Summary:
- Note: I'm using 7-day moving averages on a per capita (per 1MM) basis for these discussions of cases, hospitalizations and deaths, from the Covidtracking site. The biggest issue right now, data-wise, is the Covidtracking site has incorporated the extra 600 TX deaths on one day on the TX chart, but appears to have spread them out over the last 6 days in the national chart (and Worldometers hasn't put them in yet, which is why they're death 7-day avg is about 100 less than Covidtracking).
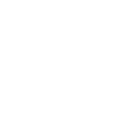
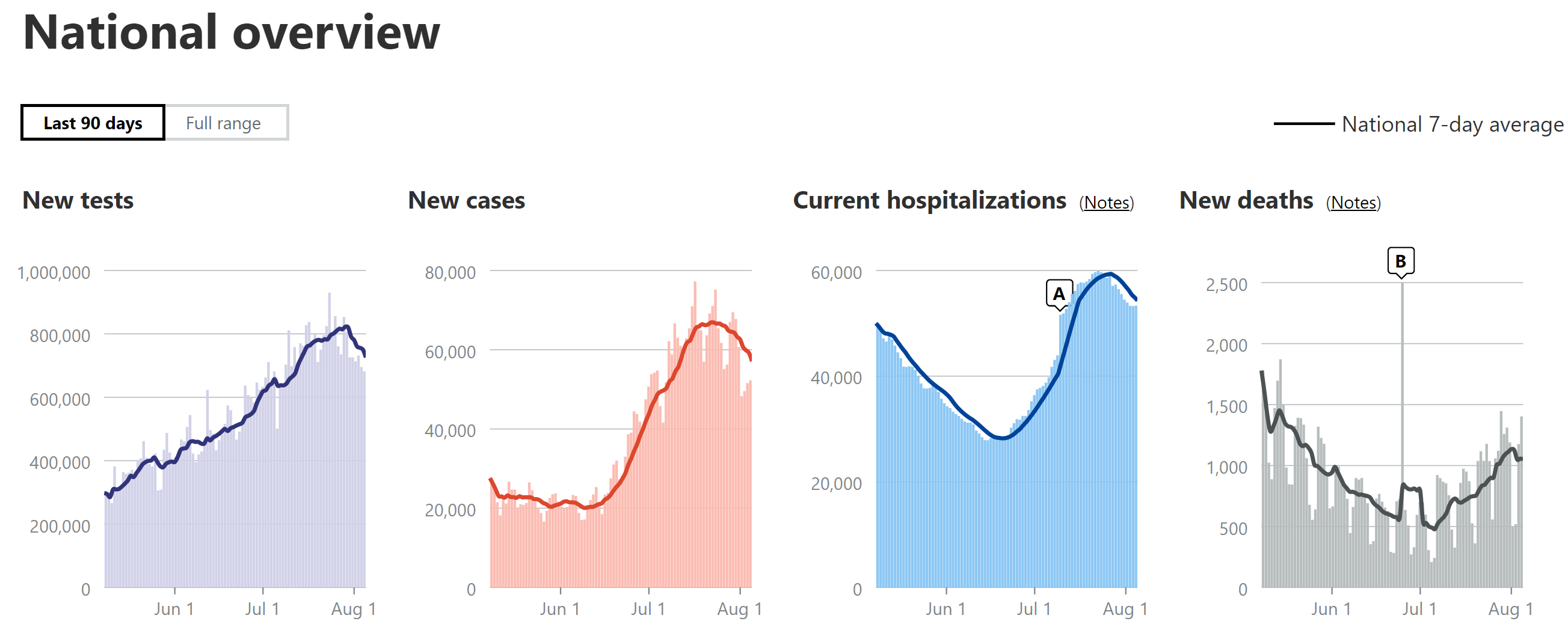
- Nationally, cases definitely have now peaked and remain roughly at ~2X vs. the first wave, while hospitalizations look to be just peaking now and will likely be slightly more than the peak in the first wave, but only a little more than half of what they were in the first wave (relative to cases, which are now twice as much per capita). Deaths are up nearly 2X from their early July low and climbing steadily and are now about 47% of the April peak (1050 now vs. 2250 in April - 7-day averages).
