I think that ship sailed 12 months ago.Right, we should model our response to China's. Sounds great.

Colleges
- AAC
- ACC
- Big 12
- Big East
- Big Ten
- Pac-12
- SEC
- Atlantic 10
- Conference USA
- Independents
- Junior College
- Mountain West
- Sun Belt
- MAC
- More
- Navy
- UAB
- Tulsa
- UTSA
- Charlotte
- Florida Atlantic
- Temple
- Rice
- East Carolina
- USF
- SMU
- North Texas
- Tulane
- Memphis
- Miami
- Louisville
- Virginia
- Syracuse
- Wake Forest
- Duke
- Boston College
- Virginia Tech
- Georgia Tech
- Pittsburgh
- North Carolina
- North Carolina State
- Clemson
- Florida State
- Cincinnati
- BYU
- Houston
- Iowa State
- Kansas State
- Kansas
- Texas
- Oklahoma State
- TCU
- Texas Tech
- Baylor
- Oklahoma
- UCF
- West Virginia
- Wisconsin
- Penn State
- Ohio State
- Purdue
- Minnesota
- Iowa
- Nebraska
- Illinois
- Indiana
- Rutgers
- Michigan State
- Maryland
- Michigan
- Northwestern
- Arizona State
- Oregon State
- UCLA
- Colorado
- Stanford
- Oregon
- Arizona
- California
- Washington
- USC
- Utah
- Washington State
- Texas A&M
- Auburn
- Mississippi State
- Kentucky
- South Carolina
- Arkansas
- Florida
- Missouri
- Ole Miss
- Alabama
- LSU
- Georgia
- Vanderbilt
- Tennessee
- Louisiana Tech
- New Mexico State
- Middle Tennessee
- Western Kentucky
- UTEP
- Florida International University
High School
- West
- Midwest
- Northeast
- Southeast
- Other
- Alaska
- Arizona
- California
- Colorado
- Nevada
- New Mexico
- Northern California
- Oregon
- Southern California Preps
- Washington
- Edgy Tim
- Indiana
- Kansas
- Nebraska
- Iowa
- Michigan
- Minnesota
- Missouri
- Oklahoma Varsity
- Texas Basketball
- Texas
- Wisconsin
- Delaware
- Maryland
- New Jersey Basketball
- New Jersey
- New York City Basketball
- Ohio
- Pennsylvania
- Greater Cincinnati
- Virginia
- West Virginia Preps
ADVERTISEMENT
Install the app
How to install the app on iOS
Follow along with the video below to see how to install our site as a web app on your home screen.
Note: This feature may not be available in some browsers.
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
OT: NEW EVERYTHING / ANYTHING COVID-19 THREAD PART II
- Thread starter Richie O
- Start date
- Status
- Not open for further replies.
You think those people that check tickets at rutgers stadium gonna be able to check for vaccine cards ? Talk about out performing your pay grade

How about retina scans that link to your vaccine records?You think those people that check tickets at rutgers stadium gonna be able to check for vaccine cards ? Talk about out performing your pay grade
All NJ Transit workers eligible for vaccine on 3/15. Makes perfect sense and I would have had them a little earlier but we were a little confused in the early stages here in NJ. Things are opening up and hopefully all elderly will be completed by that time as well.
I’m biting my tongue really hard here on what we want to check ID’s for and what we allow to go unchecked. LolYou think those people that check tickets at rutgers stadium gonna be able to check for vaccine cards ? Talk about out performing your pay grade
How about a chip inserted under your skin. My dog had one. Thankfully never had to use it.How about retina scans that link to your vaccine records?
I think the vaccines already input that chip when you get the shots. :)How about a chip inserted under your skin. My dog had one. Thankfully never had to use.
Rutgers should allow Mail-In vaccine validation to the Ticketing office. As long as they are received 1 week before game day, the self confirming applicant should be good to go !! The government trusts this process for important events, so should be good for a football game... right? Since RU is using electronic ticketing now, should not be a problem. The ticket account owner can be responsible for collecting the validations from all the tickets he /she distributes and send them all in to RU ticket office.I’m biting my tongue really hard here on what we want to check ID’s for and what we allow to go unchecked. Lol
Last edited:
You can't be serious!!Rutgers should allow Mail-In vaccine validation to the Ticketing office. As long as they are received 1 week before game day, the self confirming applicant should be good to go !! The government trusts this process for important events, so should be good for a football game... right? Since RU is using electronic ticketing now, should not be a problem. The ticket account owner can be responsible for collecting the validations from all the tickets he /she distributes and send them all in to RU ticket office.
