C'mon man, you've been on this thread long enough that you should know the obvious examples.Really, where?
You should also know the numerous resources out there which posts such information.
C'mon man, you've been on this thread long enough that you should know the obvious examples.Really, where?
Examples of what? Maybe I skipped a few of "Greg's" troll posts?C'mon man, you've been on this thread long enough that you should know the obvious examples.
You should also know the numerous resources out there which posts such information.
He only reads the posts he agrees with.C'mon man, you've been on this thread long enough that you should know the obvious examples.
You should also know the numerous resources out there which posts such information.
Nope. I just read yours. But to be fair I do skip most of "Greg's" trolling.He only reads the posts he agrees with.
I'm so honored.Nope. I just read yours. But to be fair I do skip most of "Greg's" trolling.
South Korea, Taiwan, Thailand, Vietnam, New Zealand, Australia, Germany, Hong Kong, sri lanka, estonia, ice land, uruguay, cambodia, mongolia, bermuda, barbados,uganda, zimbabwe, finland, croatia, greece, denmark, czech republic, austria, switzerland, portugal, japan, amongst others.Really, where?
His sister told him his brother in-law was very busy with work which is why he was coming home so late. I guess not.Where are you getting that? I see that the 7DMA is around 540, it was at 940 on July 31st. Huge decrease.

 www.independent.co.uk
www.independent.co.uk
They have alternative "facts".Another HCQ study
Drug cocktail touted by Trump increases chance of death by 27%, claims new study
‘No need for further studies’ into unproven Covid-19 treatment supported by US president, researchers say
Another HCQ study
Drug cocktail touted by Trump increases chance of death by 27%, claims new study
‘No need for further studies’ into unproven Covid-19 treatment supported by US president, researchers say
HCQ more success.
Large scale observational study shows a 30% decrease in mortality in 3,451 hospitalized patients-late treatment, not early use.

Use of hydroxychloroquine in hospitalised COVID-19 patients is associated with reduced mortality: Findings from the observational multicentre Italian CORIST study
Hydroxychloroquine (HCQ) was proposed as potential treatment for COVID-19.We set-up a multicenter Italian collaboration to investigate the relationshi…www.sciencedirect.com
Retrospective study of 8,075 hospitalized patients shows a 35% reduction in mortality
Low-dose hydroxychloroquine therapy and mortality in hospitalised patients with COVID-19: a nationwide observational study of 8075 participants
Hydroxychloroquine (HCQ) has been largely used and investigated as therapy for COVID-19 across various settings at a total dose usually ranging from 2…
But, but, but . . . . . .
Wait for it . . . .I'm just going to put this out there for others to look at regarding Hydroxychloroquine.
Dr. John Campbell from England has been doing daily videos on covid since January. I watched most of the early ones but eventually lost interest (covid fatigue). He has generally been very conservative and measured in his statements regarding covid and various treatments, quite the opposite of Chris Martenson who has been rabidly arguing for HCQ for months. So this one caught my eye. He reviews the recent Belgium study (link in the quoted message above) as well as several others that both support and don't support use of HCQ.
I won't post my opinion on this, will just leave it for others to consider. It's about 36 minutes but he does state his conclusions pretty early on. I'm curious about what others think.
Dr. John Cambell video on HCQ
Frankly, I've become rather tired of "it".Wait for it . . . .
I’ve made my opinion on HCQ clear. I’m quite liberal. Supported Sanders, despise Trump. But I believe it’s at least somewhat effective. And I know for a fact it’s been politicized like I’ve never seen medicine politicized in my life. And due to that, we may never know the full and honest truth. Absolutely tragic, and both sides are extremely guilty.I'm just going to put this out there for others to look at regarding Hydroxychloroquine.
Dr. John Campbell from England has been doing daily videos on covid since January. I watched most of the early ones but eventually lost interest (covid fatigue). He has generally been very conservative and measured in his statements regarding covid and various treatments, quite the opposite of Chris Martenson who has been rabidly arguing for HCQ for months. So this one caught my eye. He reviews the recent Belgium study (link in the quoted message above) as well as several others that both support and don't support use of HCQ.
I won't post my opinion on this, will just leave it for others to consider. It's about 36 minutes but he does state his conclusions pretty early on. I'm curious about what others think.
