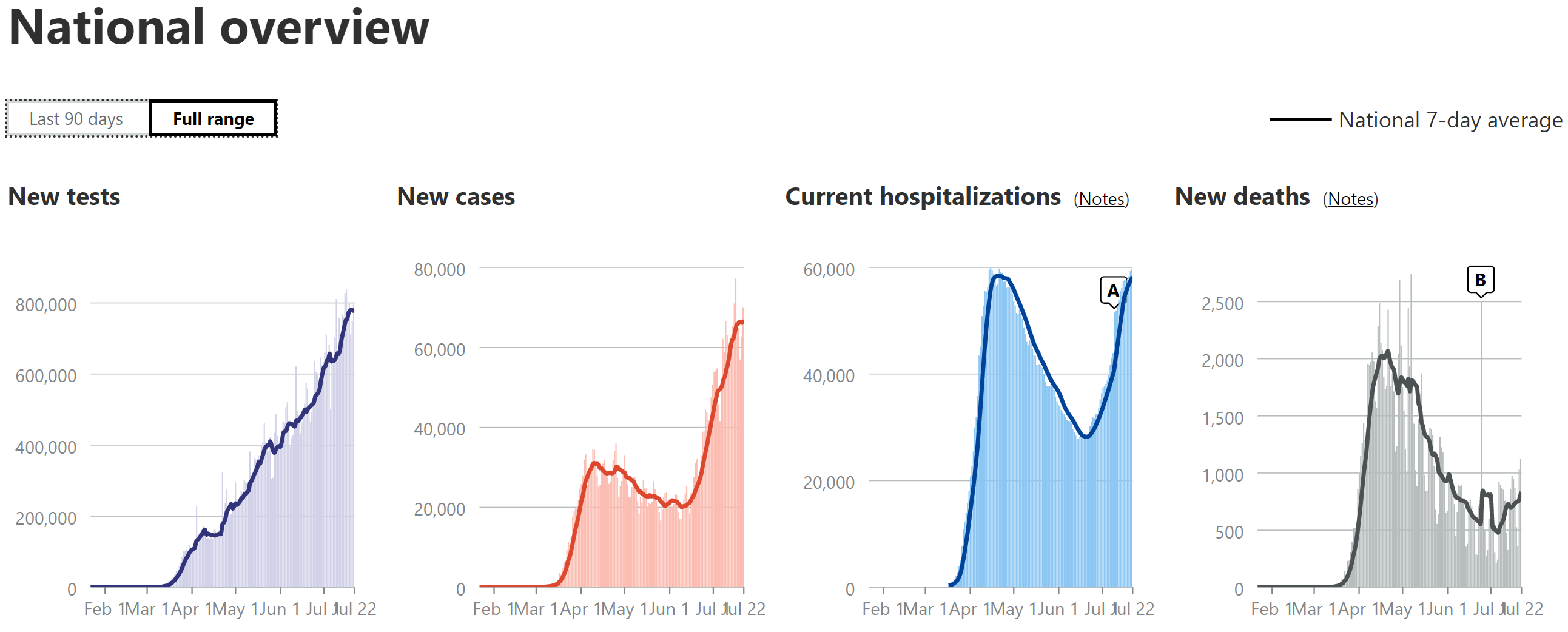
Below that are the COVID Tracking charts of tests, cases, hospitalizations, and deaths, all on 7-day moving averages, showing cases about 2x what they were during the first wave and hospitalizations being about equal to those in the first wave (but haven't peaked yet, while cases have and the accuracy of the hospitalization data is questionable), which is very likely due to a much younger population being infected than in the first wave and is why it's likely that deaths will likely remain significantly less than what we saw in the first wave (coupled with improved treatments/procedures).
https://covidtracking.com/data#chart-annotations