Right, we should model our response to China's. Sounds great.
More than just China doing vaccine passes
This P1 variant really has the insurance sector spooked. A number of firms we consult for are asking us to do claim analysis on potential exposure if this variant goes through an exponential growth phase. This was not asked of us for any of the other variants in circulation.
Looks like it's that study out of Brazil showing significant reinfection that has the gears turning. Plus if a vaccine tweak is needed it would render all of the vaccinations to date relatively useless for what they were intended for and delay vaccination another 3-6 months.
Looks like it's that study out of Brazil showing significant reinfection that has the gears turning. Plus if a vaccine tweak is needed it would render all of the vaccinations to date relatively useless for what they were intended for and delay vaccination another 3-6 months.
Sure go with that. I ‘m having Singapore Mei Fun tonite.Gonna go out on a limb and say they have this figured out.
Well let ‘s hope not a reality. Ok so let’s allow in all of South and Central America. Brilliant educated morons.This P1 variant really has the insurance sector spooked. A number of firms we consult for are asking us to do claim analysis on potential exposure if this variant goes through an exponential growth phase. This was not asked of us for any of the other variants in circulation.
Looks like it's that study out of Brazil showing significant reinfection that has the gears turning. Plus if a vaccine tweak is needed it would render all of the vaccinations to date relatively useless for what they were intended for and delay vaccination another 3-6 months.
This P1 variant really has the insurance sector spooked. A number of firms we consult for are asking us to do claim analysis on potential exposure if this variant goes through an exponential growth phase. This was not asked of us for any of the other variants in circulation.
Looks like it's that study out of Brazil showing significant reinfection that has the gears turning. Plus if a vaccine tweak is needed it would render all of the vaccinations to date relatively useless for what they were intended for and delay vaccination another 3-6 months.
Think they already found out that the P1 is not as bad as the SA variant. Vaccines should still work on them both, although not as well as the OG strain.
If only we had a communist government and citizens were slaves of the state. Pretty easy to "get stuff done" in those circumstances.More than just China doing vaccine passes
Think they already found out that the P1 is not as bad as the SA variant. Vaccines should still work on them both, although not as well as the OG strain.
OG, = China Strain?
Not sure this was posted yet. And there is no link to the study.

 news.yahoo.com
news.yahoo.com
(edit) Here is the study
Obesity a driving factor in COVID-19 deaths, global report finds
The report, which described a "dramatic" correlation between countries' COVID-19 death and obesity rates, found that 90% or 2.2 million of the 2.5 million deaths from the pandemic disease so far were in countries with high levels of obesity. The study analysed the COVID-19 death figures from...
(edit) Here is the study
Loading…
www.worldobesityday.org
Apparently this guy is in a band in the UK. The Stone Roses
Storage conditions are now a minor advantage for J&J and Novavax over Pfizer(assuming they get approval on the 2-week refrigerated storage, which they will) and Moderna. Single shot from J&J is certainly an advantage, but you can't say J&J and Novavax have better efficacy than the mRNA vaccines. We just don't have good enough head-to-head data, especially on the newer variants to say that.
In fact, comparing efficacy (prevention of symptomatic COVID in vaccinated vs. non-vaccinated people in the trials) across all of the vaccines is almost impossible, since the trials were conducted on different populations at different times in different locations with different predominant strains active at that time/location. The links below contain good info on comparisons across some of the vaccines.
The Pfizer/Moderna vaccines both had about 95% efficacy against the "original" coronavirus variant, while Novavax had 89% efficacy overall in its UK trial, but that includes the UK variant (B.117) and Novavax calculated that their efficacy was likely about 95.6% against the original coronavirus variant, which is essentially the same as Pfizer/Moderna, which did not face the UK or South African (B.1.351) variants at all. In contrast, the J&J single dose vaccine only had 66% efficacy overall, but 72% in the US vs. only 57% in South Africa, where it's mostly been against the SA variant. And the AZ vaccine only had 22% efficacy against the SA variant.