Dr. John Cambell video on HCQ
You know what we are going to get. This guy does not have the right credentials, enough published papers, he is not recognized as an expert, blah, blah, blah. I am skeptical of what Big Pharma and the FDA push. Closely studied the so-called and science on statins. A lot of junk RCTs pushing nonsense.Frankly, I've become rather tired of "it".
Update on Hawaii 08/27/2020 ... 306 more positives... testing is showing a 11% positivity rate... which I’m told is a danger now to overwhelm their healthcare system... oh Hawaii population on Oahu is 875 K not million...the population has nothing to do with the rate. The death RATE is based on population. AKA a death in Hawaii with 875k = 10 deaths in a state with 8.75 million population as far as rate is concerned. It's a per capita thing.
Didn't post "it" three times. I posted 3 distinct quotes. Let's agree to disagree. You have a tendency to shout down other posters and to criticize either the authors of studies or the studies themselves if it does not agree with your opinion on HCQ. The jury is still out IMO, and there is ample evidence that HCQ can have efficacy.
See the tweet from Professor Francois Balloux.
"Many excellent scientists were completely unprepared to deal with the fear and anger the pandemic unleashed, and found it difficult to get their voices heard. "
And on an unrelated topic this (showing that , just like with HCQ, there has been a lot of either one or both biased and really sloppy "science" propounded in the pandemic):
The other part that I left out was that back in Feb South Korea was recommending Hydrocholoriquine as part of it's treatment protocol and I believe that some Chinese doctors were also recommencing it.
There are some people on this board who point to South Korea as a model of pandemic response.
Here is a report from March 12th.

South Korea experts recommend anti-HIV, anti-malaria drugs for COVID-19 - UPI.com
South Korean disease experts have begun to recommend the use of a combination of antiviral and anti-malaria drugs for patients of the new strain of coronavirus.www.upi.com
South Korean experts are also recommending the use of hydroxychloroquine in combination with the anti-HIV medication. HCQ is sold under the brand name Plaquenil, among others, and is used for the prevention and treatment of malaria.
Here is a report from Feb.
Seoul recommends use of anti-HIV drug for COVID-19 treatment - Pulse by Maeil Business News Korea
South Korean government endorsed use of Kaletra, a combination of two anti-HIV drugs, to treatment novel coronavirus (COVID-19)-infected patients who are old or severely ill, or have other underlying diseases. The governmpulsenews.co.kr
All of this is at the beginning of the pandemic. The President sees some evidence of a widely used, cheap and safe (safe being a relative term in the world of drugs) drug that may help stop the spread and asks the FDA to fast track it. I think that's a pretty good decision but because of our fractured culture he is attacked.
Now I believe that since then HCQ has proven not to be as effective but in the early stages this seemed like a good idea.


 rutgers.forums.rivals.com
rutgers.forums.rivals.com
Hello? Bueller?

 www.medscape.com
www.medscape.com
Yes, I've posted about this one (MK-4482) a few times, since I used to work there and have some knowledge of the compound, as I may end up consulting on this one for them (I retired, but I've been doing some part-time consulting on other projects since then). My gut tells me that the potential markets for antivirals like remdesivir (annoying that that article kept calling it Veklury, a name nobody uses) and MK-4482 might dry up quickly this fall once positive results (and I expect very good positive results) are announced for the various engineered antibody cocktails. However, such success is not a given, so Merck and Gilead will keep plugging away on the antivirals and even if the antibodies are pretty successful, it's possible that a combo with an antiviral would be even better or that an antiviral might be used in cases where antibodies don't work as well.Not sure if this has been posted or not...but news on the treatment front...
Bloomberg - Are you a robot?
www.bloomberg.com
Hello? Bueller?
Peggy Noonan comes out swinging in WSJ, addressing the RNC’s treatment of the Coronavirus response:
“We are not a third-rate banana republic but at the moment we’re imitating one.
The president’s leadership in the coronavirus epidemic was lauded as timely and visionary...He denied the threat, lied with an almost pleasing abandon, especially about testing, and when forced to focus held bumbling daily briefings that only made things worse.