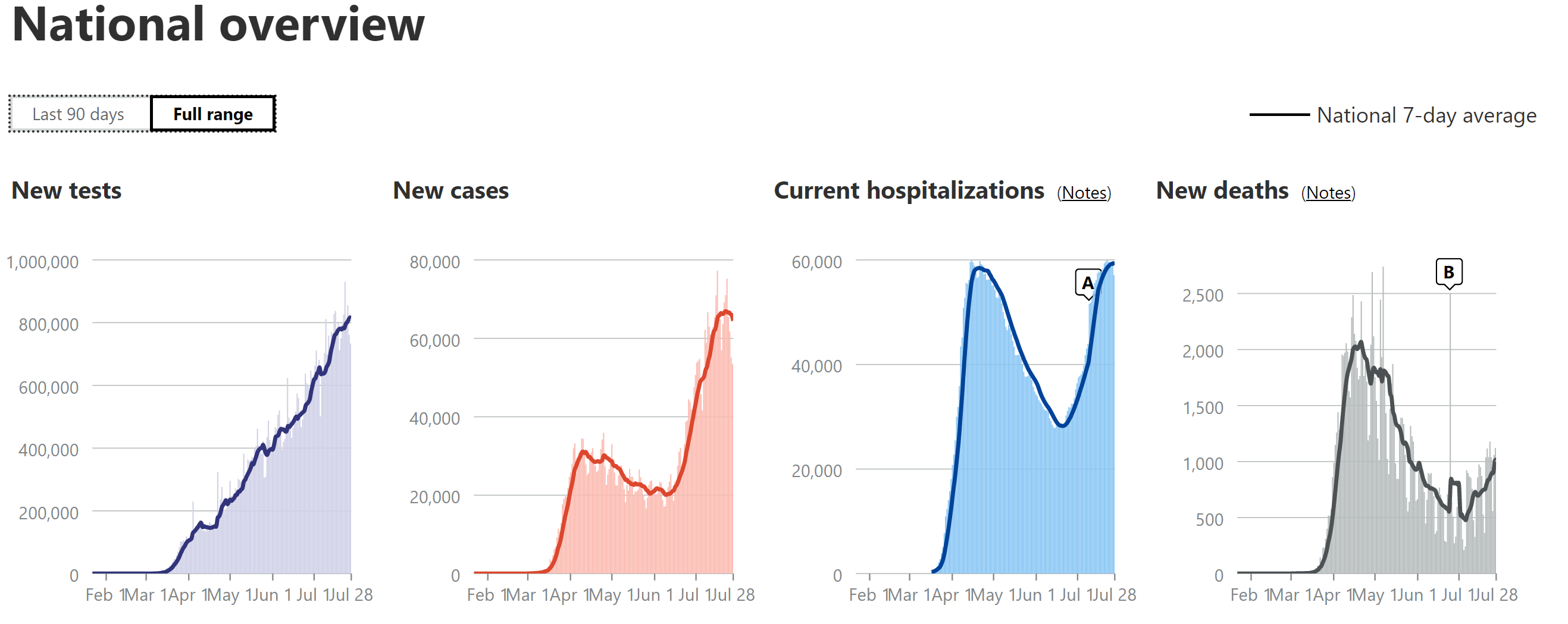
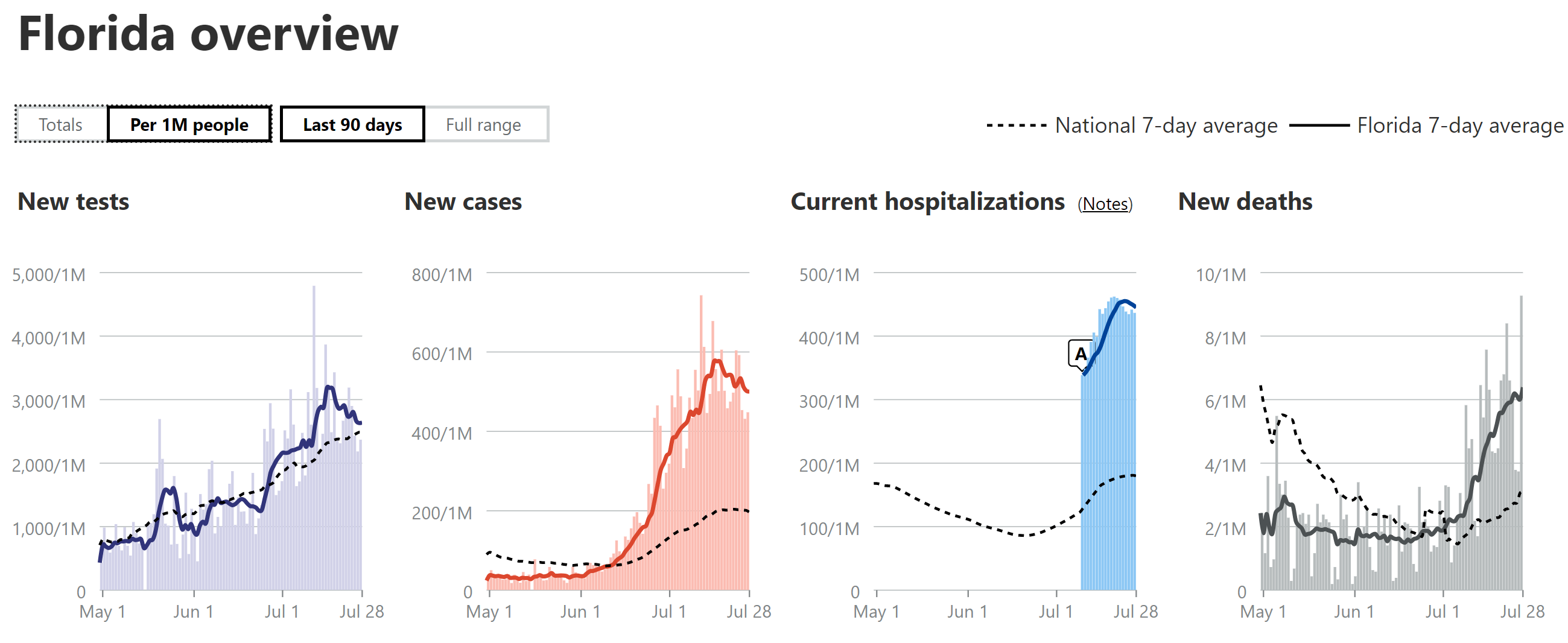
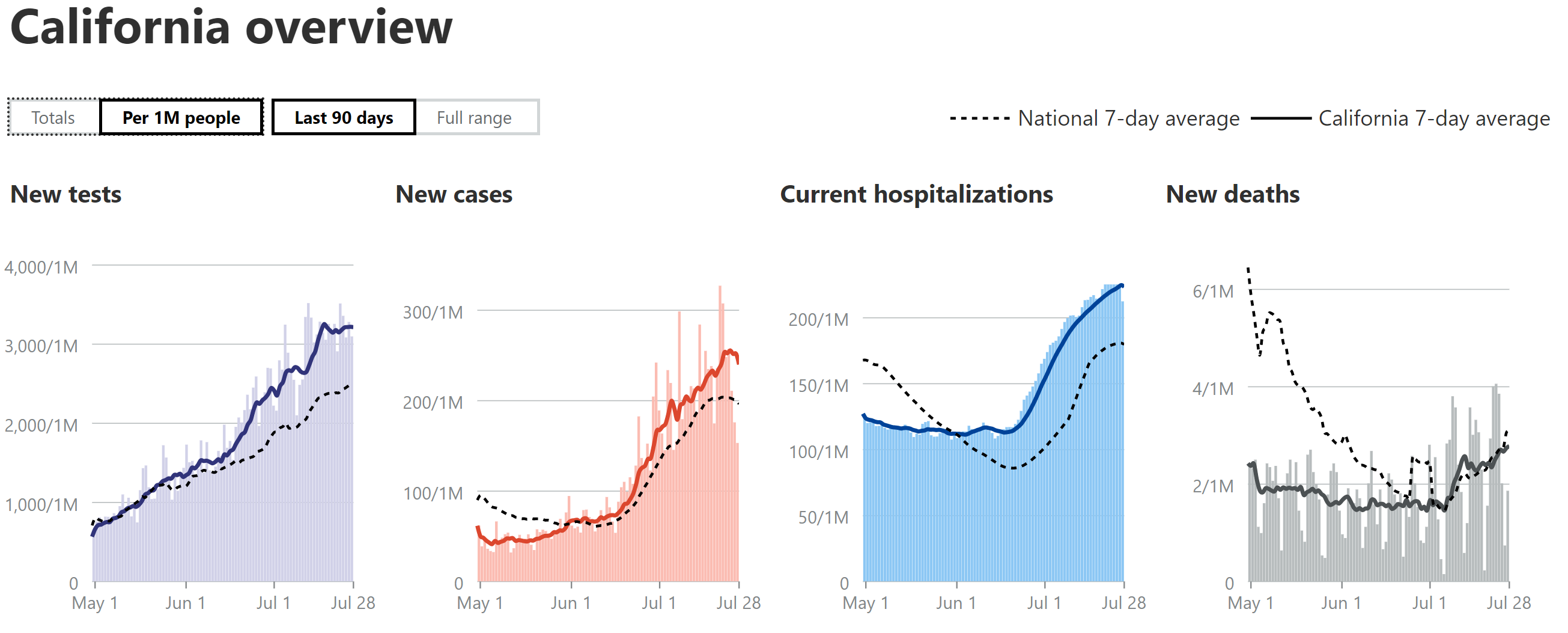
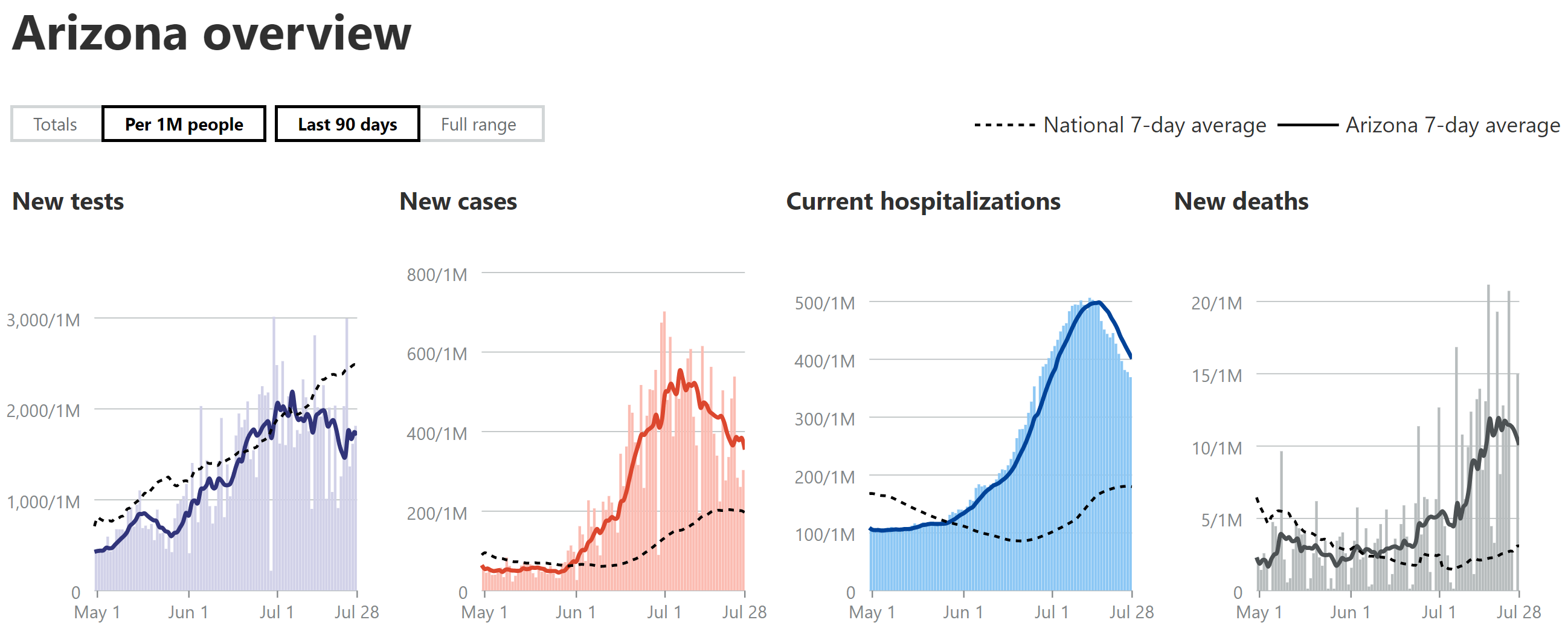
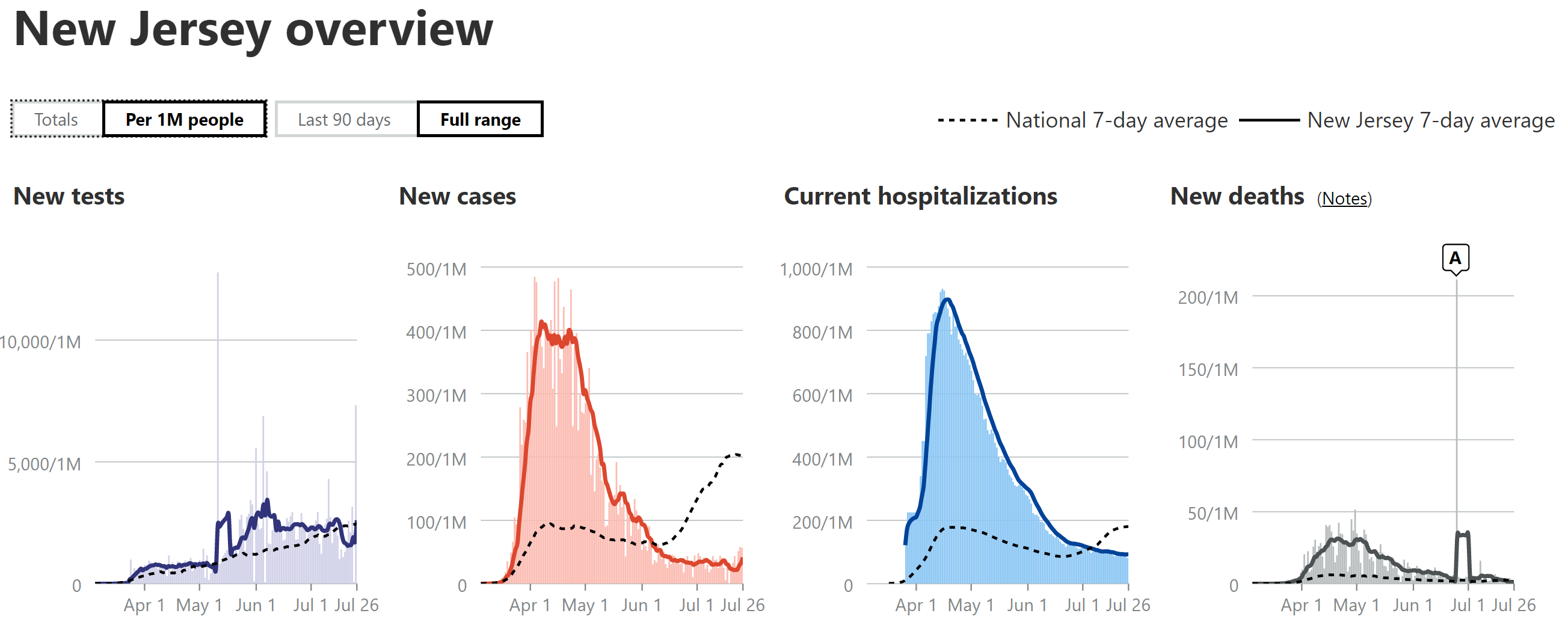