We have no real world data on Pfizer/Moderna on either the UK or SA variants, but we do have lab data with pseudoviruses indicating a less robust immune response elicited by these mRNA vaccines against the SA variant, but probably enough to still be effective according to virologists - but we'd need real world clinical or post-approval data to know for sure.
So, it looks like the Pfizer, Moderna and Novavax vaccines have similar high efficacies in the ~95% range (against the original strain), while J&J and AZ have lower efficacies, but we don't have apples-to-apples comparisons across the variants for each vaccine. The good news is that, so far, it appears that all of the vaccines have been almost perfect in preventing hospitalizations in trials (and Pfizer's has shown only 0.04% hospitalizations out of 523K vaccinated in Israel, so far) and they've all been 100% effective in preventing deaths.
So while we could really use better apples-to-apples comparisons, we're unlikely to get them soon and my guess is we'll simply continue to use whatever vaccines we have, since preventing hospitalizations and deaths is jobs #1, 2, and 3 for these vaccines. The issue with lower efficacy against some variants is that that would mean more people need to be vaccinated to achieve herd immunity, since transmissions will continue with less efficacious vaccines on certain variants, but we're just going to have to live with that for now.
As per my post of Derek Lowe's blog yesterday, this is why we need to get vaccines in arms as fast as possible, since the more transmissions we have the more chances for evolutionary roulette leading to an eventual virus that can "escape" the vaccines we have, although it's also good to know that the vaccines can all be quickly reconfigured for booster shots to address troublesome variants, especially the mRNA vaccines by Pfizer and Moderna. And even though cases are way down vs. our peak several weeks ago, cases are still as high as they were in the summer (and likely were in the spring, if we had been testing), so that's still plenty of cases and opportunities for mutations.
https://www.fool.com/investing/2021/02/04/heres-how-novavaxs-vaccine-stacks-against-modernas/
https://www.telegraph.co.uk/global-...vs-oxford-moderna-astrazeneca-covid-compared/
https://www.fiercepharma.com/pharma...om-j-j-novavax-show-there-s-room-for-everyone
Here's an update on variants and vaccines. A recent paper (preprint, not peer reviewed yet, but from a very reliable source) just came out looking much more deeply into the adaptive immune responses (T-cells/B-cells) to all of the major variants in both infected/recovered patients and post-mRNA-vaccination (Pfizer/Moderna) patients, and the news is quite good as the adaptive immune response to the UK (B.1.1.7), South African (B.1.351), Brazilian (P.1), and California (CAL.20C) variants is quite strong for both types of patients. This likely means that reports that antibody responses to these variants were not nearly as robust, is likely not that important and post-vaccination immune response to these strains should likely be assumed to be similar to what is seen for the original strain.
https://www.biorxiv.org/content/10.1101/2021.02.27.433180v1.full.pdf
Derek Lowe also weighed in on this paper and had similar comments, which is reassuring, although we're 100% aligned that we're playing evolutionary Russian roulette with variants, meaning the more transmissions that occur in the world, the more likely a variant could emerge that eludes the vaccines, which is why vaccinating as fast as possible here and worldwide is so important.
Speaking of that he also weighed in on the Novavax vaccine conundrum in the US, where their phase III clinical trial is likely decelerating due to decreased transmission rates, which could delay filing for an EUA. He, like many others, believes that the robust Novavax phase III dataset from the UK and SA ought to be enough for a US EUA, especially given the preceding paragraph - we need to get transmissions down both to save lives and to reduce the probability of elusive variants and adding another vaccine, especially a refrigerator storage one, can only help in that regard.
https://blogs.sciencemag.org/pipeline/archives/2021/03/02/early-march-vaccine-thoughts
Here's an update on variants and vaccines. A recent paper (preprint, not peer reviewed yet, but from a very reliable source) just came out looking much more deeply into the adaptive immune responses (T-cells/B-cells) to all of the major variants in both infected/recovered patients and post-mRNA-vaccination (Pfizer/Moderna) patients, and the news is quite good as the adaptive immune response to the UK (B.1.1.7), South African (B.1.351), Brazilian (P.1), and California (CAL.20C) variants is quite strong for both types of patients. This likely means that reports that antibody responses to these variants were not nearly as robust, is likely not that important and post-vaccination immune response to these strains should likely be assumed to be similar to what is seen for the original strain.
https://www.biorxiv.org/content/10.1101/2021.02.27.433180v1.full.pdf
Derek Lowe also weighed in on this paper and had similar comments, which is reassuring, although we're 100% aligned that we're playing evolutionary Russian roulette with variants, meaning the more transmissions that occur in the world, the more likely a variant could emerge that eludes the vaccines, which is why vaccinating as fast as possible here and worldwide is so important.
