
Pot calling kettle black.
Nope, deflecting doesn't work.
Your post was 100% political, own it.
Pot calling kettle black.
Are you always gloom and doom?true let's forget about the 15,500 dead people too.
Do you math? 13,578 confirmed, plus 1,947 probable.Why are you inflating the numbers?
You don't trust the official numbers by the Govenor?
Are you always let's pretend like the state wasn't devastated to make COVID look like the flu? We all know that was your point of posting that 800 something people are currently in the hospital.Are you always gloom and doom?
LOL "evidence". Thanks for the recap of Maddow's political talking points "Greg".Trash article. the United States = under 5 percent of the world's population but it has around 25 percent of worldwide deaths from Coronavirus. Why? We don't know for sure the answer to that question, but evidence suggests it could be related to policies such as 15 cases soon to be zero, it all just magically disappear, the heat in April will kill it, not allowing any states to test anyone besides those who came back from China, not stopping travel from Europe, not giving China our PPE, and waiting months to use the DPA to order more, saying nothing to worry about it here, it will magically go away, refusing to wear a mask, promoting medicines that do not work, and refusing to take the virus seriously because of an election coming up.
You gonna post the updated Horowitz article about Arizona deaths in here, or has he even lost you? Haven't seen Maddow in years.LOL "evidence". Thanks for the recap of Maddow's political talking points "Greg".
Let's just start with your hypothetical about the widespread testing that would have been done to prevent the NYC metro disaster had the government scientists and health official running the CDC lab not failed. How many test kits would have been manufactured and available in NYC metro in Feb? Do we have any stats on patients reporting chicomvirus symptoms during Feb in NY/NJ/CT? Let's not forget all the health officials including the WHO were saying that asymptomatic people with chicomvirus weren't spreaders so I'm not sure there would've been this widespread testing you assume. We also know that hospitalization case counts inexplicably---to me anyway----can take 2,3 ,4 weeks to even be validated.You consistently post absolute crap about the virus. By far the biggest reason our area had so many more cases and deaths is two-fold as I've said repeatedly: this area had, by far, the most travelers arriving from Europe bringing the virus in Feb/March, which, combined with the utter failure of the Federal Government to provide testing capability (and medical supplies/PPE) left this area flying completely blind into a pandemic with tens of thousands of unknown cases by early March when the first tests were run in NY and NJ and we didn't have more than 1000 tests per day until about mid-March when things started shutting down, during a time we should have had 20,000 tests per day.
Given the very high population and commuting densities in this area, it's no wonder that we then saw the most explosive exponential growth on the planet throughout March into April. That growth is what led to the very high death rates and as I've posted a few times before, NJ has an average % of nursing home/LTC deaths, while NY has one of the best on a % basis. The death rates in the states spiking now will likely be significantly lower than those we saw in the NE US, but that is only due to the ready availability of testing letting them know who's ill, combined with most cases now being in younger people, since older people now know to distance themselves and wear masks (very few were wearing masks in the first wave due to another Administration failure of not having secured enough masks for the general public, while other countries with 1/100th the death rate of the US did), plus improved medical procedures/treatments, which were developed on the guinea pigs in NY/NJ.
Furthermore, that article is horribly wrong on Sweden, too, saying, "Sweden suffered far fewer deaths per capita than several European neighbors that instituted strict lockdowns—including Belgium, Italy, Spain, and the United Kingdom." And he also said, "Indeed, Sweden’s death rate is remarkably close to that of France." Sweden's per capita death rate is 547/1MM - if he (or you) think that's "far fewer" than Italy's 578 (difference is 31), Spain's 608 (difference is 61), or the UK's 658 (difference is 117) and "remarkably close" to France's 460/1MM (difference is 87), you guys need to have your math cards revoked. Yes, Belgium's is 844/1MM, so he got one minor detail correct.
If this guy wants to write an expose, he should write one on why the US has done so badly vs. the countries that have done far, far better, using essentially our playbook, which we ignored.
Is there a new Horowitz article about AZ? Feel free to link "Greg". Sorry you missed the civil conversation RU-05 and I had about that article I linked weeks ago. Did you read any reports back then about 3-4 week delays in reporting hospital counts? Oh, now I see today a report the AZ chicomvirus mutated to an even more infectious strain. Looks like it's time for the adults to discuss. Nap time for "Greg".You gonna post the updated Horowitz article about Arizona deaths in here, or has he even lost you? Haven't seen Maddow in years.
We all told you the deaths there would rise and the hospitalizations were rising due to Corona you posted from Horowitz that it wasn't so bad, and that we didn't know what we were talking about. The state of Arizona admits it's a disaster there now.Is there a new Horowitz article about AZ? Feel free to link "Greg". Sorry you missed the civil conversation RU-05 and I had about that article I linked weeks ago. Did you read any reports back then about 3-4 week delays in reporting hospital counts? Oh, now I see today a report the AZ chicomvirus mutated to an even more infectious strain. Looks like it's time for the adults to discuss. Nap time for "Greg".
https://www.azcentral.com/story/new...oronavirus-strain-more-infectious/5410710002/
Do you math? 13,578 confirmed, plus 1,947 probable.
The AZ dashboard showed differently, and I'll wait for your receipts for any reports at the time warning about 3-4 week delays in hospitals reporting daily case counts. Also show me where I disputed lags in deaths from cases. I bet CuomoDomo and Murph wished they had the "disastrous" stats of AZ's 295 fatality rate vs. over 1,700.We all told you the deaths there would rise and the hospitalizations were rising due to Corona you posted from Horowitz that it wasn't so bad, and that we didn't know what we were talking about. The state of Arizona admits it's a disaster there now.
I think if you are sending your kid to school you are accepting the risk, and at this point people should be aware of what the risks are.Wrong. The flu is an accepted risk by society (and anyone can get a flu shot who wants to prevent the flu), coronavirus is not in that category. Also the chance of a FLU outbreak at school is minimal compared to a Coronavirus outbreak. Why do you think the Senate and the current administration have been desperately trying to get a liability waiver for all reopened businesses. If no one could win in court against them they wouldn't care.
I agree, confirmed is preferable.Let's stick with confirmed.
This isn't a game of horse shoes
Atlanta will open virtual school August 24 and will go back to class 9 weeks later around October 26, one week before the November election. Trump is going to be pissed. I think a significant part of the country will open later than normal in October.I live in Montgomery County, Maryland. Population 1.05M. Median household income $106,054. It is the largest school system in Maryland and 16th largest school system in the country. Announced today that K-12 students will not return to school until November the earliest. I don’t think we will be alone .
I'm not going to re-explain this to you for the 5th or 6th time, since you're clearly incapable of understanding simple math and supply chain logistics - feel free to look up my posts on testing. I'll leave you with this thought though: how was South Korea able to do all this weeks before we were? Maybe read up on that.Let's just start with your hypothetical about the widespread testing that would have been done to prevent the NYC metro disaster had the government scientists and health official running the CDC lab not failed. How many test kits would have been manufactured and available in NYC metro in Feb? Do we have any stats on patients reporting chicomvirus symptoms during Feb in NY/NJ/CT? Let's not forget all the health officials including the WHO were saying that asymptomatic people with chicomvirus weren't spreaders so I'm not sure there would've been this widespread testing you assume. We also know that hospitalization case counts inexplicably---to me anyway----can take 2,3 ,4 weeks to even be validated.
Sure everyone wishes the CDC would not have failed initially, but I'm a skeptical about your premise that the NYC metro disaster could've been mostly avoided if the CDC test was ready as planned. Trump was "flying blind" too when he stopped China travel. Yet NY Dems played it their way promoting mass gatherings in defiance. They should have been more conservative. How did LA County handle their early covid hits better "flying blind"?
Exactly. Just for assurances though I would have no problem signing something to waive my rights to sue just like I did for my son to play little league. You have to weigh the risks, but to your point everyone knows what the risks are at this point.I think if you are sending your kid to school you are accepting the risk, and at this point people should be aware of what the risks are.