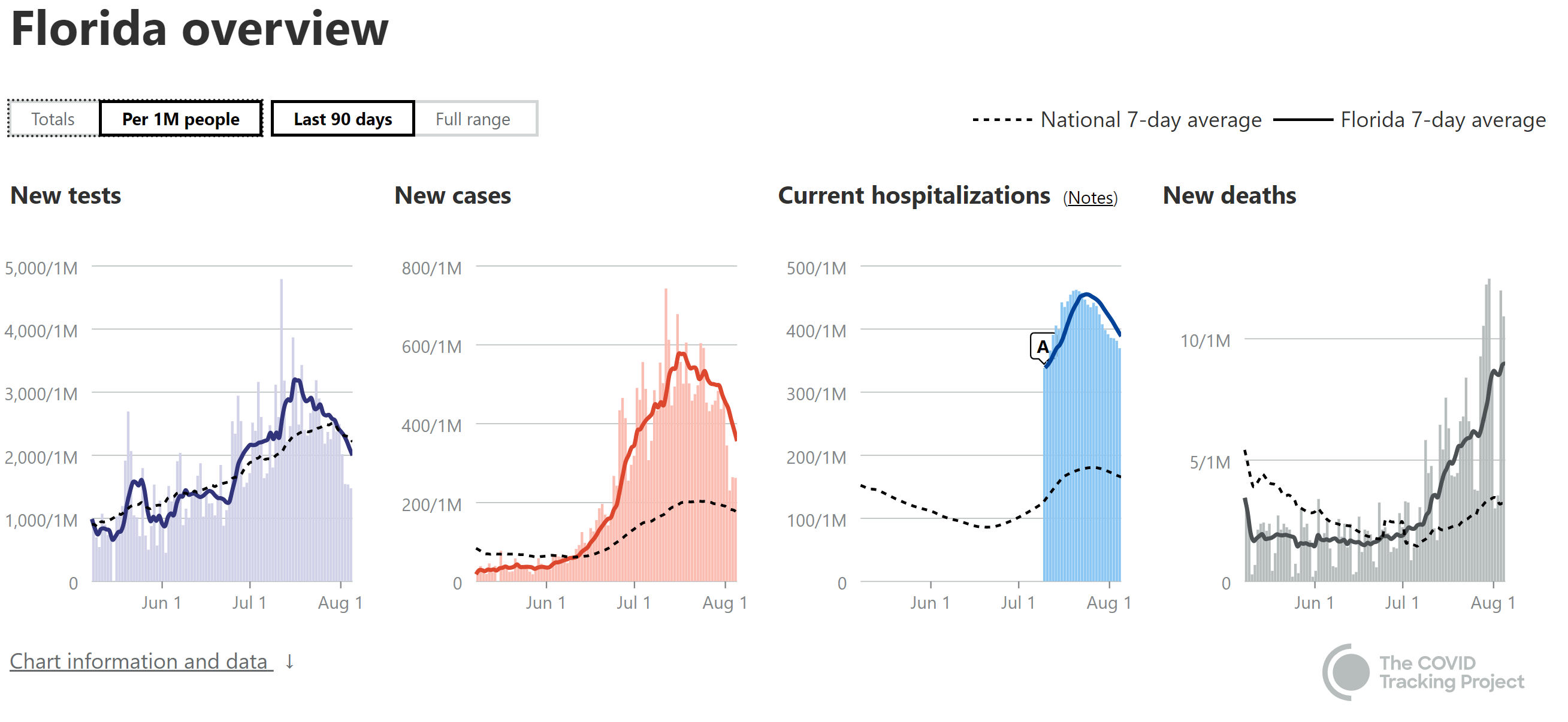
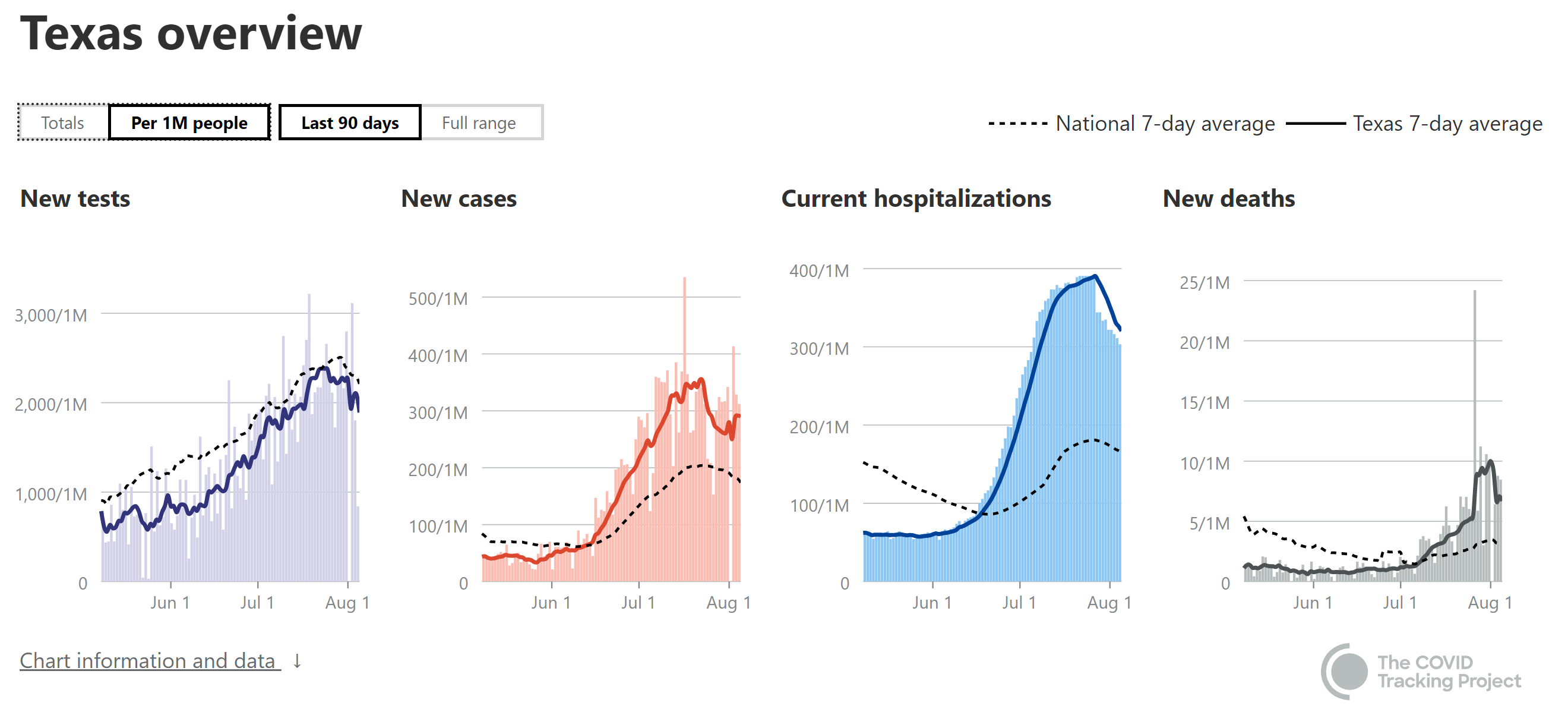
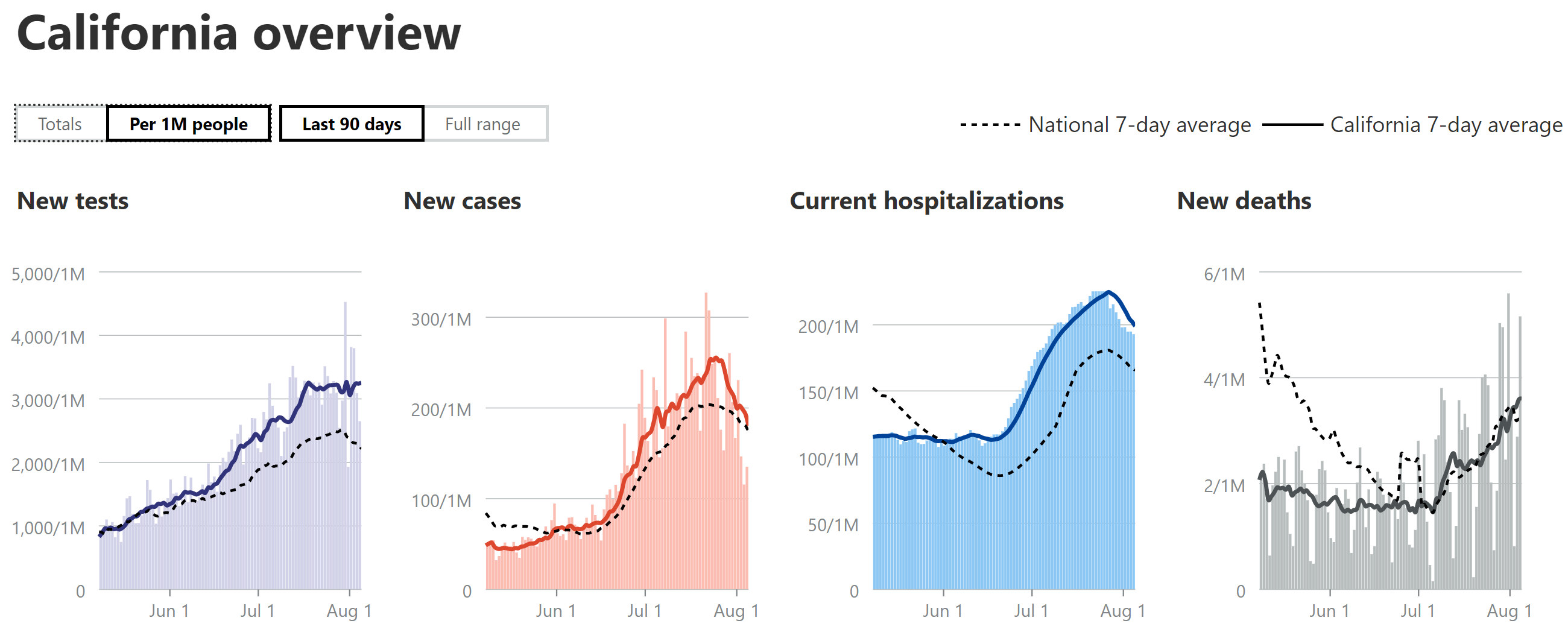
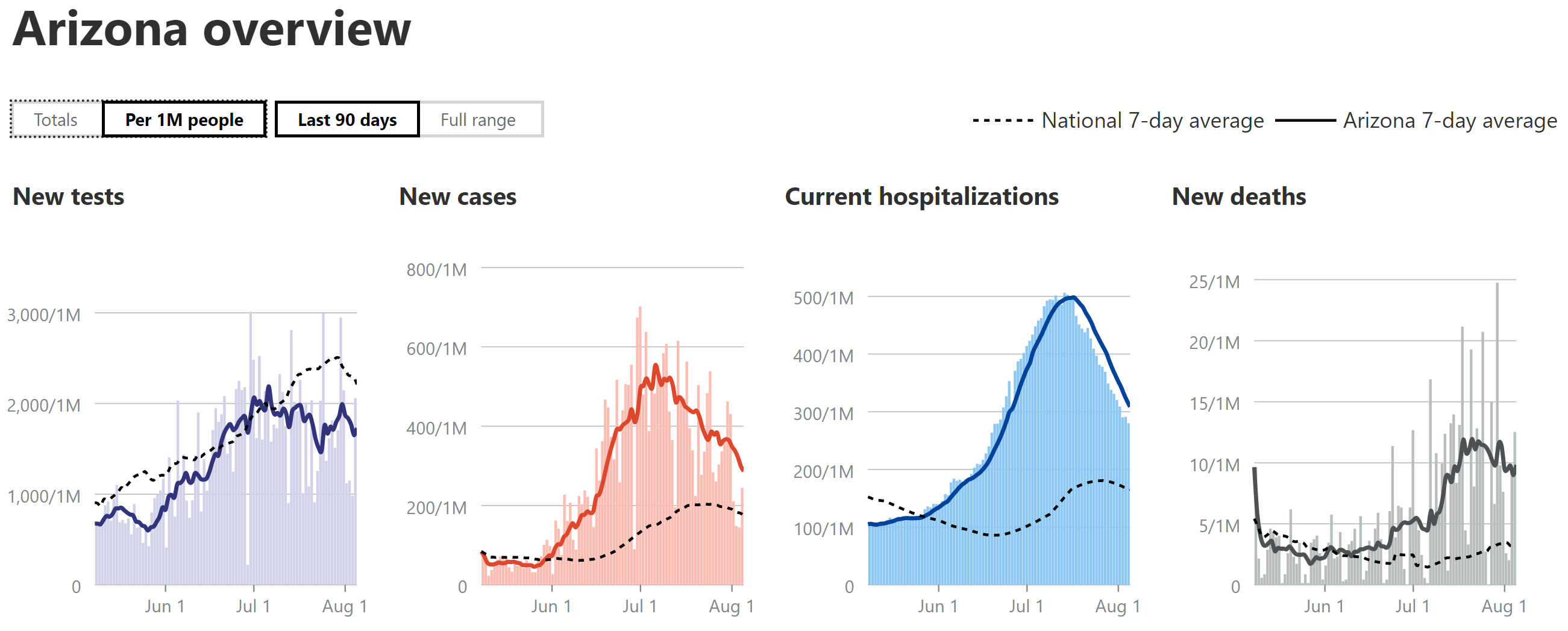
