
because they haven't been up last 5 weeks lmao.Great news. If NJ cases have been up last 5 weeks, why aren’t hospitalizations?
Colleges
- American Athletic
- Atlantic Coast
- Big 12
- Big East
- Big Ten
- Colonial
- Conference USA
- Independents (FBS)
- Junior College
- Mountain West
- Northeast
- Pac-12
- Patriot League
- Pioneer League
- Southeastern
- Sun Belt
- Army
- Charlotte
- East Carolina
- Florida Atlantic
- Memphis
- Navy
- North Texas
- Rice
- South Florida
- Temple
- Tulane
- Tulsa
- UAB
- UTSA
- Boston College
- California
- Clemson
- Duke
- Florida State
- Georgia Tech
- Louisville
- Miami (FL)
- North Carolina
- North Carolina State
- Pittsburgh
- Southern Methodist
- Stanford
- Syracuse
- Virginia
- Virginia Tech
- Wake Forest
- Arizona
- Arizona State
- Baylor
- Brigham Young
- Cincinnati
- Colorado
- Houston
- Iowa State
- Kansas
- Kansas State
- Oklahoma State
- TCU
- Texas Tech
- UCF
- Utah
- West Virginia
- Illinois
- Indiana
- Iowa
- Maryland
- Michigan
- Michigan State
- Minnesota
- Nebraska
- Northwestern
- Ohio State
- Oregon
- Penn State
- Purdue
- Rutgers
- UCLA
- USC
- Washington
- Wisconsin
High Schools
- Illinois HS Sports
- Indiana HS Sports
- Iowa HS Sports
- Kansas HS Sports
- Michigan HS Sports
- Minnesota HS Sports
- Missouri HS Sports
- Nebraska HS Sports
- Oklahoma HS Sports
- Texas HS Hoops
- Texas HS Sports
- Wisconsin HS Sports
- Cincinnati HS Sports
- Delaware
- Maryland HS Sports
- New Jersey HS Hoops
- New Jersey HS Sports
- NYC HS Hoops
- Ohio HS Sports
- Pennsylvania HS Sports
- Virginia HS Sports
- West Virginia HS Sports
ADVERTISEMENT
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
COVID-19 Pandemic: Transmissions, Deaths, Treatments, Vaccines, Interventions and More...
- Thread starter Richie O
- Start date
- Status
- Not open for further replies.