Except it is illegal to not send your children to school, and if schools don't provide an online option in addition to in person schooling what choice are you left with?I think if you are sending your kid to school you are accepting the risk, and at this point people should be aware of what the risks are.
As numbers says, your schtick is old. We all knew about the lags. Anyone who has a clue knows. We know you don't. Tell the people of Arizona it's not a disaster right now. Scream Cuomo and Murphy all you want, Arizona had 3 months of advanced notice. I won't be responding further to your posts, as it is clear you just don't get it.The AZ dashboard showed differently, and I'll wait for your receipts for any reports at the time warning about 3-4 week delays in hospitals reporting daily case counts. Also show me where I disputed lags in deaths from cases. I bet CuomoDomo and Murph wished they had the "disastrous" stats of AZ's 295 fatality rate vs. over 1,700.
You have some work to do "Greg". Go!
I'll stick with the reality, how do you explain all the excess deaths? Doctors and coronors have said they believe these people died of Corona. I will listen to the professionals all day everyday.Let's stick with confirmed.
This isn't a game of horse shoes
My kids are grown so I have no dog in this fight but I think about about parents who can't work from home and have elementary school age kids. If the kids don't go back in the fall what will these folks do? Pay for an all day sitter/tutor? Some child care businesses are open but you can't expect child care to help kids with on-line learning. And then there is the additional cost of any option which a lot of folks can't afford. Also, if people are putting their kids in child care, how is that much different than sending them to school?
Homeschool.Except it is illegal to not send your children to school, and if schools don't provide an online option in addition to in person schooling what choice are you left with?
I agree, confirmed is preferable.
And really at this point 13K or 15K does it really matter what the exact total is? We know it's a big ass number.
It's quite possible this will continue to be the case. But other states are ready to have their time in the spotlight.Nursing home mismgmt and keeping the trains and busses running to and from NYC for so long are the two main reasons why NJ has the highest death rate in the country, still, with only NY even close.
And if the parents have to work all day? Homeschool isn't a free for all.Homeschool.
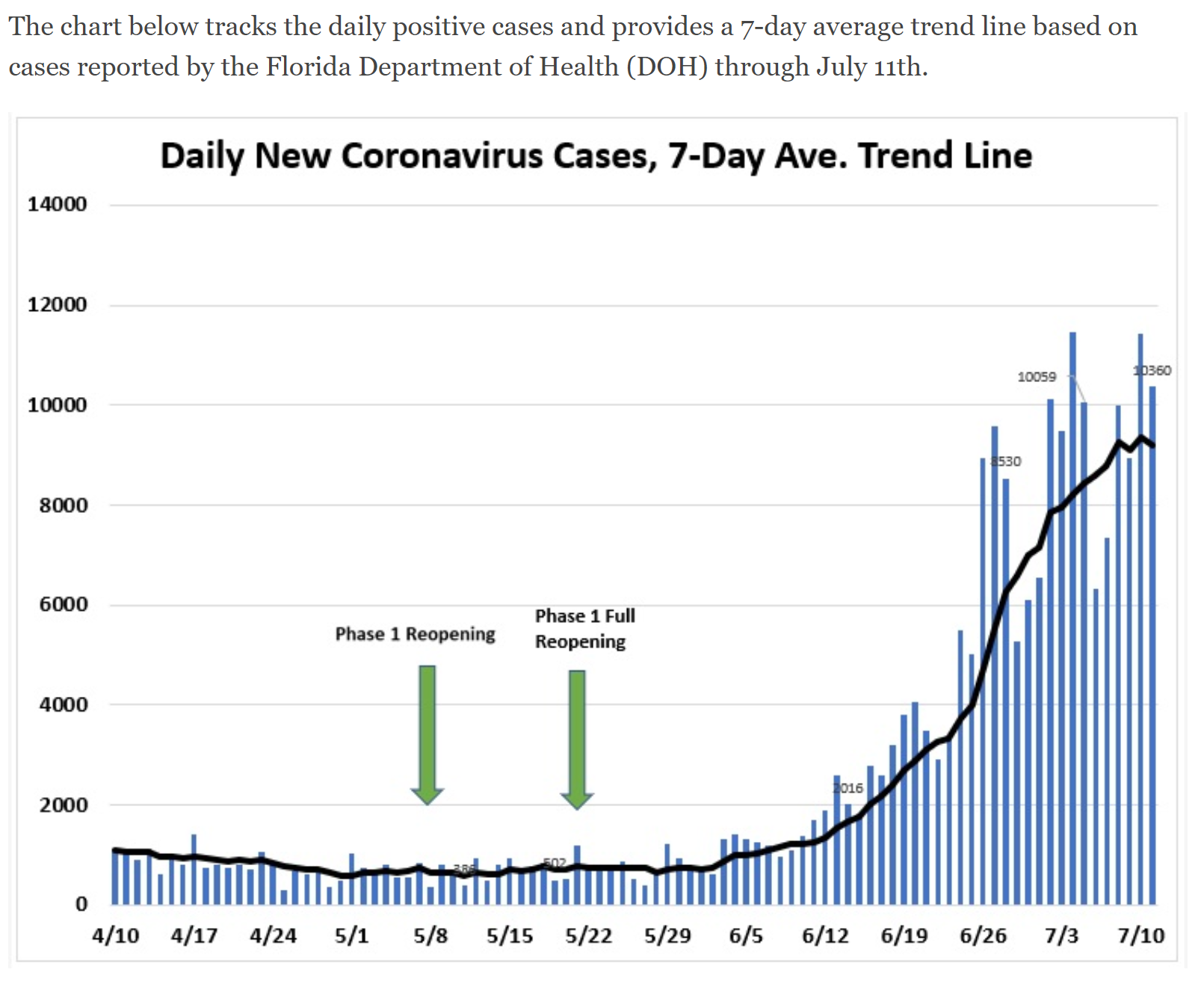
I would argue that a better demarcation is around 6/15, which looks to be close to an inflection point in the case curve. From 6/2 to 6/15 the new cases/day (on a 7-day moving avg) went from 742 to 1774 (about 2.4X), which is certainly an increase, but much less of an increase than from 6/15 to today (1774 to 8434, about 4.8X). I would've expected a modest (1.5-2.0X?) increase in deaths as a response to the initial rise and we only saw deaths go up by maybe 1.3X through now. But that's a minor point, really.
As we and others have been saying, with younger people being infected in FL and cases being caught earlier and improved medical procedures and treatments, deaths, relatively would be expected to be less per capita than they were in March/April. In the attached story, it shows the median age of Florida's cases has dropped from the low 60s to the mid/upper 30s, which is a huge difference and they show the % of cases for each age group to date, but to do any estimating of what the death rates might be would require the age distribution from March-May vs. June, which I haven't seen broken down anywhere. Could probably get it by difference if we had the breakdowns through May, but I'm not that motivated to figure it out - maybe somebody else will.