Speaking of that he also weighed in on the Novavax vaccine conundrum in the US, where their phase III clinical trial is likely decelerating due to decreased transmission rates, which could delay filing for an EUA. He, like many others, believes that the robust Novavax phase III dataset from the UK and SA ought to be enough for a US EUA, especially given the preceding paragraph - we need to get transmissions down both to save lives and to reduce the probability of elusive variants and adding another vaccine, especially a refrigerator storage one, can only help in that regard.
https://blogs.sciencemag.org/pipeline/archives/2021/03/02/early-march-vaccine-thoughts
Hey @DJ Spanky - remember when I was whining about locked threads meaning the "reply" and "quote" functions were disabled, which annoyed me as I do that a lot? Figured out a workaround. Simply reply to any post in the thread, strip out the post contents, replacing it with the contents from the post in the locked thread, and then replace the "post #" in the quoted post with the post # from the locked thread post. See above.
Apparently this guy is in a band in the UK. The Stone Roses
Sorry, but who cares?
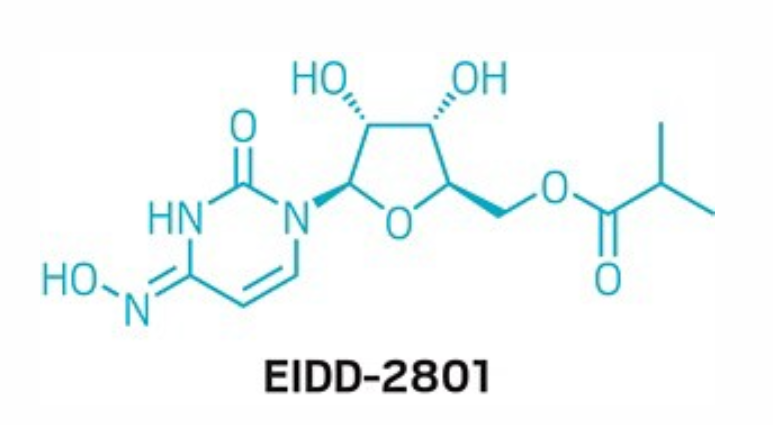
Some more details on what could look like the "afterthought" part of the Merck announcement the other day, relative to the vaccine announcements, but may end up being pretty important. The antiviral drug that Merck has licensed from Ridgeback Biotherapeutics, known as EIDD-2081, which came from the Emory Institute of Drug Development, a small company, that George Painter (famed drug discovery scientist) joined in 2013, shows some amazing activity against all kinds of viruses (including SARS-CoV-2) in vitro and in animals and is about to start phase II clinical trials.
It has shown better activity against the virus in vitro and in animals than remdesivir - both attack the same RNA polymerase enzyme in the virus, but Remdesivir blocks the enzyme so the virus can't replicate, while EIDD-2801 causes the enzyme to make replication mistakes which ead to a catastrophic mutational burden.
Whether it will work well in humans is obviously an open question, but if it does, one major advantage it has over remdesivir is that it's orally bioavailable, so it's available in tablet form, meaning it doesn't need to be dosed by IV in a hospital. One drawback is its potential mutagenicity, although with an acute (5-day dosing), potentially lifesaving application, one would think that wouldn't be a showstopper. It also looks like a relatively simple molecule to make (good chance this would've been my team's project if I hadn't retired), so if it works, I doubt availability would will be a major issue. Stay tuned.
https://cen.acs.org/pharmaceuticals..._source=LJ&utm_medium=Social&utm_campaign=CEN
https://www.ft.com/content/de7df1ee-c566-4c79-9b3e-9b7d792d424c
A paper was published today on phase I clinical trials (pharmacokinetics and safety, not efficacy) with Merck's orally bioavailable antiviral drug, molnupiravir (MK-4482). This is the molecule I've been consulting on for the past 6 months, working with my old group in the Process R&D area (in an ironic twist, the guy leading the project form the process side was in my group for 10 years, but now he's my "boss" lol, which we chuckle about). The paper is linked below and it at least appears that the drug is metabolized as expected and is pretty well tolerated. Now we just need to see efficacy, which will be coming by late March.