No it's not keep up your lies though.That icus are full in Texas is fake news
TX and FL have lower fatality rates vs. CA , AZ a tad higher (+0.2%) according to the current RCP tracker. TX, AZ and FL are 100% in the sunbelt vs around 60% for CA. As we know San Fran locked down early after analyzing their chicomvirus infection models, unlike NYC, helping to control the spread for CA statewide. LA County is seeing the major spikes in CA, so I guess it's all those R's in LA County not wearing masks.
Your unscientific political spin is such a joke.

https://www.realclearpolitics.com/coronavirus/country/united-states/
I've been talking about death rates in wave 2 for several weeks (which is why you brought up the summer heat/AC/indoors angle) and have posted numerous comparisons of them for FL/TX/CA/AZ and California's current death rate, per capita, is 1/2 to 1/6 the death rates, per capita, in these other states, as per my post from last Tuesday (and that gap has widened a bit since last week). So why you'd bring in overall deaths per capita is beyond me.
And if you're going to focus on overall pandemic death rates, at least get the data right. You said, "TX and FL have lower fatality rates vs. CA , AZ a tad higher (+0.2%) according to the current RCP tracker." Below are the fatality rates per 1MM in that tracker and it shows that TX is about 20% lower than CA, FL is 29% greater, and AZ has more than 2X the death rate of CA, so you got one of three right. The fact that you can be so far off from reality in the simple task of reading numbers from a table is consistent with your numerous other misinterpretations of data (e.g., posting misleading info from Horowitz) why you get no respect on this board.
FL death rate = 276/1MM
TX death rate = 178/1MM
AZ death rate = 453/1MM
CA death rate = 214/1MM
Summary:
Details - Cases
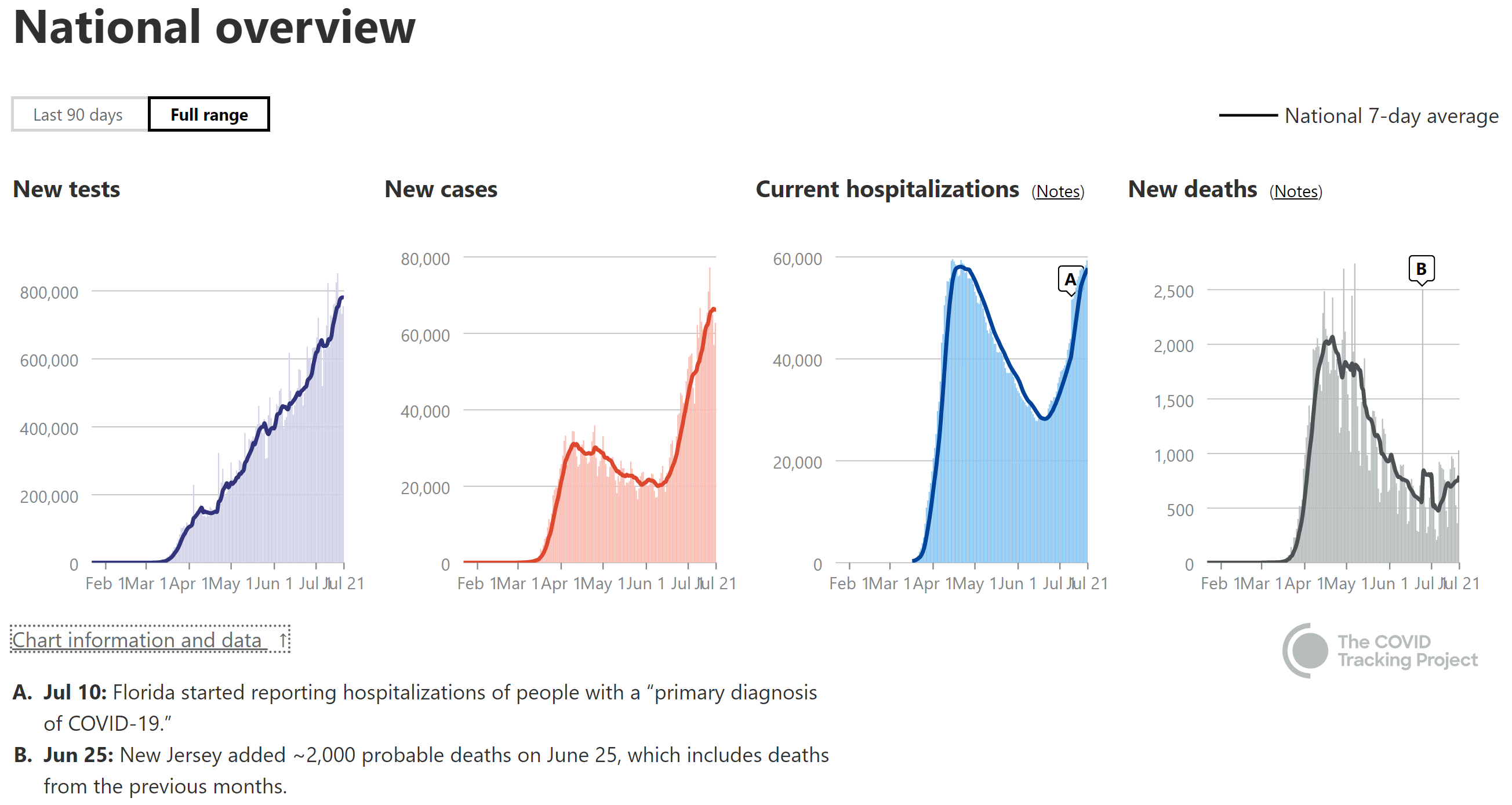