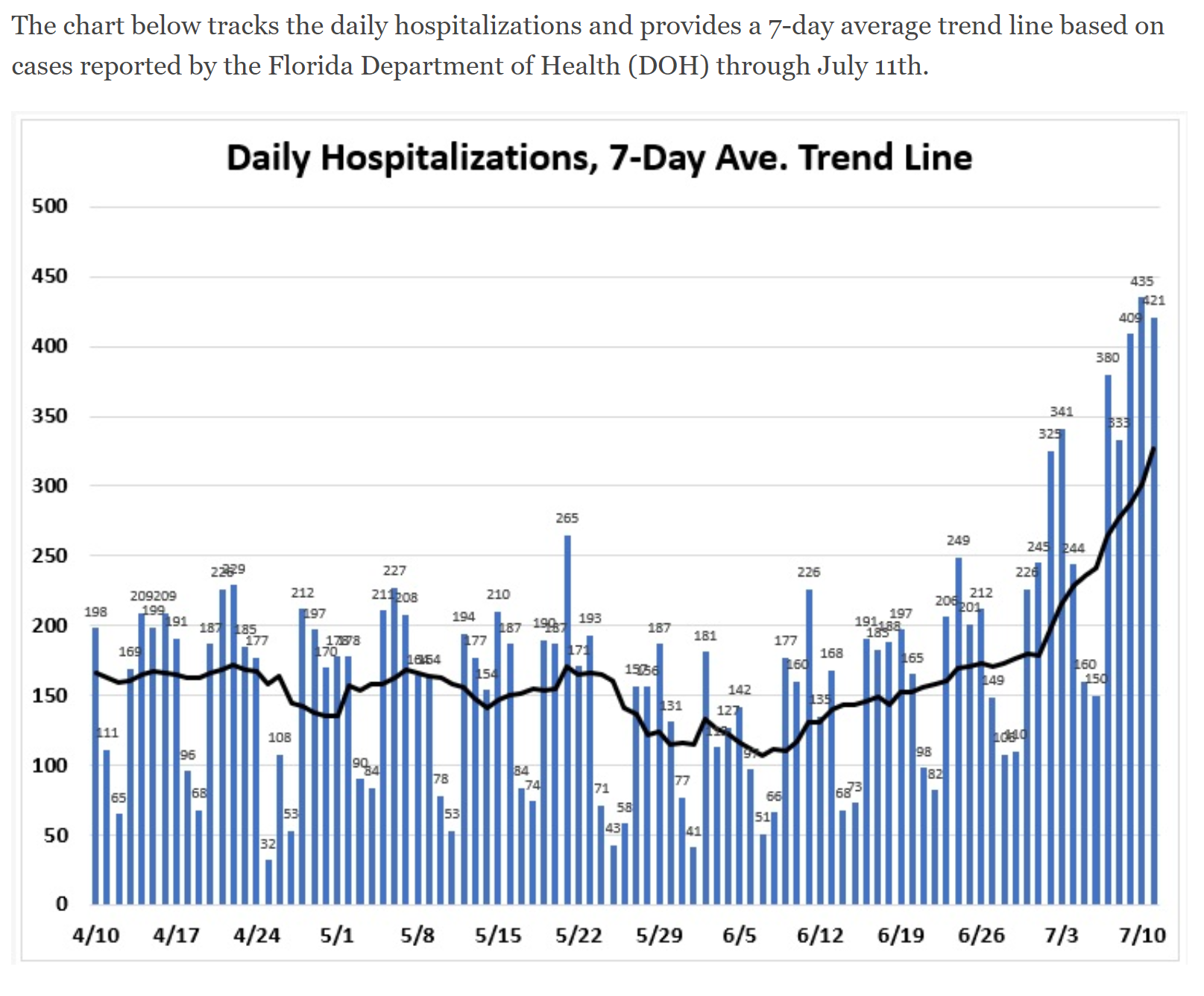
To your point on relative hospitalization rates vs. cases, in NJ, at its peak NJ had about 3600 new cases per day and the peak hospitalization rate ended up being about 400 new ones per day for a ratio of 0.11X. Florida in April had a ratio of roughly 1000 cases/day over a long steady "peak" vs. about 170 new hospitalizations per day for a ratio of about 0.17X, so FL back then had a ~50% higher hospitalization to case rate than NJ. Right now, though, we're seeing a FL peak which should be at least 8000 cases/day and even if they "only" had NJ's 0.11X ratio one would expect 880 hospitalizations per day vs. the ~250/day we're hitting now (0.03X), although hospitalizations surely haven't peaked while cases could be peaking now. Even if hospitalizations doubled from now to a peak of ~500/day, that would still be a ratio of 0.06X, which is only have half of NJ's at the peak. Maybe it'll be lower or higher - no idea.
https://www.nj.gov/health/cd/documents/topics/NCOV/COVID_Confirmed_Case_Summary.pdf
If FL's peak ended up being only half the hospitalizations of NJ's (vs. cases) and death rates per hospitalization were a constant, then FL would likely have half the death rate of NJ's, per capita, but if we factor in improved medical procedures and treatments now vs. 2 months ago, that could cut another 30%(?), leaving FL's peak death rate at only 1/3 of NJ's peak, per capita. My "guesstimate" from 4 days ago was that death rates per capita for the newly peaking states (FL/TX/CA/GA/AZ etc.) would be 1/2-2/3 of those in NY/NJ. FL having only 1/3 of NJ's per capita death rate would be even lower than my 1/2-2/3 guesstimate obviously (which would be fantastic...my dad is 86 and living in Vero), but that depends on FL maintaining the huge case age drop they've seen - in April, their median case age was around 60 and now it's in the mid-30s.
https://rutgers.forums.rivals.com/t...rventions-and-more.198855/page-5#post-4623771
https://www.orlandosentinel.com/cor...0200704-e5lqdwvuhrcb5f2ynyplzprtrq-story.html
A lot depends on FL government and citizens, themselves, keeping the younger, infected people away from the older people, given that FL is the 2nd oldest state in the US (slightly behind Maine, surprisingly), especially those in nursing homes and socially active retirement communities. That might be easier in FL vs. NJ, since many more older people in FL only have contact with other older people (or medical professionals/staff), whereas the elderly in NJ are more likely to be visited by nearby family - this is a bit of a guess, though. Also, in NY/NJ, there was simply no real warning of the exponentially growing outbreak, given the lack of testing until about mid-March, so keeping the old protected from their own families and medical professionals/staff was much harder. The FL/NJ graphics on cases, hospitalizations, and deaths per day are below.
https://www.prb.org/which-us-states-are-the-oldest/
FYI, FL has 21.5MM people and NJ has 8.9MM (2.4X), so given NJ's long death peak of ~300/day, the equivalent rate would be ~720/day in FL and 1/3 of that would be ~240/day (vs. ~45/day now). Well, IMO, we should see the death rate rise substantially by the end of this coming week and we'll know where we end up in several weeks. Let's hope the rates stay lower than expected. TX/AZ/CA/GA et al have also seen a lot more younger people infected than before, but it's really hard to find apples to apples data on ages now vs. April and consistent case and hospitalization data (TX reports total currently hospitalized, while FL reports cumulative ever hospitalized and new hospitalized per day, for example) So for FL and these other states, take these "guesstimates" with a large grain of salt given the inconsistent data at times.