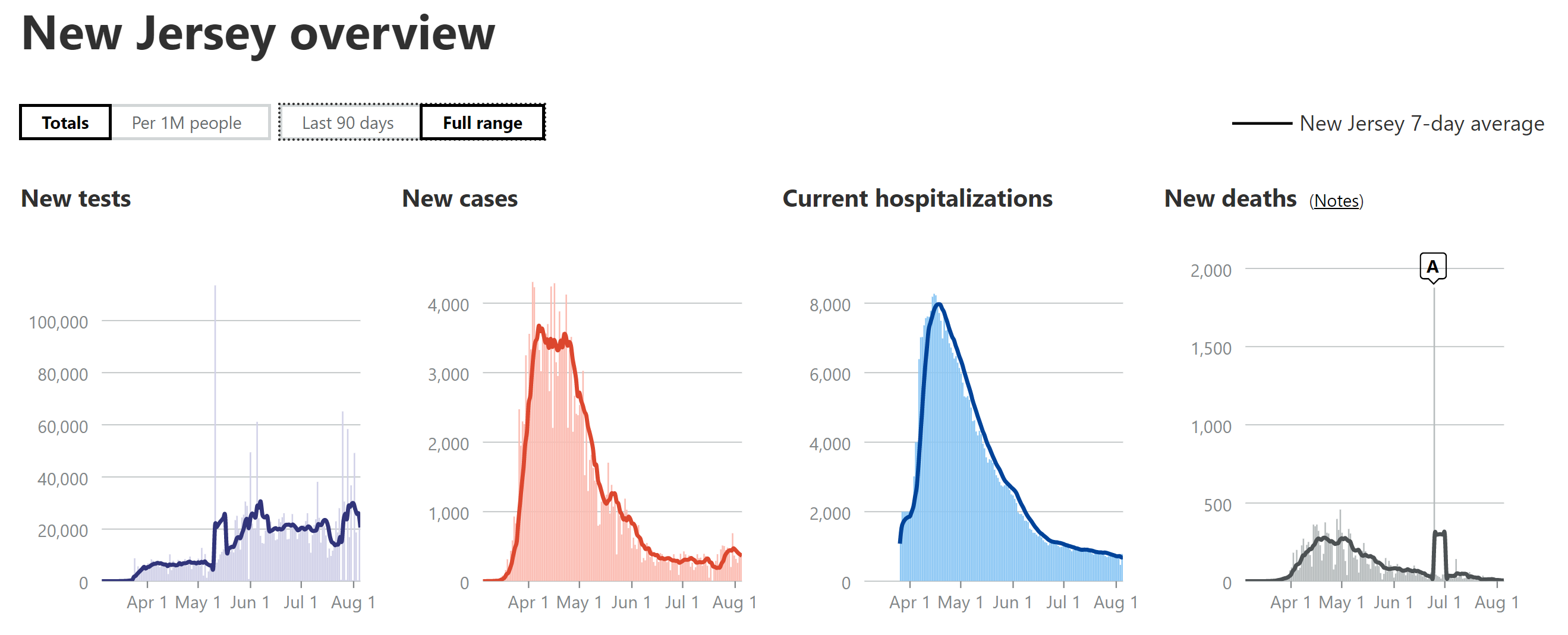
- Cases are clearly declining in AZ and are just starting to decline in FL/TX/CA. The AZ peak was about 30% more, per capita (per 1MM people) than the NJ peak (about 3500/day or 400/1MM) per day or , while the FL peak was ~50% more, the TX peak was ~10% less and the CA peak was ~40% less.
- AZ's hospitalizations peaked (and are declining) at ~55% of NJ's (which were 8000 total or 900 per 1MM), while FL is peaking at about 50% of NJ's per capita rate and TX is peaking at ~45% of NJ's rate, but it's still too early to call the peak for FL/TX yet; CA looks like it's about to peak at maybe 25-30% of NJ's peak. These reductions vs. NJ are likely due to the much younger age of those infected in this wave.