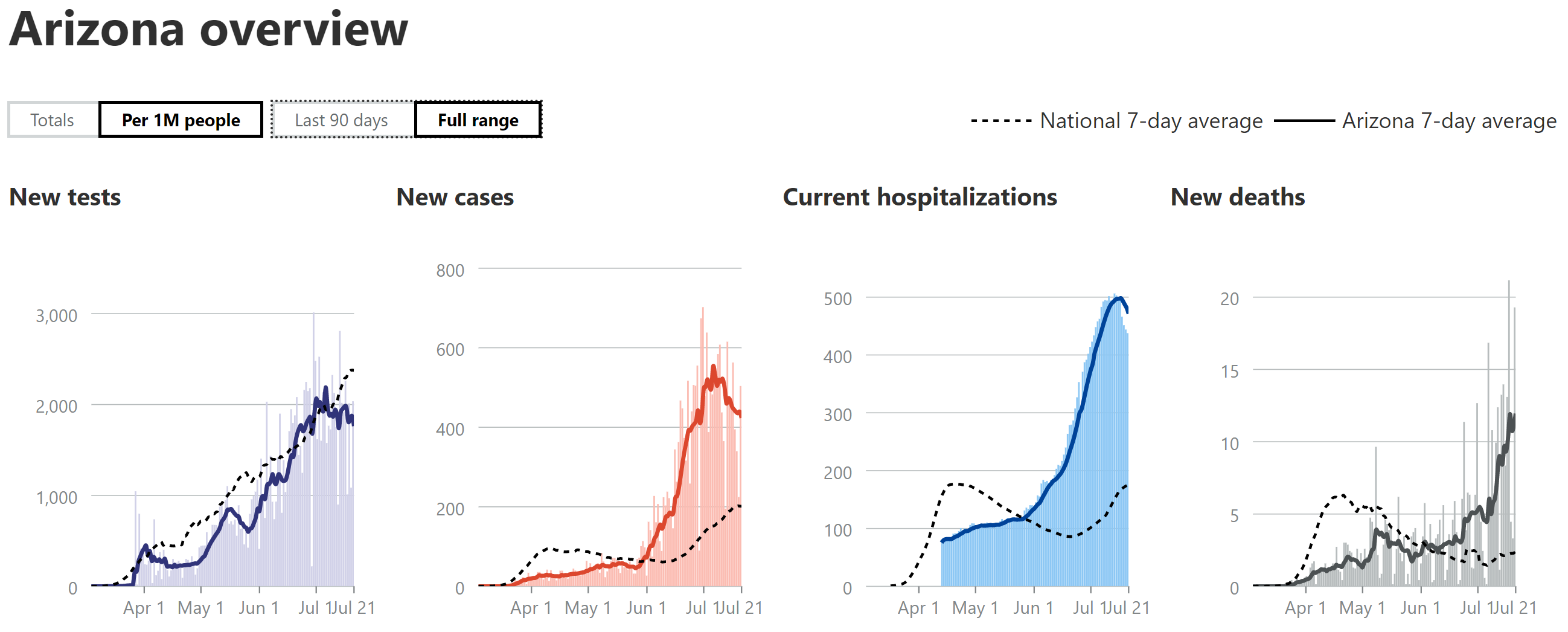
- Nationally, cases are peaking at ~2X vs. the first wave, while hospitalizations haven't quite peaked, but will likely be a bit more than half of what they were in the first wave (per capita). Deaths are up 60% from their early July low and climbing steadily, but are only 35-40% of the April peak.
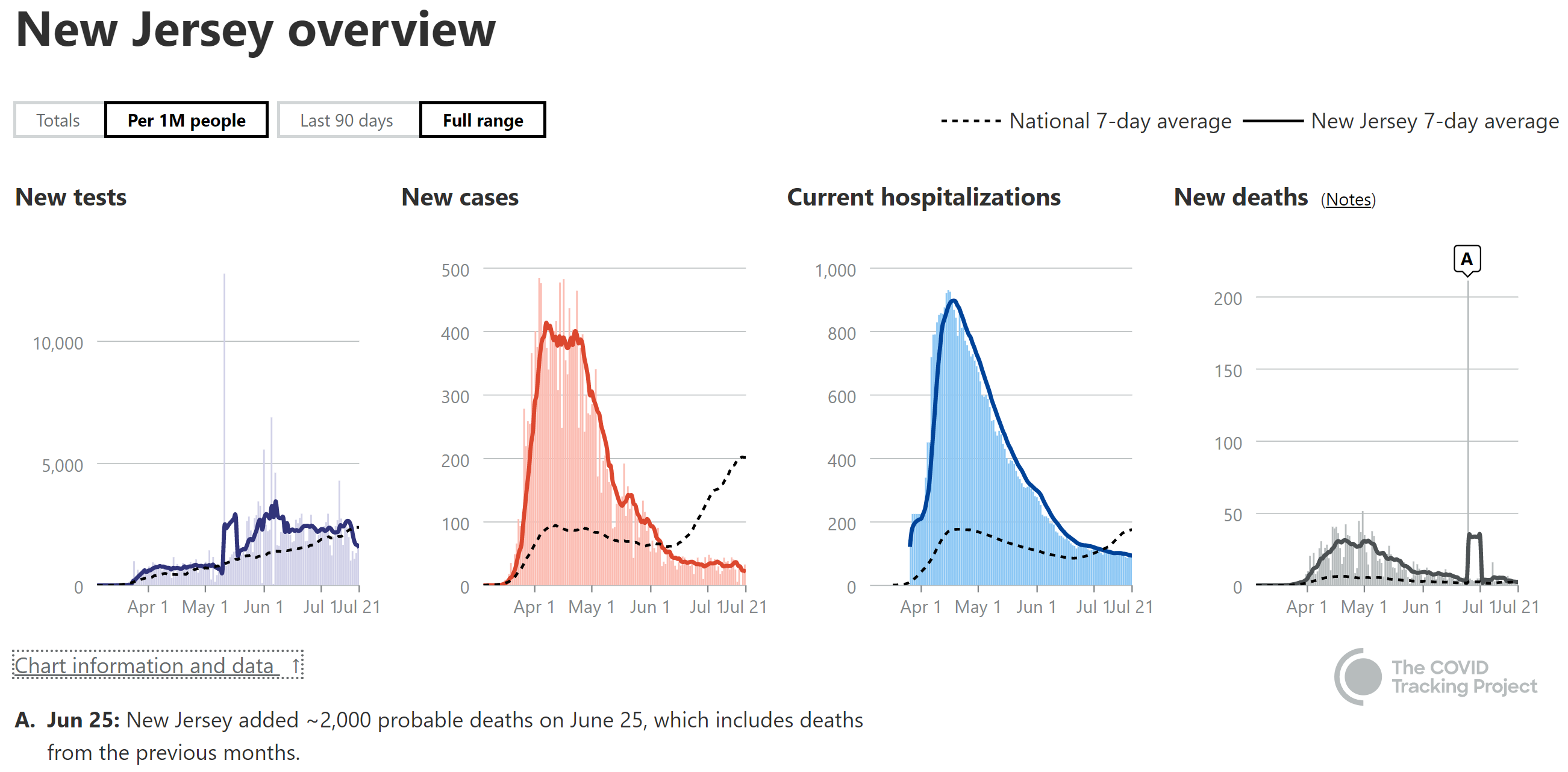
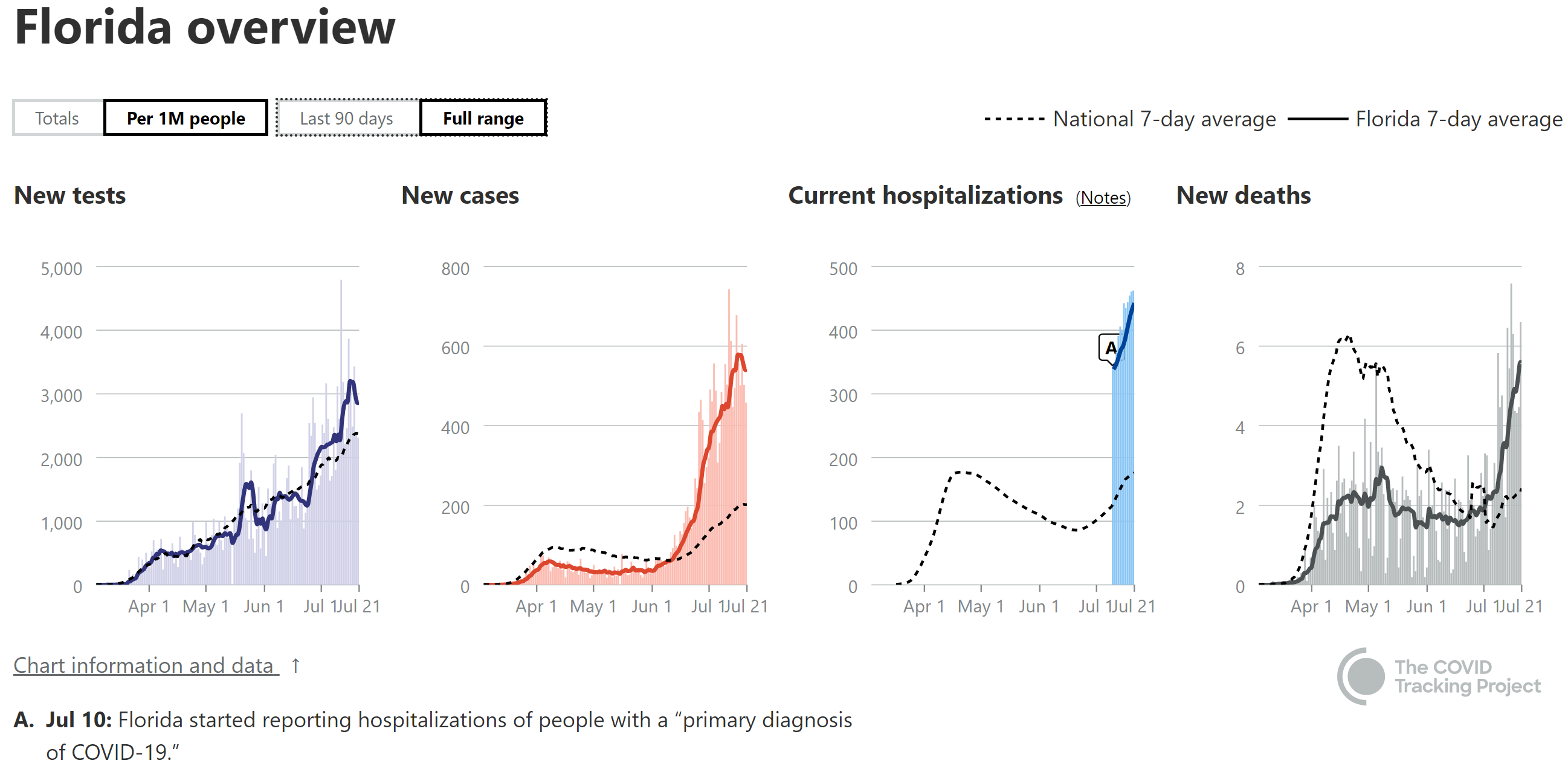
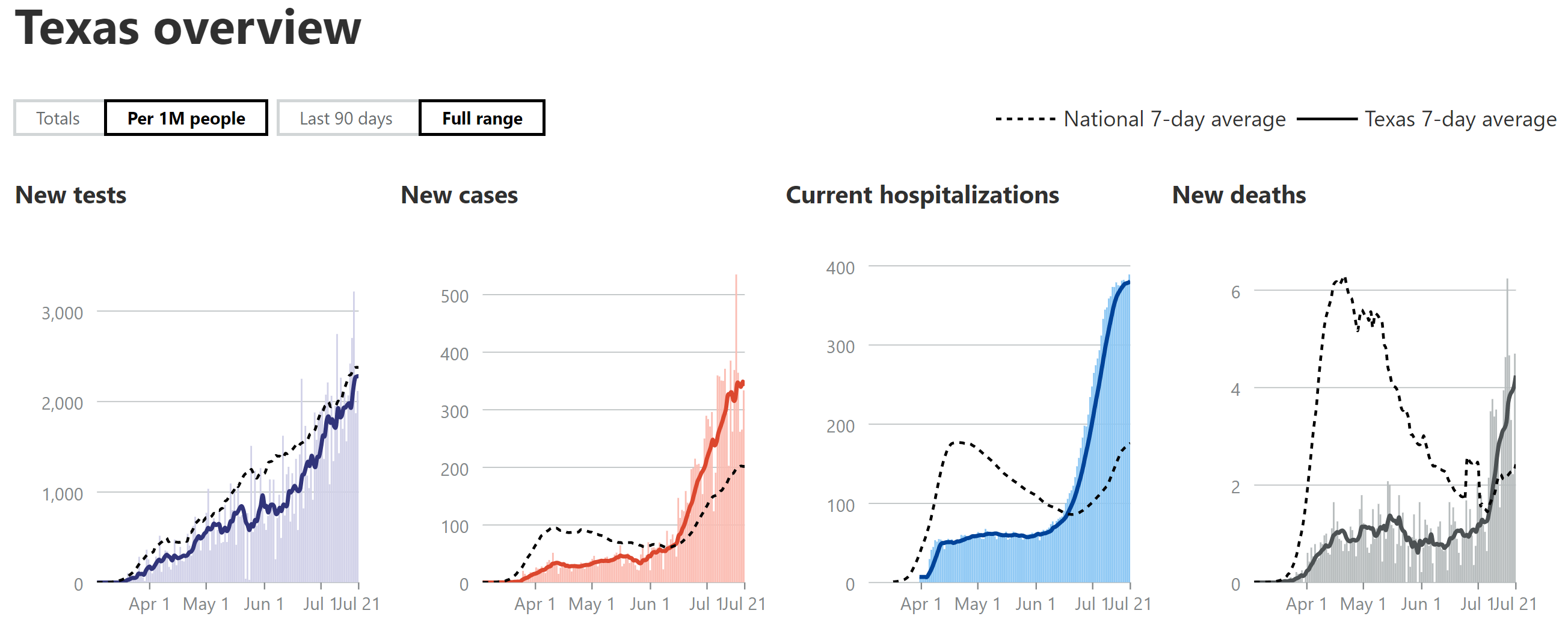
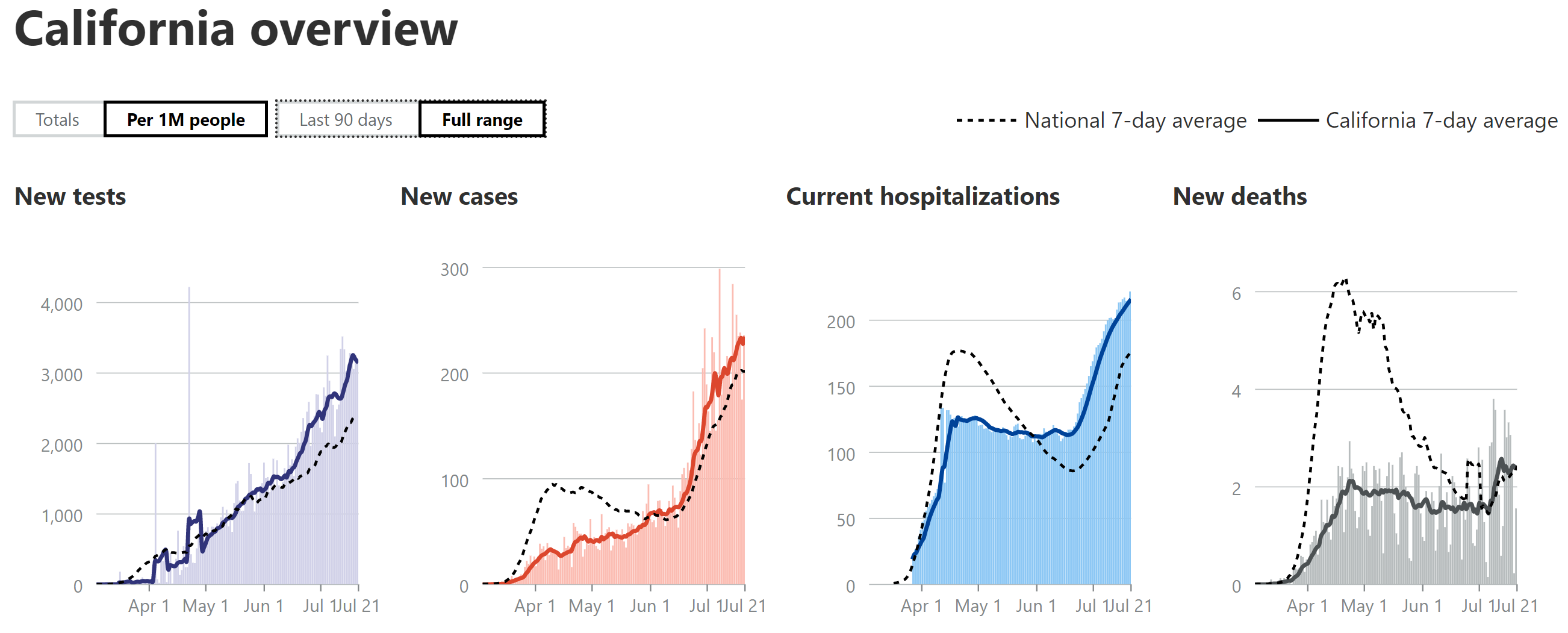
- Cases have peaked (AZ) or are likely peaking (FL/TX/CA) at levels at or above NJ's peak case levels per 1MM people (per capita basis), except for CA, which is well below NJ's peak.
- AZ's hospitalizations peaked at ~55% of NJ's (per 1MM) and FL/TX will likely peak in that region (they haven't peaked yet, though), while CA will likely peak well below that, at maybe 25% of NJ's peak; these reductions vs. NJ are likely due to the much younger age of those infected in this wave.
- We still don't know where death peaks will end up but my guesstimate has been 1/3-2/3 of the peaks of NY/NJ, partly due to the younger age of those infected (as above) and partly due to improved treatments and procedures. AZ is already at 35-40% of NJ's peak and deaths there might be starting to peak, but not in the other states yet. FL/TX seem likely to reach 1/3 of NJ's peak level, but CA will likely not be more than 15% of NJ's peak.
Updating this post a week later and will try to do so weekly for awhile, as weekly as likely infrequent enough to not be fooled by 1-2 day deviations that aren't that relevant (like the usual weekend dips), but frequent enough to see changes occurring. Let's look at cases first, starting with the national picture, where total cases seem to be just reaching a peak around 65-67K cases per day on a 7-day moving average (all the data are on that basis in the charts below), which is about twice what the peak in the first wave was (around 31-32K cases/day).