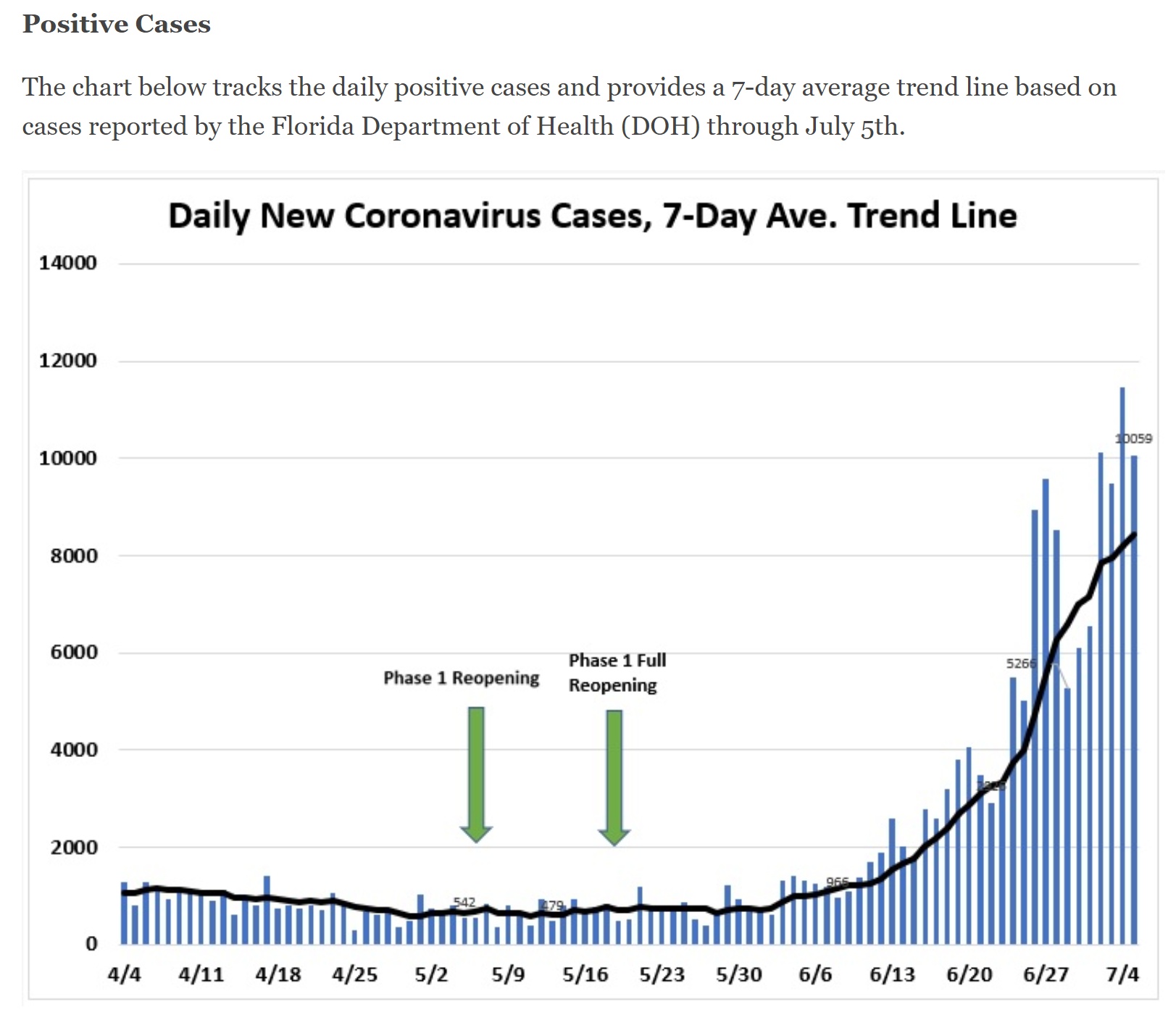
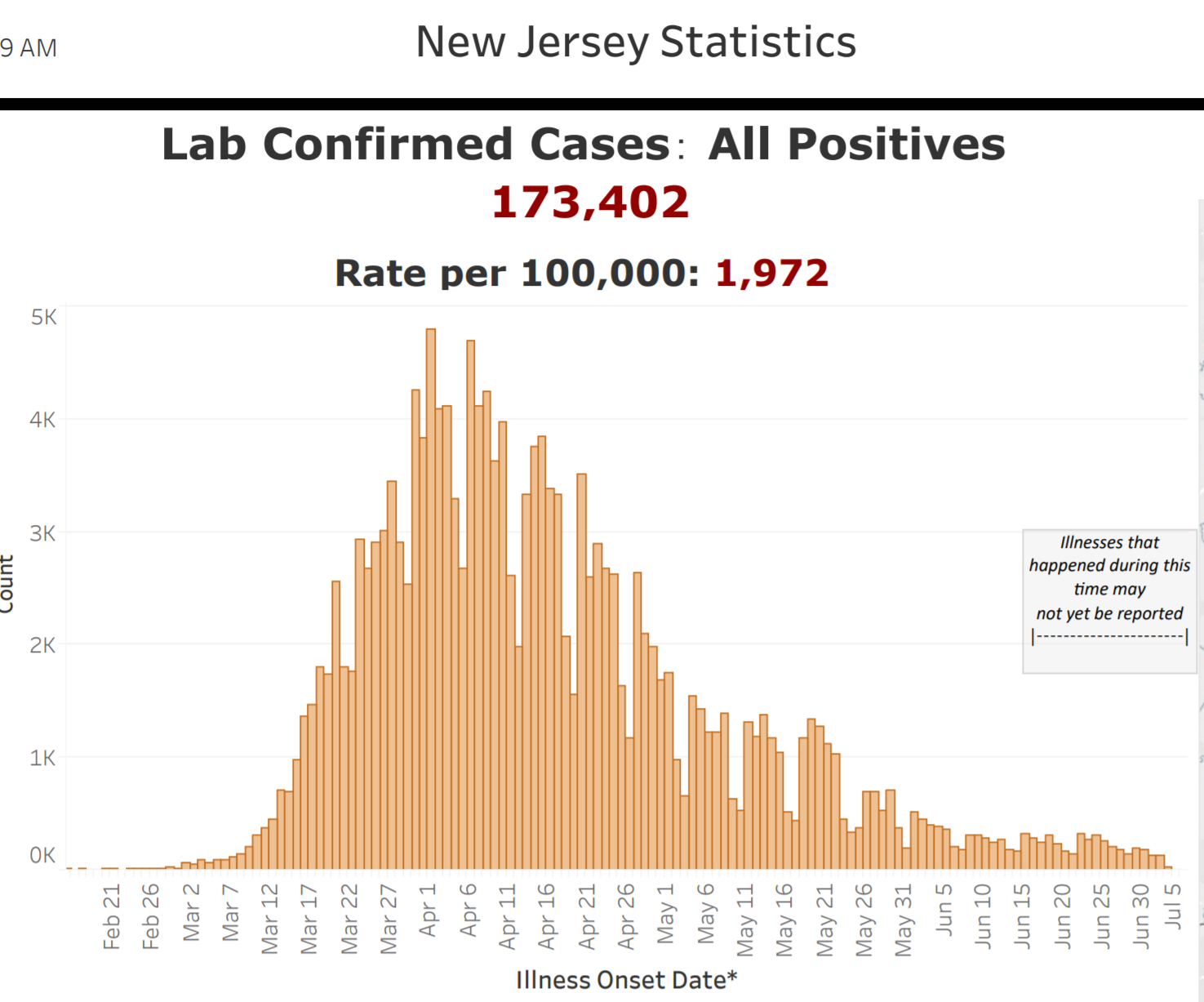
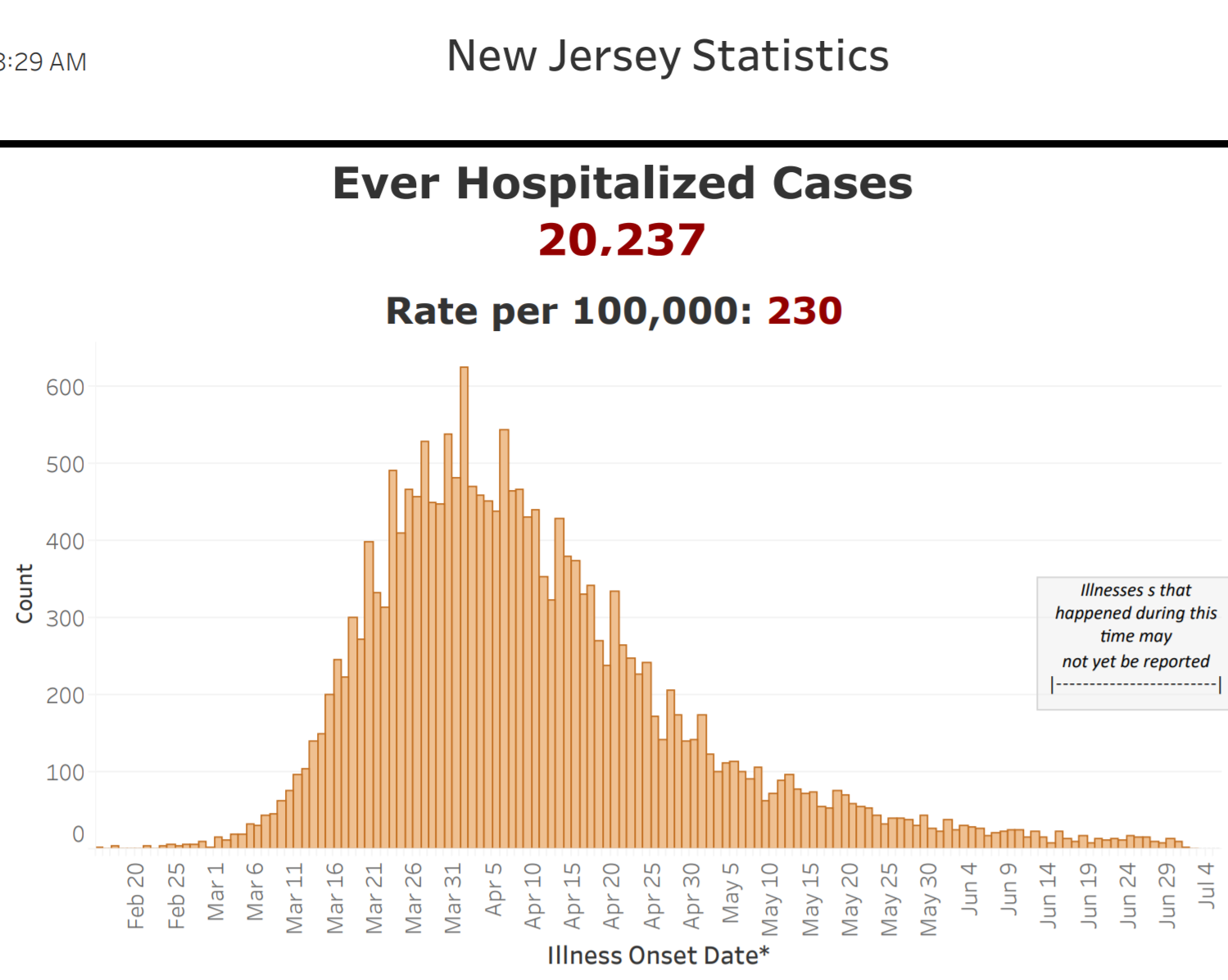
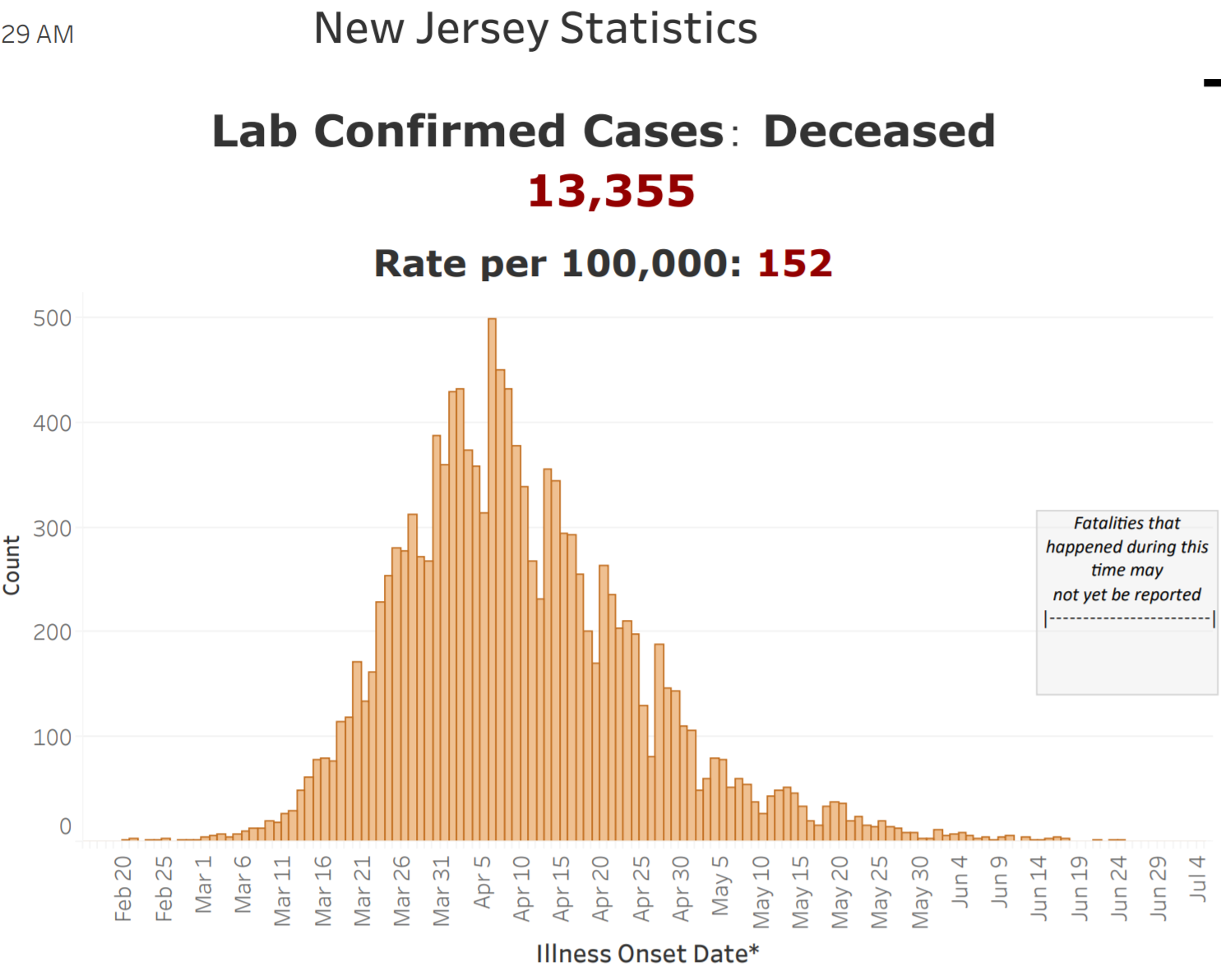
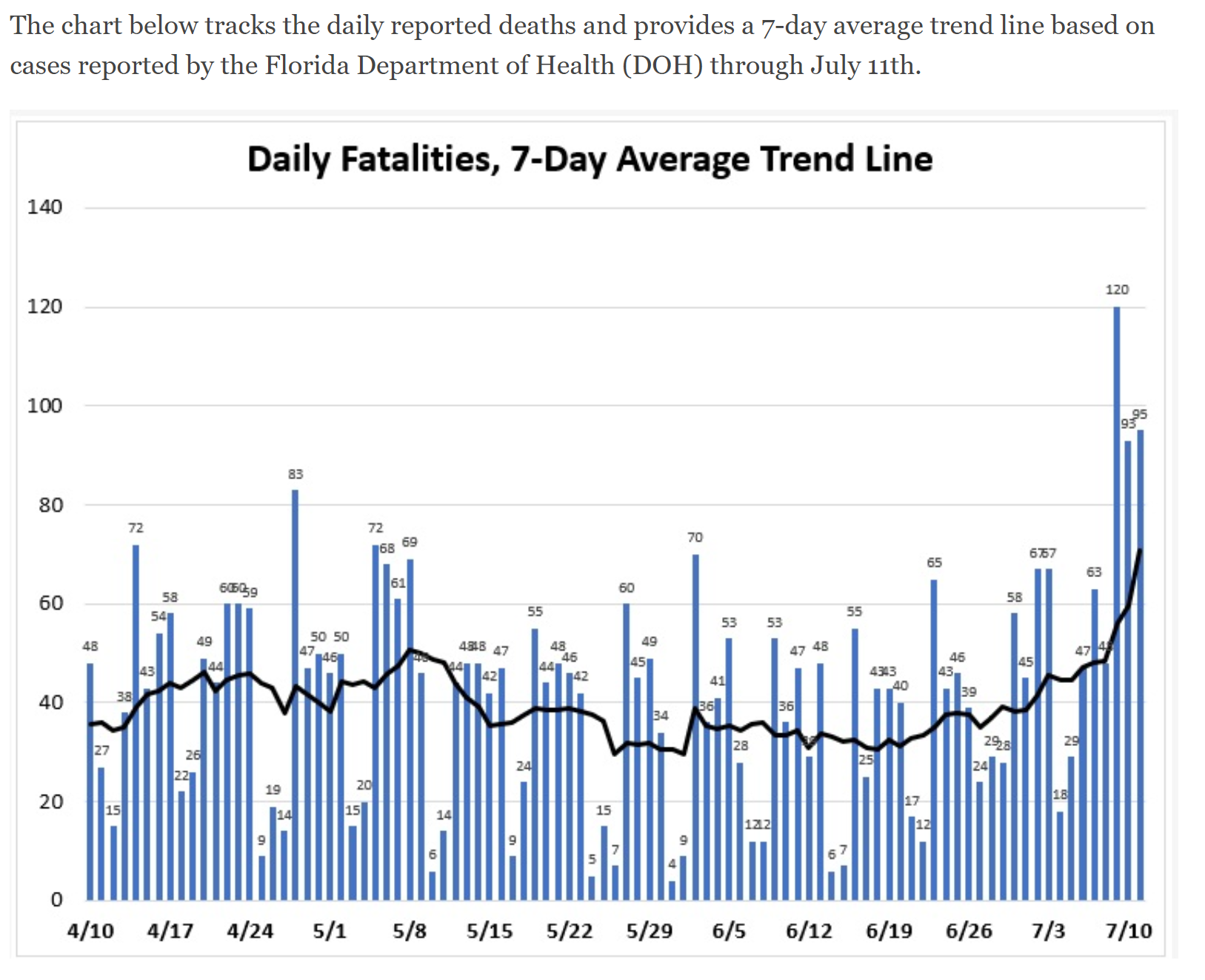
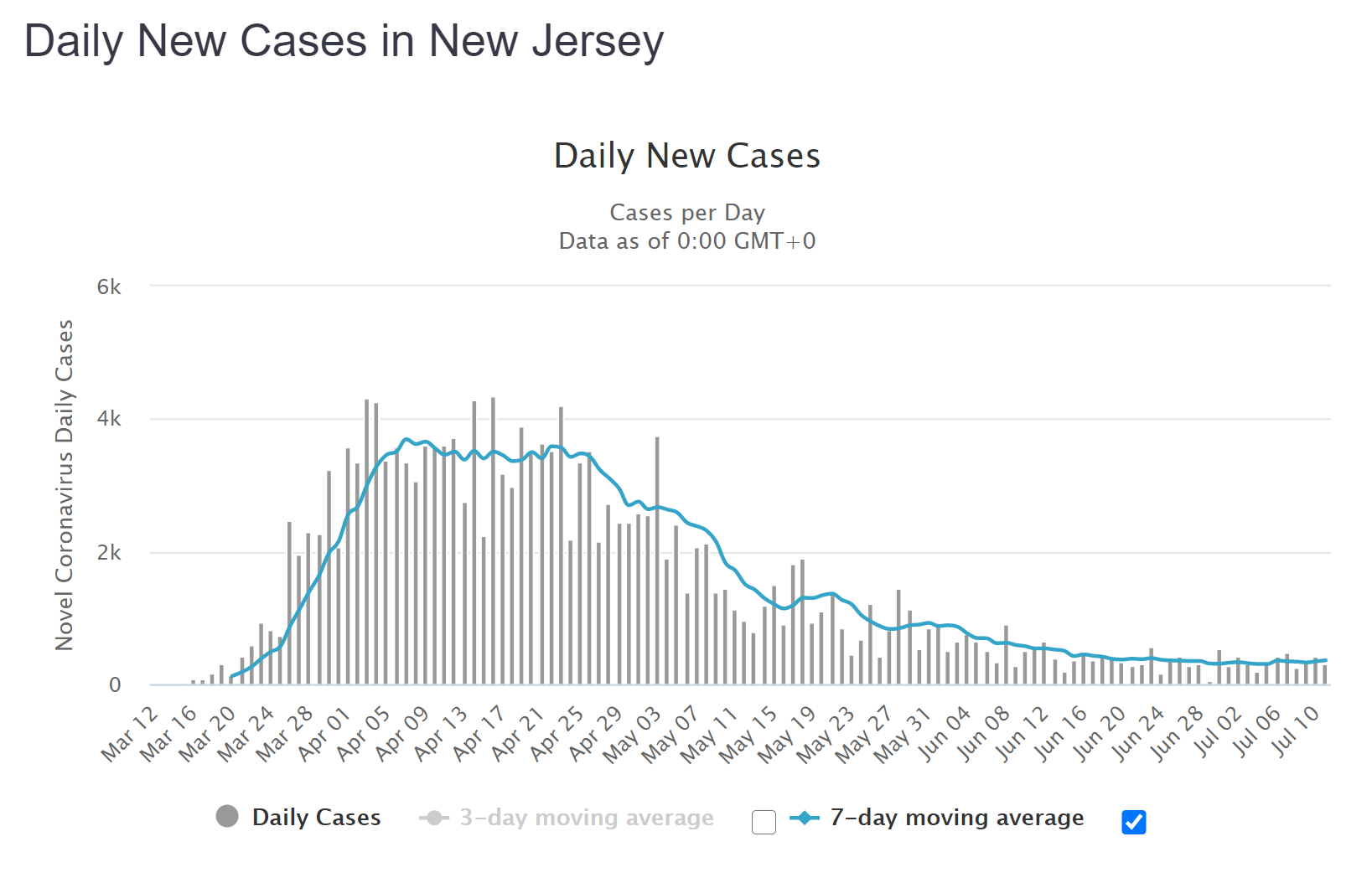
Regarding cases it should be noted that NJ was not catching anywhere near the % of actual infected that Florida now is.Revisiting the Florida vs. New Jersey comparison from Monday. Been guessing the newly spiking states might end up with 1/2-2/3 the death rates per capita as NJ, given the much younger profile of those infected, earlier detection of cases (since we have testing now, but didn't have it available except for the worst cases for most of the exponential growth in NJ), and improved medical procedures and treatments vs. March/April. Let's see how we've progressed in case rates, hospitalization rates and death rates per capita for FL vs. NJ. I decided to use the Worldometers NJ graphics for cases/deaths vs. the NJDOH ones in the quoted post, since these provide 7-day moving averages (7-DMA); these include about 2000 provisional deaths while the NJDOH chart does not, although that doesn't change the analysis much.
First, note that FL has 21.5MM people and NJ has 8.9MM (2.4X), so given NJ's peak case rate of about 3500 cases per day over about a 3-week long plateau on the 7-day moving average, that would translate to a FL peak of 8400 cases per day and FL, right now, has a case rate that's growing more slowly, but is already around 9200 cases/day, which is 2.6X NJ's peak. Nobody knows if FL has peaked (it likely is close) yet or if the peak will be long and sustained like NJ's or a shorter, sharper peak - the answer will obviously affect hospitalizations and deaths.