- My guesstimate has been that deaths in AZ/FL/TX would likely be about 1/3-2/3 of the peaks of NJ (about 270-300/day or ~31/1MM); NY's was a little higher), partly due to the younger age of those infected (as above) and partly due to improved treatments and procedures. AZ has likely peaked at ~40% of NJ's peak, but they're having major fluctuations, so hard to call a peak yet. FL and TX are now at 20-25% and 30% of NJ's peak, respectively, and neither has peaked. CA's case/hospitalization rates have been well below the other 3 states and is why CA is only at 10% of NJ's peak and will likely max out at <15% of NJ's peak.
Details - Cases
Still going to try to do this weekly for awhile, as weekly as likely infrequent enough to not be fooled by 1-2 day deviations that aren't that relevant (like the usual weekend dips), but frequent enough to see changes occurring. Let's look at cases first, starting with the national picture, where total cases have definitely now reached a peak (a 2-week plateau, so far) around 65-67K cases per day (7-day avg) which is about twice what the peak in the first wave was (around 31-32K cases/day over a 4-week plateau).
The "good" news is Arizona has clearly peaked in cases and started to decline significantly, while Florida, Texas, and California all appear to be at their peaks and just starting to decline. Many other states could be discussed, but these seemed relevant, as FL/TX/CA are the three most populous states and they're peaking and AZ peaked a bit earlier and has a similar population as NJ, which I'm including as a comparison from the worst of the first wave and since there's so much local interest. It should be noted that AZ peaked ~30% above NJ's peak of ~400/1MM, FL peaked ~50% above NJ's peak, TX peaked ~10% below NJ's peak, and CA peaked about 40% less than NJ's peak (I'm using per capita data for all the graphs, so they're "apples to apples" comparisons).
Details - Hospitalizations
With regard to hospitalizations, on a national level, hospitalizations are just starting to peak and will probably peak just a little bit above what they were in the first wave, despite there being twice as many cases. This was expected several weeks ago, when it became clear that there was a much younger average age of those infected in most states in this current wave (vs. wave 1) and the hospitalization rates in AZ (which had a 1-2 week earlier outbreak than FL/TX/CA) were tracking at about half the rate of NJ's. Note that if COVID were as deadly as it was in the first wave (it's thought to be) one would expect eventual death peaks to mirror relative hospitalization rates, i.e., if a state peaks at 50% of NJ's peak hospitalization rate, one would expect deaths to be around 50%, also (assuming no improved treatments/procedures).
Looking at states, AZ peaked at about 55% of NJ's hospitalization rate, i.e., about 500 per 1MM vs. NJ's 900 per 1MM. FL looks to be peaking at about half of NJ's peak rate, TX is peaking at about 45% of NJ's peak rate, and CA is peaking at about 25-30% of NJ's peak (although still a little early to call these peaks). It's not surprising that CA's case and hospitalization numbers (and likely deaths) are not as bad as the other three states in this comparison, as CA reopened later and after having achieved better reopening metrics, plus CA made masking mandatory on 6/18, just as cases were starting to rise significantly, while the other three states didn't start issuing mask requirements until later and they're not nearly as strong as California's.
Details - Deaths
With respect to deaths, on a national level, they've doubled from the low in early July (500-550/day), as they're now up around 1050/day on a 7-day moving average (with the 600 extra TX deaths factored in), which is almost 50% of the death rate at its peak in April (which was more like a 3-week plateau). Note that the 4 states (FL/TX/CA/AZ) I've been discussing account for about half of that death toll per day, which also means that there are many other states with less people, many of which are also spiking in cases, hospitalizations and deaths. We still don't know where death peaks for these states will end up (or total deaths, since that will also depend on whether a peak is sharp or a plateau and long decline, like NJ had), but my guesstimate has been 1/3-2/3 of the peaks of NJ, partly due to the younger age of those infected (as above) and partly due to improved pharmaceutical treatments (such as remdesivir, dexamethasone, tocilimuzab and convalescent plasma) and improved medical procedures.
With regard to specific states, AZ appears to have peaked at almost 40% of NJ's peak of about 31/1MM (I think, although they're fluctuations are very large, i.e., some are at 60% of NJ's peak, so need to keep an eye on that to be sure they've peaked), which aligns well with my 33-66% guesstimate. FL is now at 20-25% of NJ's peak and still climbing, so it's unclear where they'll end up (especially if they have any large TX-style "adjustments" - today's all-time high peak was at 30% of NJ's peak).
As discussed in the summary, TX had a major "adjustment" made to their death count with ~600 deaths added (all deaths were on death certificates - this looks to be an accounting issue), which the Covidtracking incorporated into their TX death graphic all on today, jacking their 7-day avg up from about 170 to 250 per day (which makes sense as Worldometers is still at about 170/day, as they haven't added the 600 deaths in yet). This brings TX up to about 30% of NJ's peak and TX rate is still climbing, so it seems likely that FL and CA will reach at least 1/3 of NJ's peak level and maybe more. However, CA is only at 10% of NJ's peak death rate per capita and likely won't reach more than 15% of the NJ peak given the lower hospitalization rates (as expected).
Keep in mind that all of these are educated guesses and a big wild card is assuming cases don't go way up amongst the elderly from here on out - they already are increasing in FL and if that continues and also occurs in the other states, these states could easily reach or exceed the upper end of my estimated range of 2/3 the level of NJ's deaths. Hope people find these to be informative - please let me know if any obvious errors (hard to keep all the #'s straight, lol).
https://covidtracking.com/data#chart-annotations