The "good" news is Arizona has likely peaked in cases and started to decline a bit, although it's too early to call it a real decline, yet, IMO, while Florida, Texas, and California are all nearing or possibly at their peaks (I think, judging by the shape of the 7-day curves). Many other states could be discussed, but these seemed relevant, as FL/TX/CA are the three most populous states and they're peaking and AZ peaked a bit earlier and has a similar population as NJ, which I'm including as a comparison from the worst of the first wave. It should be noted that AZ peaked about 20% above NJ's peak, FL is peaking around 40% above NJ's peak, TX is near NJ's peak, and CA is only at about 60% of NJ's peak (I'm also using per capita data for all the graphs, so they're "apples to apples" comparisons).
Details - Hospitalizations
With regard to hospitalizations, on a national level, hospitalizations are still growing, but not as fast as they were (they only lag cases by a week or so) and they're looking to probably be only a bit above what they were in the first wave, despite there likely being twice as many cases. This was expected a few weeks ago, when it became clear that there was a much younger average age of those infected in most states in this current wave (vs. wave 1) and the hospitalization rates in AZ (which had a 1-2 week earlier outbreak than FL/TX/CA) were tracking at about half the rate of NJ's. Note that if COVID were as deadly as it was in the first wave (it's thought to be) one would expect eventual death peaks to mirror relative hospitalization rates, i.e., if a state peaks at 50% of NJ's peak hospitalization rate, one would expect deaths to be around 50%, also (assuming no improved treatments/procedures).