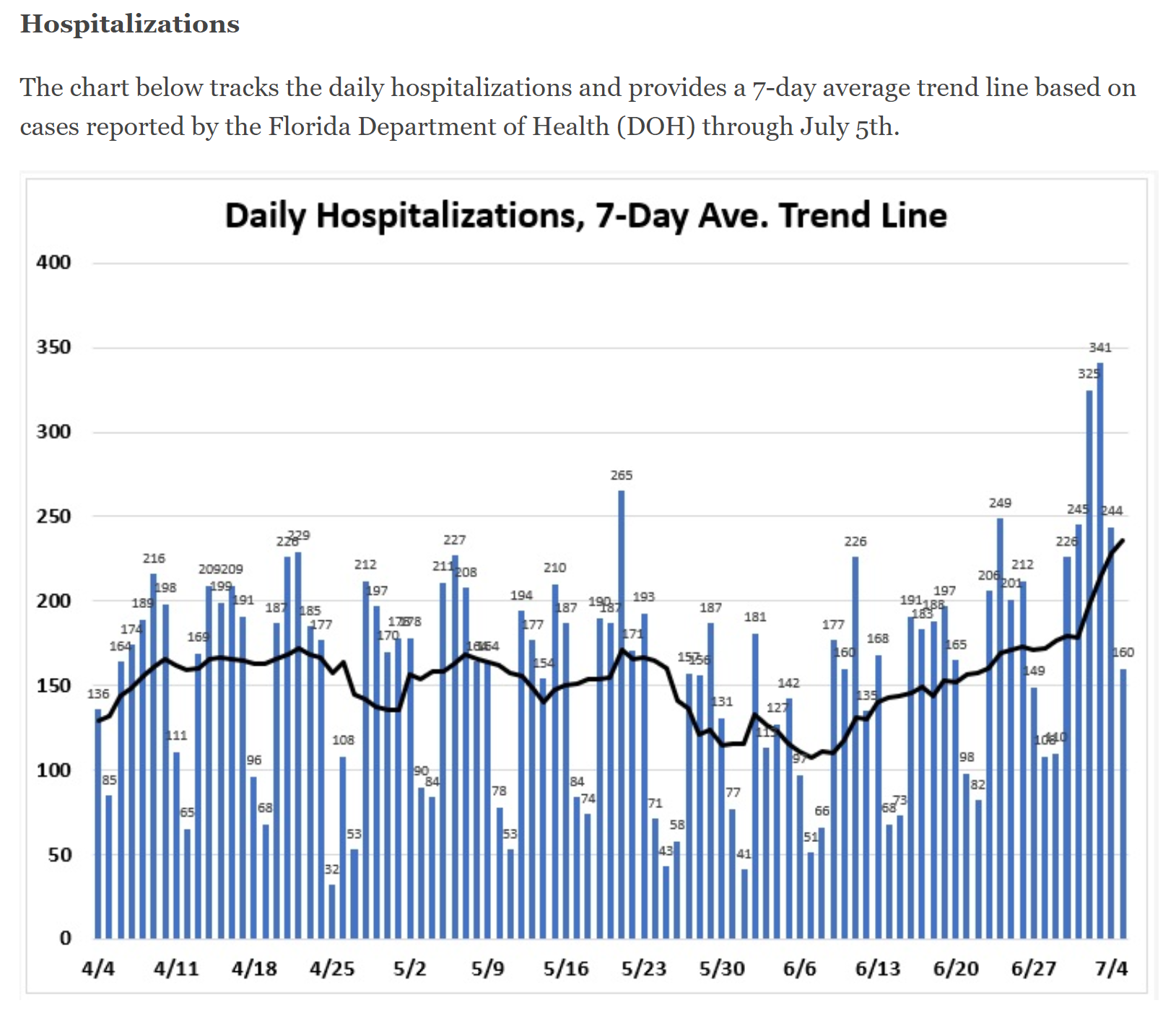
Second, with regard to relative hospitalization rates, at its peak NJ had a daily new hospitalization case rate of about 400-450 new ones per day; Florida would be expected to have a peak 2.4X that if the states had identical outbreaks, which would correspond to around 1000 per day for FL at its peak. Florida's hospitalizations per day are now over 400 per day for the past few days, although their 7-day moving average is still only about 325 per day (it's catching up). So, for now, FL is still at less than half of NJ's per capita hospitalization rate, despite being slightly above NJ's peak case rate, but the FL rate is still climbing rapidly (and their data has been questionable). If I had to guess, FL will at least reach 2/3 of NJ's peak per capita hospitalization rate, which would be about 675 per day. - but that's a WAG.
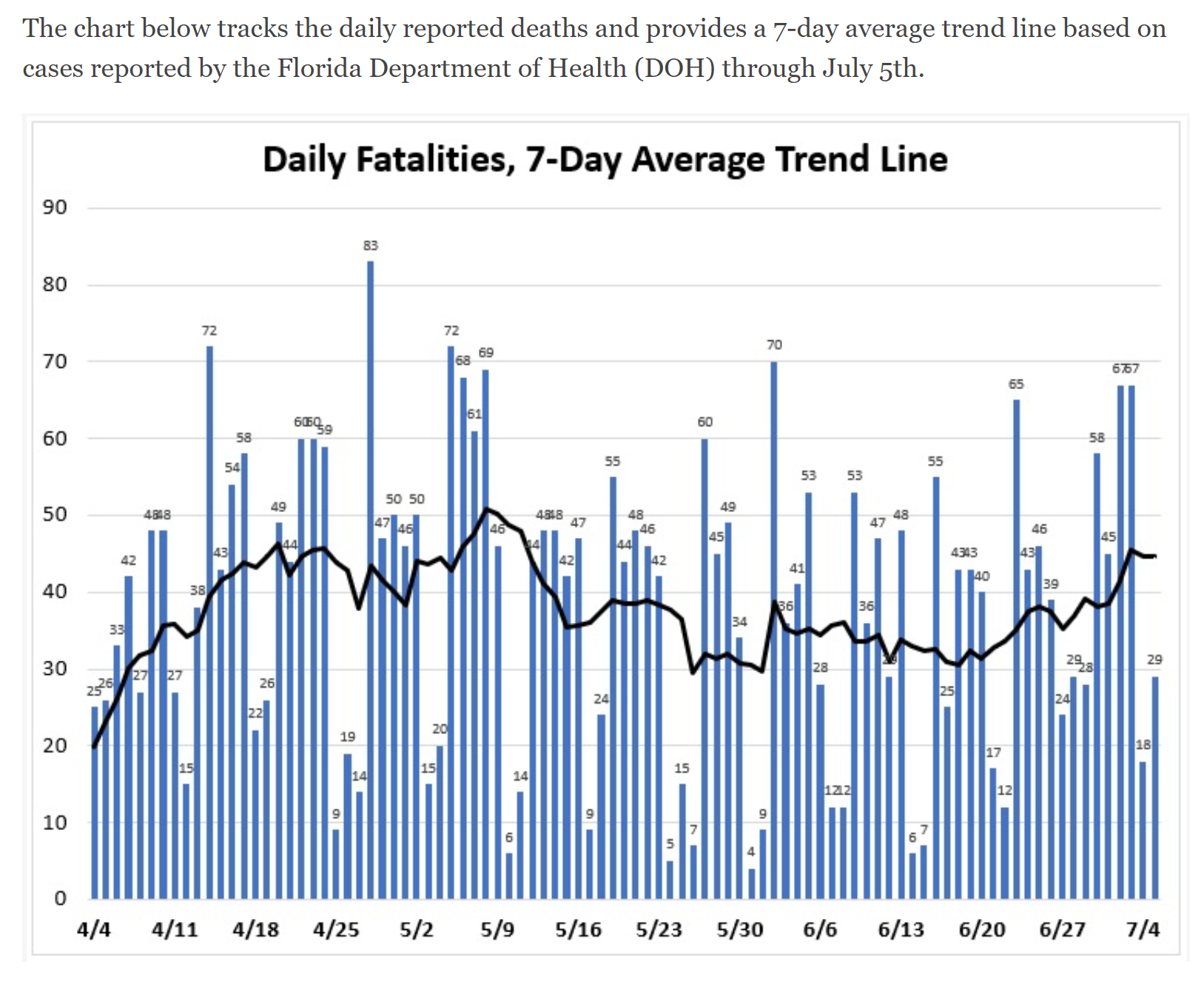
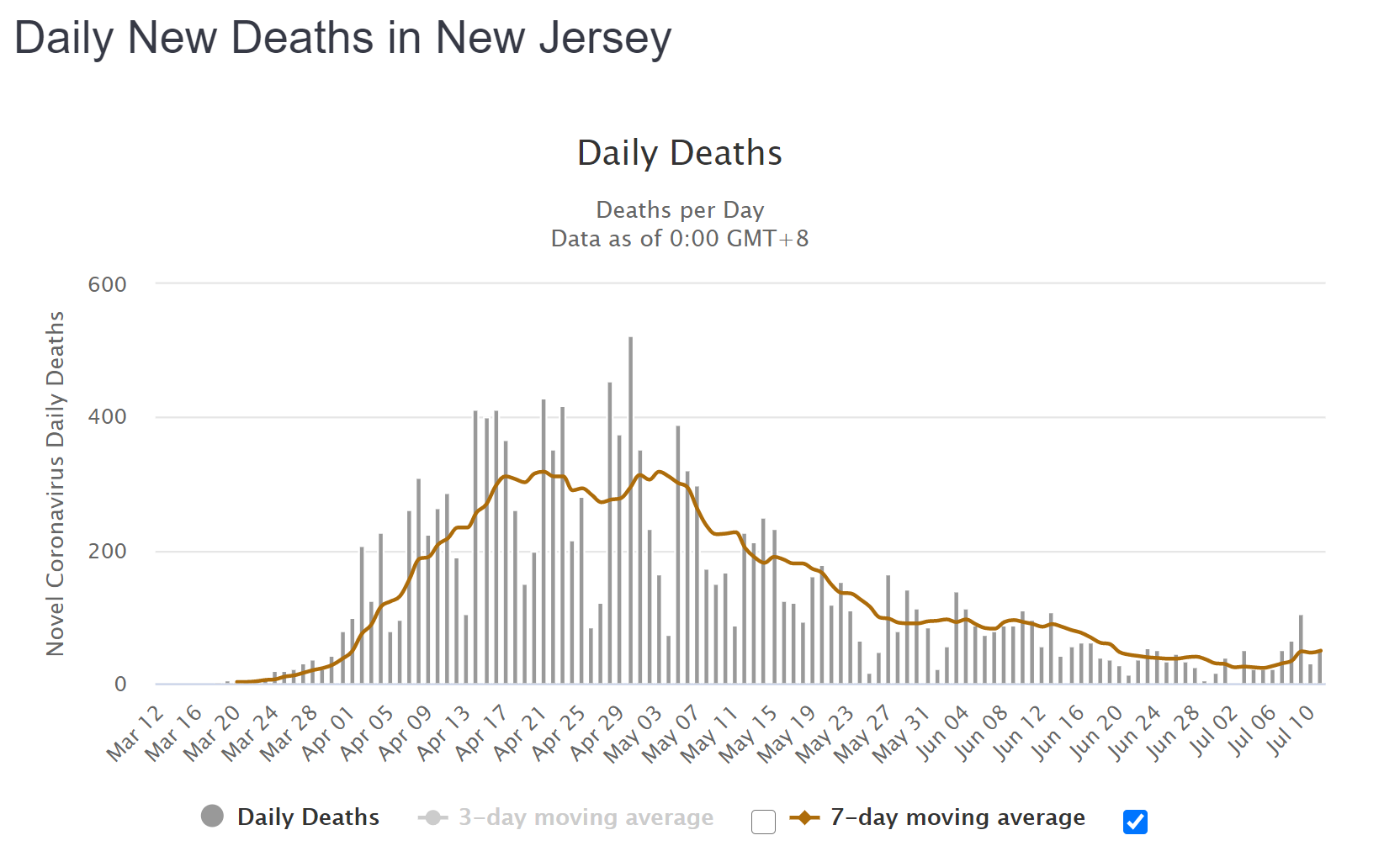
Third, for argument's sake, let's assume FL reaches 2/3 of NJ's per capita peak hospitalization rate (~675/day in FL). Without any improved procedures and treatments, we'd likely expect similar deaths per hospitalizations, assuming patients admitted to hospitals were at a similar seriousness level as they were in NJ. However, as I said last week, I'd guess we might see maybe a 25-30% reduction in mortality rates vs. what we saw in NJ (could be 50% if plasma is working as well as I expect it is and is used enough - but those data aren't available), which would then translate to a FL death rate of about 1/2 what NJ's was per capita - and NJ's peak death rate was about 300/day (7-DMA) for about a 3-week period in mid/late April (equivalent to FL having 720 deaths/day at its peak).
However, if the FL peak death rate of 720/day, were reduced by 1/2, that would be 360/day. FL's death rate is just starting to climb and has averaged ~100/day for the last three days, but the 7-DMA is still only about 70. If FL's death rate curve is similar to NJ's, it'll take roughly 12 more days to go from the inflection point in the growth curve (which was 7/6) to the plateau of the peak 17 days after the inflection point (as seen in NJ) - this involves a huge amount of extrapolation on my part, though, and could easily be significantly off, especially since NJ's case rise was a bit steeper than FL's, so perhaps the death curves will be different too. It would be fantastic if FL's (and other peaking states) had death rates a fair amount lower than we had, but there is one huge assumption in this: much depends on FL maintaining the huge case age drop they've seen - in April, their median case age was around 60 and now it's in the mid-30s - if somehow their elderly population (they're the 2nd oldest state) starts getting seriously infected, then death rates could go up a lot.
I get it could be very difficult. But we are in the midst of a pandemic. There are risks everywhere and everyone should know this by now.And if the parents have to work all day? Homeschool isn't a free for all.
I guess it's the nature of US citizens to collect $$ by suing someone when something bad happens even if it's nobody's fault. Some of the responses on here are mind boggling. We are in a world wide pandemic and people think they can sue if they catch the virus. First off if you catch it there is no way to find out exactly when and where you got it. If you are in a group and someone tests positive later that just means they were the first one to test positive. It doesn't mean that person was the first in the group to have it. Secondly you can't file suit over natural disasters. Unless someone intentionally tries to make ill don't bother to call an ambulance chaser.I get it could be very difficult. But we are in the midst of a pandemic. There are risks everywhere and everyone should know this by now.