It was a mistake to insist it was a success. That ship has sunk.“
Complete political post that doesn't belong in this thread
Please watch the YouTube video posted above. It is very well done and science-based. Either one of two things happened: (1)the anti-HCQ crowd purposefully cooked their results by giving a higher dose to obtain bad results; (2) the people running the studies with the bad results were idiots. Let's face it, big Pharma had nothing to gain from HCQ, and some were going to do everything they could to deep six the results. Others hate the guy who promoted HCQ and they did not want to see it promoted as successful, perhaps because they feared backlash.You posted the Doidge article on 8/16, then posted it twice within 2 minutes yesterday, which is three times by my count, but that's unimportant really. I certainly didn't "shout you down" then or now, but I disagree strongly with Doidge here. Sometimes I show little patience with people who don't do their homework or who aren't really trying to make relevant points, but I don't feel I did that with you now or two weeks ago, as I can tell you're making legitimate points that need to be discussed (and there's a ton of general stuff in the Doidge article that's very well done - I just disagree strongly with his application of that to the HCQ case). Anyway, I don't think he's done any clinical studies himself - and neither have I, but I spent much of my 30 years in Pharma learning quite a bit about clinical trial design from some of the world's foremost clinicians (leading to about 8 different major drug approvals I was involved in) and all of them wouldn't even consider doing observational studies for drug approval vs. RCTs.
I also checked in with two of these old clinical colleagues of mine recently and had discussions with them about HCQ and they were unequivocal in their opinions that RCTs are usually (but not always as Doidge pointed out - there can be bad RCTs too) better than observational trials and that in the HCQ case the RCTs (especially the Spanish study on prophylaxis and the Recovery trial in hospitalized patients) were very well run and that the most prominently cited observational trials - those by Raoult and the Ford study - were very badly designed and run. And this is exactly what both Gorski and Gavura said in the articles I linked yesterday and I focused on also.
We can agree that there has been a lot of sloppy science conducted during this pandemic (including the two I mentioned above and the Lancet trial on HCQ and the one on ACE-inhibitors using data from the apparently fraudulent Surgisphere group).
This is am incomplete picture. First off, South Korea may have started recommending HCQ plus antivirals on 3/12, but their major outbreak was over by 3/12, so it had no impact on their low mortality rate. Prior to then it was simply one of a couple dozen drugs on the list of compounds that could be used. HCQ is no longer on their list of recommended drugs.
[News Analysis] Breakdown of drugs currently used to treat coronavirus
With experts suggesting that it will take one to five years for a vaccine for the new coronavirus to be developed from scratch, researchers are redirecting existing drugs and pipelines in an effort to control the outbreak. On Tuesday, Gilead Sciences’ Ebola treatment remdesivir was approved for...www.koreaherald.com
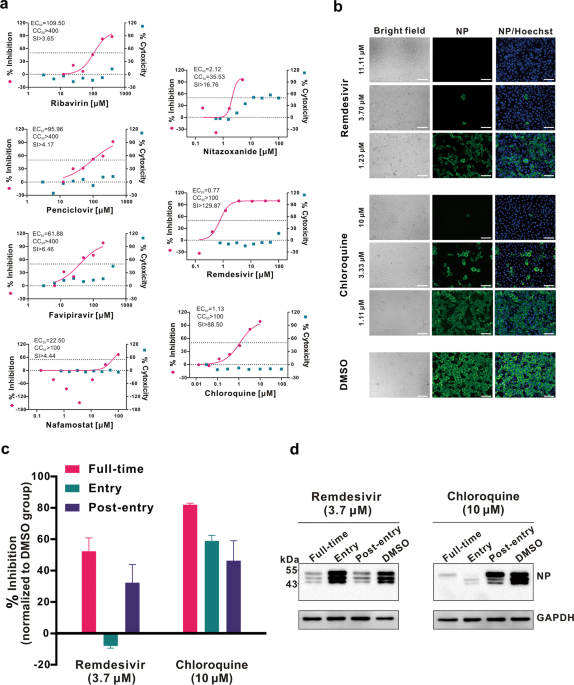
Having said that, I never had a problem with trying HCQ and many other drugs, especially once the paper had been pubished in early February showing both remdesivir and HCQ were effective in vitro against the virus. It was natural to then try them in clinical trials, as they were already tested/approved and available.
The problem I had was with the media blitz on the right after Raoult's now-discredited initial study in March. Elon Musk, the Rigano character, Fox, and then Trump all came out touting HCQ as a "cure" or "gamechanger."