Looking at states, AZ has now peaked at about 55% of NJ's hospitalization rate, i.e., about 500 per 1MM vs. NJ's 900 per 1MM (all per capita). FL hasn't peaked yet and is at about half of NJ's peak rate, while TX might be starting to peak at just below half of NJ's rate (too early to call yet), and CA is close to peaking and is only at about 25% of NJ's peak. It's not surprising that CA's case and hospitalization numbers (and likely deaths) are not as bad as the other three states in this comparison, as CA reopened later and after having achieved better reopening metrics, plus CA made masking mandatory on 6/18, just as cases were starting to rise significantly, while the other three states didn't start issuing mask requirements until later and they're not nearly as strong as California's.
Details - Deaths
With respect to deaths, on a national level, they've jumped about 60% from the low in early July and are now up around 830/day on a 7-day moving average, which is about 35-40% of the death rate at its peak in April. Note that the 4 states (FL/TX/CA/AZ) I've been discussing account for about half of that death toll per day, which also means that there are many other states with less people, many of which are also spiking in cases, hospitalizations and deaths. We still don't know where death peaks for these states will end up (or total deaths, since that will also depend on whether a peak is sharp or a plateau and long decline, like NY/NJ had), but my guesstimate has been 1/3-2/3 of the peaks of NY/NJ, partly due to the younger age of those infected (as above) and partly due to improved pharmaceutical treatments (such as remdesivir, dexamethasone, tocilimuzab and convalescent plasma) and improved medical procedures.
With regard to specific states, AZ is already at 35-40% of NJ's peak and deaths there might be starting to peak, although it's too early to make that call yet - they've had several individual spikes that were at 50-60% of NJ's peak, so I think that 50-60% is possible to reach with the 7-day moving average. FL/TX/CA have not peaked yet and FL/TX, in particular appear to still be climbing rapidly, with FL currently at about 20% of NJ's peak and TX currently at almost 15% of NJ's peak, so FL/TX seem likely to reach at least 1/3 of NJ's peak level (largely based on comparison to AZ) and maybe more. However, CA likely won't reach more than 15% of the NY/NJ peak given the lower hospitalization rates.
Keep in mind that all of these are educated guesses and a big wild card is assuming cases don't go way up amongst the elderly from here on out - they already are increasing in FL and if that continues and also occurs in the other states, these states could easily reach or exceed the upper end of my estimated range of 2/3 the level of NJ's deaths. Hope people find these to be informative - please let me know if any obvious errors (hard to keep all the #'s straight, lol).
https://covidtracking.com/data#chart-annotations

Does anyone know if there is an easy rapid test that can be done at home or at the entrance of a venue? I feel like we should have that by now.
Sobering. We are losing to an enemy that can be defeated. Not easily defeated, but it can be done.
65M people live in France. 21M live in Florida.

Isn't Florida at a different stage than France is?
Not so fast ....https://apple.news/AqmeJ_z7ZQUG8K9uIRHw9dw
I could see training a new employee to be a problem
Isn't Florida at a different stage than France is?
Why?
And I'll answer my own question. France is at a different stage because they went hard lockdown from March-May. Once/week shopping, no BS mask policy, fines for not social distancing. And that chart is the result. I am open to hearing why their "loss of Freedom" wasn't worth it.
In the long run.. the very long run.. I think freshwater is everything. We really could use a national pipeline system to move water from region to region as we often have droughts one place and floods in another. Costs, of course, would be ridiculous.. but we have had times where we thought about investing in infrastructure.. we could couple an effort like that alongside highspeed rail, new electric distribution system, green energy.. etc. We could even build new towns along the way to accommodate social distancing for the long-haul.
Ahhh the economy.. I am quite surprised it is not worse than it is already. Guess people and the guvhmint bin doin okay so fars. Buy Murphy wants to borrow $9.9B.. and he is likely not an exception.. it is all troubling. We really need a return to the old normal.. 2X or even 3X the usual flu deaths doesn't seem like its worth total destruction of the economy to avoid. But maybe it is. Maybe if we went to the old normal it would be 10X the usual annual flu deaths. I don't know.
With ~150K deaths, so far, we're at 4.4X the deaths of a typical flu (34K on average, from 2010-11 to 2016-2017; the last 2 years are still listed as "preliminary" data) and remember, these are modeled numbers and most experts think they're overestimated, based on the models being 2-3X over the actual reported flu deaths for school-age kids, which have to be reported by law) and are on our way to at least 5-10X, given the infection fatality ratio being 0.5-1.0% for COVID vs. 0.1% for flu - and possibly well beyond that, given that herd immunity is expected to be 55-80% of the population getting infected with COVID (unless we get lucky with "cross-reactivity" leading to much greater built-in immunity than we thought), whereas only about 10% of the US catches the flu in a year (models) - multiply that all out and it's 900K-2.64MM US deaths eventually (that's roughly 25-75X annual flu deaths).
As I've said countless times, I don't think we come anywhere near those numbers given quickly improving treatments/procedures with potential cures or near-cures coming in the fall (engineered antibodies) and vaccines by the end of the year, combined with many to most now wearing masks/distancing, but if those treatments/vaccines don't materialize and we don't wear masks or distance or have any other interventions, those far higher numbers vs. the flu are at least possible. And until we have those cures/vaccines, it seems nuts to not at least have everyone practice distancing and wear masks when distancing isn't possible (like subways, airplanes, crowded cities, churches, etc.).
Sobering. We are losing to an enemy that can be defeated. Not easily defeated, but it can be done.
65M people live in France. 21M live in Florida.
Appears NY/NJ has already Lost:
France 65 Million Residents - 30K Deaths
NY/NJ 28 Million Residents - 48K Deaths
Florida still has a chance
FL 21 Million Residents - 6K Deaths
Right, it hit them much earlier, that's the point, Florida wasn't doing badly until recently plus Florida and France are hardly alike at all, there are factors in that as wellWhy?
And I'll answer my own question. France is at a different stage because they went hard lockdown from March-May. Once/week shopping, no BS mask policy, fines for not social distancing. And that chart is the result. I am open to hearing why their "loss of Freedom" wasn't worth it.
It would make more sense to compare Florida to us.
2X or even 3X the usual flu deaths doesn't seem like its worth total destruction of the economy to avoid. But maybe it is. Maybe if we went to the old normal it would be 10X the usual annual flu deaths. I don't know.
It already rounds to over 4X the annual flu average and the dying isn't quite done yet by 8 months of a representative TTM.
Why?
And I'll answer my own question. France is at a different stage because they went hard lockdown from March-May. Once/week shopping, no BS mask policy, fines for not social distancing. And that chart is the result. I am open to hearing why their "loss of Freedom" wasn't worth it.