If you send your kid to situation where you know there are risks, to then potentially sue afterwards smells like BS to me.
Obviously if there is some gross negligence then that is a different story.
I'm sorry but this type of info gives a lot of false hope. Mostly these types of "announcements" by the company is to increase their stock price or get extra billions from the Goverment to pay for acceleration of production.Go Pharma!
Pfizer CEO Albert Bourla Raises Expectations That the Pharmaceutical Giant Can Deliver a COVID-19 Vaccine by Fall
https://time.com/5864690/pfizer-vaccine-coronavirus/
Pfizer is increasingly confident that its efforts to develop a coronavirus vaccine will be successful. In a July 7 interview with TIME, Pfizer CEO Albert Bourla said he believes that Food and Drug Administration approval could come as soon as October. On the basis of promising results in an early-stage trial released on July 1, Pfizer has dramatically increased the projections for thie number of doses it will produce this year, from tens of millions to 100 million. Bourla alsodisim closed that the company has begun commercial talks with governments around the world about how many doses they will receive.
Bourla is so convinced his $52 billion global pharmaceutical giant is on the right track that he has decided Pfizer will start producing the vaccine before receiving approval from the FDA. It’s a move as risky as it is unorthodox. Pfizer’s vaccine, being developed with its German biotech partner BioNTech, uses a novel genetics-based approach called messenger RNA; Bourla acknowledges that no messenger-RNA vaccine has ever been approved to prevent infectious disease to date.
Pfizer doesn't need to hype anything, this is not a small company begging for attention or a start-up. When one of the biggies publicly express confidence, that's a damn good thing.I'm sorry but this type of info gives a lot of false hope. Mostly these types of "announcements" by the company is to increase their stock price or get extra billions from the Goverment to pay for acceleration of production.
Sorry but very reputable companies are not beneath this. The make drugs to make money. They are seeing the billions being given out to their competitors. You seriously think they don't want their slice of the pie?Pfizer doesn't need to hype anything, this is not a small company begging for attention or a start-up. When one of the biggies publicly express confidence, that's a damn good thing.
You are way too cynical. All you need to know is Pfizer is going to spend $1B to manufacture the vaccine candidate at risk prior to FDA approval. That proves their confidence is real. Read the Q&A.Sorry but very reputable companies are not beneath this. The make drugs to make money. They are seeing the billions being given out to their competitors. You seriously think they don't want their slice of the pie?
Besides since my dad past away from Alzheimer's. 21 years ago I generally pay attention to any news on any advance in finding a cure or dramatically slow it down. Countless times I've read about a new drug or treatment is just around the corner only to never hear of it again. Like malaria, aids, countless others there is no guarantees on a vaccine. To believe and pronouce one at this time is foolish.
So you don't think they want to recover those costs?? Seriously?You are way too cynical. All you need to know is Pfizer is going to spend $1B to manufacture the vaccine candidate at risk prior to FDA approval. That proves their confidence is real. Read the Q&A.
Sorry, this reply makes no sense. Please reread. They are spending $1B to manufacture the vaccine now because they are confident it will be successful. If it is not successful/FDA approved, that investment will be 100% wasted. This financial risk proves their confidence is legit.So you don't think they want to recover those costs?? Seriously?