That was grossly inappropriate before anything had even been published and peer-reviewed and Trump's tweet on 3/21, below, was beyond inappropriate for a non-MD/scientist POTUS, especially when Fauci, the medical expert, had already weighed in on 3/20 saying HCQ was unproven, as all we had was anecdotal data.
A POTUS should never be injecting his medical opinion. Period. If he had just kept his mouth shut, like he should have, we likely would have simply looked at the trial results as they came out and concluded it was ineffective and there likely wouldn't have been any controversy.
“HYDROXYCHLOROQUINE & AZITHROMYCIN, taken together, have a real chance to be one of the biggest game changers in the history of medicine; put in use IMMEDIATELY. PEOPLE ARE DYING, MOVE FAST, and GOD BLESS EVERYONE!”
Fauci throws cold water on Trump's declaration that malaria drug chloroquine is a 'game changer'
Infectious disease expert Anthony Fauci throws cold water on Trump's insistence that one drug is a “game changer” in the fight against novel coronavirus.abcnews.go.com
One more point on HCQ which often gets overlooked. HCQ looked good in vitro and then went right to human COVID use/trials, since time was short and it was already shown to be reasonably safe for lupus/malaria. However, a paper in June showed that HCQ had no benefit in either disease progression or prophylaxis for either hamsters or macaques being given HCQ - if this study had been run before any clinical trials, there wouldn't have been any clinical trials run.
COVID-19 Pandemic: Transmissions, Deaths, Treatments, Vaccines, Interventions and More...
 thefederalist.com
thefederalist.com
Yes, I've posted about this one (MK-4482) a few times, since I used to work there and have some knowledge of the compound, as I may end up consulting on this one for them (I retired, but I've been doing some part-time consulting on other projects since then). My gut tells me that the potential markets for antivirals like remdesivir (annoying that that article kept calling it Veklury, a name nobody uses) and MK-4482 might dry up quickly this fall once positive results (and I expect very good positive results) are announced for the various engineered antibody cocktails. However, such success is not a given, so Merck and Gilead will keep plugging away on the antivirals and even if the antibodies are pretty successful, it's possible that a combo with an antiviral would be even better or that an antiviral might be used in cases where antibodies don't work as well.
Interesting. There's more to this than lockdowns. Have noted before, many of the countries with the lowest numbers are island countries. But maybe also, those countries overall are more metabolically healthy?
No lockdown in Taiwan:
What The Rest Of The World Can Learn From Taiwan's On Coronavirus
At this critical period when the coronavirus is amplifying worldwide, it’s clear Taiwan has done something right in its containment measures.
Interesting. There's more to this than lockdowns. Have noted before, many of the countries with the lowest numbers are island countries. But maybe also, those countries overall are more metabolically healthy?
No lockdown in Taiwan:
What The Rest Of The World Can Learn From Taiwan's On Coronavirus
At this critical period when the coronavirus is amplifying worldwide, it’s clear Taiwan has done something right in its containment measures.
Please stop posting twitter news. Nobody takes it seriously.
Please put me on ignore, Karen. You can be reasonable at times, but other times, you are too triggered. If you weren't so triggered by Twitter, you would recognize that 99% of what I post from Twitter references a news article or a journal, but perhaps you can't see that . Twitter, like any other source, when properly used and filtered, provides a wealth of information. You should give it a try.Please stop posting twitter news. Nobody takes it seriously.
Now we know exactly where you are coming from. You are one of them.Speaking of Peru, another country that supposedly uses HCQ with poor results.
That is why I stated in my post that there is more to this than lockdowns. One of the problems with Twitter is that many Tweets want to make an absolute statement. There are no absolutes with Covid-19. Someone had raised your point in reply to the Tweet I posted. It may also be useful to understand what is meant by a "lockdown," as it probably varies quite a bit by country and even region.Worth noting that 40% of homes in Peru don’t have a refrigerator. That’s relevant because it means locking down in name and practice are probably two very different things. If you can’t store food, you’re shopping for it in markets probably almost daily.
The thing is, I am not advocating one viewpoint. Just reading information that is interesting to add to the discussion. Some people can't handle facts or align themselves with a conclusion or a theory if it is associated with the side that they hate.Knightshift...keep being you. We need more voices not less
The thing is, I am not advocating one viewpoint. Just reading information that is interesting to add to the discussion. Some people can't handle facts or align themselves with a conclusion or a theory if it is associated with the side that they hate.