You really are trying too hard....how about comparing nj to france
More like 40 years.good post, for me here, I am here to challenge people to research beyond what the msm is feeding you. Get all kinds of information, Question things that do not quite make sense or seem random and hypocritical. I realize some are in love with what the msm dictates to them. Remember some like myself believe the msm has been lying to the public for 4 years now on every major story.
Your post referenced death rates in CA vs TX, FL and AZ, which is what I noted as it is reported in the RCP Tracker. Anyway, while we know you would prefer to ignore the numbers in NY/NJ/CT when the regional climate drove the spread somewhat similarly there as it is recently in the sunbelt , the overall numbers of course matter nonetheless for that reason.I've been talking about death rates in wave 2 for several weeks (which is why you brought up the summer heat/AC/indoors angle) and have posted numerous comparisons of them for FL/TX/CA/AZ and California's current death rate, per capita, is 1/2 to 1/6 the death rates, per capita, in these other states, as per my post from last Tuesday (and that gap has widened a bit since last week). So why you'd bring in overall deaths per capita is beyond me.
And if you're going to focus on overall pandemic death rates, at least get the data right. You said, "TX and FL have lower fatality rates vs. CA , AZ a tad higher (+0.2%) according to the current RCP tracker." Below are the fatality rates per 1MM in that tracker and it shows that TX is about 20% lower than CA, FL is 29% greater, and AZ has more than 2X the death rate of CA, so you got one of three right. The fact that you can be so far off from reality in the simple task of reading numbers from a table is consistent with your numerous other misinterpretations of data (e.g., posting misleading info from Horowitz) why you get no respect on this board.
FL death rate = 276/1MM
TX death rate = 178/1MM
AZ death rate = 453/1MM
CA death rate = 214/1MM
And sorry, you're making the same dumb mistake as "Greg" in misunderstanding the one Horowitz article I linked months ago that discussed why the cases were increasing in the sunbelt states, not that they were not. Try again.
Now how about all those crazy Trumpers not wearing masks in LA County! LOL.
Great Goldwater!
Arizona reported only one death yesterday.
Arizona reported only one death yesterday.
1300-1350 it was still from China ... Google is God... bubonic plague which today would not be a worry... estimates of deaths? 75-200 million... it sounded like a defense of where this came from... if you didn’t mean it why did you emphasize “ it was from Mongolia. “ ... let’s just say out of East Asia.
Because when someone says “blame China” they’re not referring to the piece of Earth upon which China sits; and when they say the plague was China’s fault too (which is clearly half in jest because we’re talking about the 14th century), I feel comfortable pointing out that the piece of earth occupied by China today was possessed by a Mongol dynasty back then — so (in jest) the mongols deserve blame.
Mexico is in the midst of an outbreak worse than ours, as measured by deaths per capita, which are about twice as high as ours are now (their case rate is artificially low, since they're not testing nearly as much as we are) and they have 16% of homes with air-conditioning vs. >90% in states like FL/TX/CA/AZ, so no, don't think it's air-conditioning (stats are easy to Google on that). Also, as I've shown before, CA's case/death rates are well below those of FL/TX/AZ, per capita - explain that one with your AC theory. The most likely reason is they have a D governor, who didn't reopen his state nearly as recklessly as the R gov's in the other states and CA has much stronger masking requirements (and less R's proportionally).
It is hard to understand why someone would try to rely so much on proven numbers in some aspects but then resort to far overgeneralized conclusions like this in others. It is equally hard to understand why it is in any way controversial that people being driven inside due to weather would adversely affect the fight to slow covid.
It does not mean that weather is the only risk factor.
770,000 people voted for Trump in LA County. Plenty of crazy to go around, pal.Your post referenced death rates in CA vs TX, FL and AZ, which is what I noted as it is reported in the RCP Tracker. Anyway, while we know you would prefer to ignore the numbers in NY/NJ/CT when the regional climate drove the spread somewhat similarly there as it is recently in the sunbelt , the overall numbers of course matter nonetheless for that reason.
And sorry, you're making the same dumb mistake as "Greg" in misunderstanding the one Horowitz article I linked months ago that discussed why the cases were increasing in the sunbelt states, not that they were not. Try again.
Now how about all those crazy Trumpers not wearing masks in LA County! LOL.
I think he was discussing CFR as that aligns with his statement exactly where AZ is 0.2% higher than CA, and FL and TX are lower, etc. Go to RCP tracker and sort by CFR.I've been talking about death rates in wave 2 for several weeks (which is why you brought up the summer heat/AC/indoors angle) and have posted numerous comparisons of them for FL/TX/CA/AZ and California's current death rate, per capita, is 1/2 to 1/6 the death rates, per capita, in these other states, as per my post from last Tuesday (and that gap has widened a bit since last week). So why you'd bring in overall deaths per capita is beyond me.
And if you're going to focus on overall pandemic death rates, at least get the data right. You said, "TX and FL have lower fatality rates vs. CA , AZ a tad higher (+0.2%) according to the current RCP tracker." Below are the fatality rates per 1MM in that tracker and it shows that TX is about 20% lower than CA, FL is 29% greater, and AZ has more than 2X the death rate of CA, so you got one of three right. The fact that you can be so far off from reality in the simple task of reading numbers from a table is consistent with your numerous other misinterpretations of data (e.g., posting misleading info from Horowitz) why you get no respect on this board.
FL death rate = 276/1MM
TX death rate = 178/1MM
AZ death rate = 453/1MM
CA death rate = 214/1MM
I think we are in the first or second inning of this. I think your post is solid, but large segments of the US economy: Hotels, airlines, casinos, movie theaters, oil and gas (less travel), automobile sales, tourism, cruise industry, etc. etc are all going to be really hurt in to the foreseeable future. We are looking at an 85% or less economy for (at least) the next six months unless something drastically changes. If the real estate market starts to tumble.....
I don't logically see how at least the existing commercial real estate market won't be significantly effected in the short and medium term. I think it will take time to play out due to commercial leases often being lengthy, but what company isn't going to at least consider reducing their leasing costs when they come up for renewal.
So out of over 10mil in LA County that's about 7.6%, thanks. Can you confirm the political affiliations with the case counts? #Science770,000 people voted for Trump in LA County. Plenty of crazy to go around, pal.
Manhattan will not be a shell of itself. People live there for a ton of reasons not related to being close to the office. More people are going to live there due to corporate space being converting to residential.
Many do, but at least some not insignificant percentage does live there for work related reasons. Losing that segment could have a pretty large effect on Manhattan. In my view, there's going to be some change, it's just a matter of how big of one and how long it lasts. These things tend to be cyclical, and it could just be the other part of the cycle. For example, in the 80s and early 90s, NJ office parks were all the rage.
Incorrect as Zelenko has published his findings.
https://www.preprints.org/manuscript/202007.0025/v1
also here:
https://files.internetprotocol.co/ebook-covid-19.pdf
Speaking of Boulware, here is a discussion of his study in preprint. https://arxiv.org/abs/2007.09477
Quote from discussion:
"Our results suggest there is probably little or no benefit if the treatment is used in patients infected for too long, like hospitalized severe patients. On the contrary, they also suggest infected patients may have a large benefit if treated as early as possible, mostly as pre-prophylaxis treatment where symptoms appear will have an estimated relative reduction of at least 72%.