If effective in large scale trials, this would become the first orally available (capsule/tablet) antiviral for use in mild to moderately ill COVID patients, where there's certainly a need as remdesivir isn't particularly effective and requires an IV. Also, this could likely be co-administered with the antibody cocktails, as they have different mechanisms of action, which would likely be complementary. Derek Lowe (In the Pipeline) also blogged about this small molecule drug candidate today and he's quite upbeat on it, given how effective it has been in animal studies with COVID and other viruses, so far.
https://aac.asm.org/content/aac/early/2021/02/24/AAC.02428-20.full.pdf
https://blogs.sciencemag.org/pipeli...-last-of-the-small-molecule-coronavirus-hopes
Huge Stone Roses fan, but Ian has always been a bit of a wanker, lol, which is why they've only put out few albums over 30 years...Apparently this guy is in a band in the UK. The Stone Roses
Connecticut is lifting capacity restrictions on March 19th. Mask rules are not changing for now.
NBC tweet on Connecticut
NBC tweet on Connecticut
A
anon_ivydyf0amkzay
Guest
They’re ALL China strains...OG, = China Strain?
/HTH
They’re ALL China strains...
/HTH
Yes, correct.
For the initial outbreak in Wuhan, yes, there's no way such an enforced draconian lockdown would have ever worked here and I'm good with that. However, post-Wuhan, their use of our pandemic playbook was textbook, especially with regard to massive, rapid testing anywhere there were flare-ups (along with tracing/isolating contacts), which is what one has to do to prevent flare-ups from becoming major outbreaks. That and having a very effective communications program to effect near 100% mask wearing. Other countries, like South Korea, Taiwan and several others in that table I posted were able to be similarly efficient and have far, far fewer cases/deaths.If only we had a communist government and citizens were slaves of the state. Pretty easy to "get stuff done" in those circumstances.
We all understand . We all know where it came from. We all know how many incompetents there were and still are. We know it is still political. We know eventually people are going to say Enough Is Enough. We know know the reasons it is still used as a weapon even with 3 vaccines available and millions able soon to be vaccinated . Yet the‘re still predicting doom n gloom daily . NOT HOPE but contempt for people , groups, philosophical differences.Face it people are sick of this crap.Goodnite 🤟
A friend of my daughter called and received the JNJ shot all in the same day in Jackson
It looks like things are opening up because anecdotally I have become aware of at least 10 people who were able to schedule the shot within a week
It looks like things are opening up because anecdotally I have become aware of at least 10 people who were able to schedule the shot within a week
Yep, seeing tons of friends now getting shots scheduled, which is great...A friend of my daughter called and received the JNJ shot all in the same day in Jackson
It looks like things are opening up because anecdotally I have become aware of at least 10 people who were able to schedule the shot within a week
Yet my parents in their 80's, who registered on the state website as soon as they were eligible, still have received no opportunity to book appointments from the state.A friend of my daughter called and received the JNJ shot all in the same day in Jackson
It looks like things are opening up because anecdotally I have become aware of at least 10 people who were able to schedule the shot within a week
I later registered them with several other sites that use their own system.
Thanks to helpful suggestions on this football message board, I was able to get them appointments at Rowan, Sewell/Deptford for later this month.
But the fact the the state has yet to contact them to make appointments, even while I keep reading here and elsewhere how people got appointments like you describe is incredible. NJ's system is a major cluster F!@$.