Another important aspect is that the variable of the study, be asymptomatic or be symptomatic, is quite time sensitive. Future trials should adopt less time sensitive variables, such as the number of days each patient is symptomatic, which could measure the possible benefit of treatment for patients that have been exposed for more than 3 days before the beginning of treatment. Another common possibility is to adopt some score system to measure severity of symptoms.1 However, score systems are difficult to be scientifically validated because they typically depend on personal judgment, whereas the variable number of days with symptoms can be more easily replicated by other studies.
Furthermore, the hydroxychloroquine prophylaxis should also be investigated with concomitant use of azithromycin and zinc7 , as also other antivirals should also be tested as prophylaxis, measuring the relative efficacy as a measure of the elapsed time after exposure to the virus to the beginning of treatment."
First off, do you really have any confidence in the Zelenko study, which was not randomized or controlled in any way? We have no information on the "control" population at all, with regard to demographics, underlying conditions, or severity of conditions at t=0 (patients going to see a family physician could have quite different severity from patients going to the ER). Nobody can know from this "study" whether the treatment is effective or not. At a minimum we need the full data set on the control population to have any hope of determining efficacy, especially in a retrospective/observational study like this - at best, his results might suggest that we do a randomized, controlled, blinded study.
I've seen that discussion of Boulware and haven't had time to read it in any detail, apart from chuckling at his graphic, where he extrapolates from his data reanalysis time points (days 1-4) to make conclusions about what would happen if HCQ were given at Day 0. That's a statistical no-no to extrapolate beyond the given data set. So, I'm already suspicious. And at this point, the Spanish study is much stronger than the Boulware study, anyway, as per my post yesterday, so we should likely be focusing on that one.
I think he was discussing CFR as that aligns with his statement exactly where AZ is 0.2% higher than CA, and FL and TX are lower, etc. Go to RCP tracker and sort by CFR.
Yes, probably that, thanks. I didn't even look at that, as I didn't think anyone would be dumb enough to use CFR in a comparison of death rates and severity of the outbreak. Deaths per capita is the bottom line number for this pandemic, not CFR, which is subject to wild variations depending on testing. Also, even for CFR, the "difference" between AZ and CA is 0.2%, but this is a 10% difference in CFRs, so he couldn't even get that right.
This will not be a simple fix even after the virus is controlled.Sorry, I wasn't trying to paint a permanent picture of NYC, everything in life comes in cycles, my point it's going to be a while before NYC recovers from both effects of the virus and rioters (not to be confused with genuine well meaning protesters).
I have so many friends who either worked or lived in the city (and loved it) who really have no desire to go back any time soon.
I said it was a hypothesis, not proven conclusions - big difference. Also, you never replied to my post on that, replying to yours from the weekend.It is hard to understand why someone would try to rely so much on proven numbers in some aspects but then resort to far overgeneralized conclusions like this in others. It is equally hard to understand why it is in any way controversial that people being driven inside due to weather would adversely affect the fight to slow covid.
It does not mean that weather is the only risk factor.
Rrrrrright how a state's fatality rate compares is meaningless in judging a state dealing with the chicomvirus. I wonder why the tracker even bothers to report it lol.Yes, probably that, thanks. I didn't even look at that, as I didn't think anyone would be dumb enough to use CFR in a comparison of death rates and severity of the outbreak. Deaths per capita is the bottom line number for this pandemic, not CFR, which is subject to wild variations depending on testing. Also, even for CFR, the "difference" between AZ and CA is 0.2%, but this is a 10% difference in CFRs, so he couldn't even get that right.
Sorry you can't make the horrendous numbers in NY/NJ/CT at 7.5% to over 9%, or the 7%+ in Mich, go away and hide the terrible chicomvirus response by those certain political party governors like sending infected elderly patients to nursing homes.
From the NJ Economic front,
https://www.nj.com/coronavirus/2020...e-reopen-what-that-means-for-our-economy.html
“It’s just devastating. This is the first downturn we deliberately engineered. Given the severity of the health crisis, we have to shut down the economy,” said Hughes, co-author of the “Coronavirus Economic Rebound” study. “In order to save lives, we had to sacrifice livelihoods. So that high unemployment rate is a paradox.”
In June, the state’s unemployment rate reached 16.2%, according to the Bureau of Labor Statistics, up from 15.2% in May and the highest since record keeping began in 1976.
At the second highest in the nation — behind only Massachusetts at 17.5% — the number of jobs in New Jersey are down to what they were in 1985, when at least 1.2 million fewer people lived in the state, said Hughes.
The key reason for the skyrocketing unemployment rate is that Gov. Phil Murphy was among the first to impose major lockdown restrictions, so the economy is experiencing the effects of it faster, Hughes explained.
I will add that Murphy continues to keep things locked down as we know. We do know that loss of income, jobs leads to increased in depression, drug use, etc. so the cost of the virus cannot be counted just by looking at the deaths due directly to the virus.
https://www.forbes.com/sites/onemin...stance-abuse-a-watershed-moment/#2e72128964bc
https://www.nj.com/coronavirus/2020...e-reopen-what-that-means-for-our-economy.html
“It’s just devastating. This is the first downturn we deliberately engineered. Given the severity of the health crisis, we have to shut down the economy,” said Hughes, co-author of the “Coronavirus Economic Rebound” study. “In order to save lives, we had to sacrifice livelihoods. So that high unemployment rate is a paradox.”
In June, the state’s unemployment rate reached 16.2%, according to the Bureau of Labor Statistics, up from 15.2% in May and the highest since record keeping began in 1976.
At the second highest in the nation — behind only Massachusetts at 17.5% — the number of jobs in New Jersey are down to what they were in 1985, when at least 1.2 million fewer people lived in the state, said Hughes.
The key reason for the skyrocketing unemployment rate is that Gov. Phil Murphy was among the first to impose major lockdown restrictions, so the economy is experiencing the effects of it faster, Hughes explained.
I will add that Murphy continues to keep things locked down as we know. We do know that loss of income, jobs leads to increased in depression, drug use, etc. so the cost of the virus cannot be counted just by looking at the deaths due directly to the virus.
https://www.forbes.com/sites/onemin...stance-abuse-a-watershed-moment/#2e72128964bc
I said it was a hypothesis, not proven conclusions - big difference. Also, you never replied to my post on that, replying to yours from the weekend.
I'm not sure what there was to respond to but maybe I missed it. I do think there are examples, like Southern California, that show rises are due to factors other than political leanings. I also think using political leanings far overestimates the number of people in the country that even care about politics. Even in presidential election years, a huge percentage of people don't even care enough to vote.
I think there is a reasonable argument to make that some places "opened" to early or too aggressively, but what is very difficult to know is what would have happened had they waited a period of time that was feasible. It is equally possible that the virus would have grown in these places for the reasons that it hadn't really been there yet to infect the most vulnerable, and other factors such as weather driving people inside and infection spreading from Mexico wouldn't have led to similar results anyway.
I think the point about a lot of this is that, like a scientific experiment, you don't have a "control" to compare things to. You don't get to have two Floridas or two states of Texas. You then are left with educated guesses which have supporting and contradicting factors. I personally do not like it when people ignore these uncertainties and are not only so sure so as to ignore other opinions, but also ignore the many conflating factors.
LOL, but sCiENcE.I said it was a hypothesis, not proven conclusions - big difference. Also, you never replied to my post on that, replying to yours from the weekend.
According to the data found here..
https://www.cdc.gov/nchs/nvss/vsrr/covid19/index.htm
..is seems that since the week of the 4th of July we have been UNDER the expected deaths count by a wide margin. Perhaps the "average number across the same week in 2017–2019" were exceptionally high for some reason.. but it hardly shows that we are in the middle of the new Black Death.
On April 11 we were at 42% MORE than the expected death rate from the average of the same weeks for 2017-2019. And the last number was only 16% of the expected number of deaths.. that is 84% UNDER the expected number of deaths. That 16% has to have been an abberation.. the previous weeks were 67%, 93% and 99% of the expected number of deaths.
I have seen people posting all kinds of things about rising numbers of cases here or there.. but deaths seem to be dropping quite a bit. Why aren't deaths rising if the cases are rising? Are we just catching more cases now that would have been ignored earlier? Is the virus weaker now and people are just not getting the serious symptoms that cause death as often?
https://www.cdc.gov/nchs/nvss/vsrr/covid19/index.htm
..is seems that since the week of the 4th of July we have been UNDER the expected deaths count by a wide margin. Perhaps the "average number across the same week in 2017–2019" were exceptionally high for some reason.. but it hardly shows that we are in the middle of the new Black Death.
On April 11 we were at 42% MORE than the expected death rate from the average of the same weeks for 2017-2019. And the last number was only 16% of the expected number of deaths.. that is 84% UNDER the expected number of deaths. That 16% has to have been an abberation.. the previous weeks were 67%, 93% and 99% of the expected number of deaths.
I have seen people posting all kinds of things about rising numbers of cases here or there.. but deaths seem to be dropping quite a bit. Why aren't deaths rising if the cases are rising? Are we just catching more cases now that would have been ignored earlier? Is the virus weaker now and people are just not getting the serious symptoms that cause death as often?
https://www.theguardian.com/world/2020/jul/27/europe-braces-for-second-wave-of-coronavirus
Obviously not the levels that we have seen in the US recently but Europe is starting to see some increase in cases, mainly driven by the young.
Obviously not the levels that we have seen in the US recently but Europe is starting to see some increase in cases, mainly driven by the young.
First off, do you really have any confidence in the Zelenko study, which was not randomized or controlled in any way? We have no information on the "control" population at all, with regard to demographics, underlying conditions, or severity of conditions at t=0 (patients going to see a family physician could have quite different severity from patients going to the ER). Nobody can know from this "study" whether the treatment is effective or not. At a minimum we need the full data set on the control population to have any hope of determining efficacy, especially in a retrospective/observational study like this - at best, his results might suggest that we do a randomized, controlled, blinded study.
I've seen that discussion of Boulware and haven't had time to read it in any detail, apart from chuckling at his graphic, where he extrapolates from his data reanalysis time points (days 1-4) to make conclusions about what would happen if HCQ were given at Day 0. That's a statistical no-no to extrapolate beyond the given data set. So, I'm already suspicious. And at this point, the Spanish study is much stronger than the Boulware study, anyway, as per my post yesterday, so we should likely be focusing on that one.
Where did I say anything about confidence in Zelenko study? You made an incorrect statement that Zelenko never published anything which I corrected via the link provided. I offered no commentary on what I thought of his paper.
Frankly, I have seen you do this quite a bit and then later say that someone said things they never did. It seems to be your approach. I usually find that people who have trouble being truthful do this frequently but I do not believe that of you. You respond like you did above to me and then later make outlandish claims that I thought that his published study was excellent/believable, etc. When the person you do that to never said or supported what you claim.
Hey if you really believe the virus did not come out of China to the entire world I don’t care . If you continue to create the narrative blame Mongolia I won’t lose sleep but it came out of East Asia and last we checked they were both located there between 1300-1350 AD. Most of the disease we have seen in the past originated in either Africa or your favorite ... China.Because when someone says “blame China” they’re not referring to the piece of Earth upon which China sits; and when they say the plague was China’s fault too (which is clearly half in jest because we’re talking about the 14th century), I feel comfortable pointing out that the piece of earth occupied by China today was possessed by a Mongol dynasty back then — so (in jest) the mongols deserve blame.
Didn't the Chinese use the Black Death as a means to overthrow Mongol Rule? Wasn't that the origins of the Ming Dynasty? Maybe they brewed that up in a lab in Wuhan.Because when someone says “blame China” they’re not referring to the piece of Earth upon which China sits; and when they say the plague was China’s fault too (which is clearly half in jest because we’re talking about the 14th century), I feel comfortable pointing out that the piece of earth occupied by China today was possessed by a Mongol dynasty back then — so (in jest) the mongols deserve blame.
Worst market in many years and was so pre pandemic... don’t you watch Million Dollar Listing?How are the prices in NYC for purchasing?
Like in the “new improved “ Age of Enlightenment . Remember the more things change the more they stay the same.I think a death knell is unlikely for big cities, and a period of change is more probable. There will be closures, and time will have to pass before we see bars / restaurants / entertainment scaled up again.
Reluctance to use mass transit may persist for a time. There will be financial holes for strained city financial planners to overcome.
That said, urban density has many social and economic advantages that are likely to continue to drive urban living over the long haul.
I wouldn’t even bet on a long-term secular migration from north to south; I think it is likely to be a near-term pressure for northern cities. Climate change complications and costs, fresh water scarcity, and infrastructure constraints are some of the looming headwinds for some of the rapidly growing areas that are projected to ultimately reverse the current migration patterns
It's not AC. In April Mexico was way down on the World Meter list. Illegals here in central NC (cant speak for CA, AZ, TX and FL), ran back to Mexico in April and early May to avoid the virus, but bringing the virus with them. Then Mexico explodes, now #4 on the death list. The illegals came back in June seeking healthcare and work. Three weeks ago, NC Human Svcs had a stat that 46% of positive tests in NC were hispanic, yet they make up only 10% of the population. Yeah I know, no one wants to acknowledge this stuff, but that's what happened. My eyes are fine.Don't be so quick to discount the effect A/C has on humans spending more time indoors.
I suspect that Mexico has a larger percentage of people living with extended families than we do in the US. That may be a cause close contact even though they do not have as much A/C.
- Status
- Not open for further replies.
Similar threads
- Replies
- 47
- Views
- 3K
- Replies
- 472
- Views
- 19K
- Replies
- 136
- Views
- 5K
- Replies
- 90
- Views
- 3K
- Replies
- 25
- Views
- 2K
ADVERTISEMENT
ADVERTISEMENT