By comparison, I live in New Hampshire. Here you register with the state and nowhere else. All vaccination appointments are scheduled through one system. All the state-run sites as well as the CVS and Walgreens, etc are handled in the same system. My group isn't yet eligible, but my wife and her mom, who are were initially given appointments for a first shot in April. Then as the supply increased they both received calls with the opportunity to move up their appointments. They had their first shots a couple weeks ago. There was no calling multiple places, or registering with multiple websites. No opening multiple incognito browser sessions on vaccine appointment sites to try and secure better "lottery" numbers. no muss, no fuss. Yes NH has 1 million people to NJ's 8 million. But that should not prevent NJ from managing a single cohesive system that lets the 80 year old's, who are not computer savvy, secure appointments in a simple fashion.
My staff and I all had the Pfizer vaccine. We all had symptoms post 2nd shot including tired, head aches, muscle aches , chills and one person had a low grade fever. We all tested ourselves 3 weeks post vaccine for antibodies and we all have them. Life is good
As of this morning the top 5 counties by % of population receiving at least 1 vaccination
Cape May 24.3%
Morris 22.3%
Gloucester 19.0%
Monmouth 18.5%
Somerset 18.2%
Monmouth County, NJ COVID-19 Vaccine Tracker | heraldtribune.com
Cape May 24.3%
Morris 22.3%
Gloucester 19.0%
Monmouth 18.5%
Somerset 18.2%
Monmouth County, NJ COVID-19 Vaccine Tracker | heraldtribune.com
CVS just opened up another 100+ NJ locations where you can get the vaccine.
That’s not what he meant as some of my men are very young and qualify just like you did.Thanks for sticking up for me to the troll but to clarify I don’t have any conditions, and I don’t live in NJ. I work at FBI HQ and have to go into the office every day so was eligible under law enforcement. Guy in the cubicle next to me got covid in early Jan but thanks to mask-wearing and distancing none of the rest of us got it. Was behind most of my coworkers in getting an appointment but now we’re all vaccinated pretty much which is really awesome.
Can’t be as not everyone will be able to do that.It will all be digital I’m sure.
My staff and I all had the Pfizer vaccine. We all had symptoms post 2nd shot including tired, head aches, muscle aches , chills and one person had a low grade fever. We all tested ourselves 3 weeks post vaccine for antibodies and we all have them. Life is good
Just my opinion but the state should have had the Queen of Rutgers Football at the very front of the line😁
Yet my parents in their 80's, who registered on the state website as soon as they were eligible, still have received no opportunity to book appointments from the state.
I later registered them with several other sites that use their own system.
Thanks to helpful suggestions on this football message board, I was able to get them appointments at Rowan, Sewell/Deptford for later this month.
But the fact the the state has yet to contact them to make appointments, even while I keep reading here and elsewhere how people got appointments like you describe is incredible. NJ's system is a major cluster F!@$.
By comparison, I live in New Hampshire. Here you register with the state and nowhere else. All vaccination appointments are scheduled through one system. All the state-run sites as well as the CVS and Walgreens, etc are handled in the same system. My group isn't yet eligible, but my wife and her mom, who are were initially given appointments for a first shot in April. Then as the supply increased they both received calls with the opportunity to move up their appointments. They had their first shots a couple weeks ago. There was no calling multiple places, or registering with multiple websites. No opening multiple incognito browser sessions on vaccine appointment sites to try and secure better "lottery" numbers. no muss, no fuss. Yes NH has 1 million people to NJ's 8 million. But that should not prevent NJ from managing a single cohesive system that lets the 80 year old's, who are not computer savvy, secure appointments in a simple fashion.
I think that is a fair assessment and NJ should be criticized for it
A friend of my daughter called and received the JNJ shot all in the same day in Jackson
It looks like things are opening up because anecdotally I have become aware of at least 10 people who were able to schedule the shot within a week
In the past week my ex, son, daughter, sister, and 3 friends all had appt's scheduled. I showed up at Brookdale CC only to find a friend in line with the same scheduled time.
I haven't seen one plan about vaccination IDs that didn't have major flaws.Can’t be as not everyone will be able to do that.
- Status
- Not open for further replies.
Similar threads
- Replies
- 175
- Views
- 6K
- Replies
- 77
- Views
- 2K
- Replies
- 592
- Views
- 15K
ADVERTISEMENT
Latest posts
-
-
With the portal now open, does Gavin Wimsatt enter after the spring game?
- Latest: Nycrusupporter
-
-

ADVERTISEMENT